
Abstract
Type 2 diabetes is a progressive disease characterized by decline in β-cell function and insulin resistance. The development of liraglutide, a glucagon-like peptide 1 (GLP-1) receptor agonist, has been shown in clinical trials to be an effective drug with beneficial effects on β-cell function and improved glycemic control, without the side effects of weight gain and hypoglycemia that frequently limit the use of oral anti-diabetic drugs. Furthermore, its prolonged half-life makes it suitable for once daily administration. Liraglutide is demonstrated to be an effective agent in combination with commonly used oral antidiabetic drugs such as metformin and sulphonylureas, with a significant number of patients achieving their glycemic targets without hypoglycemia. In this review, the results from clinical trials utilizing liraglutide in combination with metformin or sulphonylurea are summarized with regards to efficacy and safety.
Keywords
Introduction
Type 2 diabetes mellitus (T2DM) is a progressive disease that is increasing in prevalence all over the world. 366 million adults were predicted to have diabetes in 2011 and this is expected to rise sharply to 552 million by 2030. 1 T2DM accounts for approximately 90% of these cases. 2
The progressive nature of T2DM, characterized by insulin resistance and impaired insulin secretion as a result of impaired β cell function,3–6 leads to chronic hyperglycemia and increased risk of micro- and macro-vascular complications. 7
Good glycemic control has been shown to prevent microvascular complications,8–10 but is known to deteriorate gradually with decline in β-cell function, which poses significant challenges to the health care professional in chronic management of this disease. Current treatment modalities for T2DM include lifestyle modification and pharmacologic therapy. 50% of patients with T2DM will require multiple oral antidiabetic drugs (OAD) within three years 11 after diagnosis, as reported in the United Kingdom Prospective Diabetes Study (UKPDS).
First line pharmacotherapy is typically metformin, which exerts neutral or protective effects on β-cell function and is considered to be weight neutral and possibly cardioprotective. Other well-validated agents include sulphonylureas (SU), thiazolidinediones and insulin, but their use is limited by undesirable side effects such as weight gain and an increased risk of hypoglycemia. 12 Hypoglycemia may actually increase cardiovascular risk in spite of achieving good glycemic control.
The Role of Incretin Mimetics in Type 2 Diabetes
There has been an increasing focus in the use of a relatively new drug class for management of patients with T2DM, made up of incretin mimetics and incretin enhancers. Two naturally occurring gut hormones (peptides) are released into circulation in response to the ingestion of food, being glucose-dependent insulinotropic polypeptide (GIP) and glucagon-like peptide 1 (GLP-1).13,14 As a result of the release of these gut hormones, insulin secretion is greater following oral glucose intake than an intravenous glucose bolus, while similar plasma levels are achieved. This phenomenon is known as the ‘incretin effect’ and may account for 50%-70% of total insulin secretion after food intake, 15 playing a crucial role in the maintenance of glycemic control.
In addition to increasing insulin secretion in a glucose-dependent manner, GLP-1 inhibits glucagon release, restores the first-phase insulin response, decreases gastric emptying16–18 and is shown to improve cardiac, endothelial and β-cell function. 19 In-vitro and animal studies reveal other potential benefits of GLP-1 agonist treatment, such as promotion of β-cell proliferation and reduced β-cell apoptosis. 20 Human GLP-1 is, however, rapidly degraded by dipeptidyl peptidase-4 (DPP-4) with a short half-life of 1.5 minutes therefore limiting its clinical use. 21
Two classes of incretin-based therapies have been developed to overcome the clinical limitations of human GLP-1: GLP-1 receptor agonists (incretin mimetics) and DPP-4 inhibitors (incretin enhancers). 22 GLP-1 receptor agonists (eg, liraglutide and exenatide) are partially resistant to DPP-4 degradation and, therefore, have a longer half-life and prolonged duration of action. 24 DPP-4 inhibitors (eg, sitagliptin, vildagliptin, saxagliptin and linagliptin) inhibit the degradation of native (human) GLP-1 by DPP-4, thereby increasing the levels of GLP-1. 22
Liraglutide, a once-daily subcutaneously administered GLP-1 analogue, has been in use in the UK for over 2 years. It shares 97% amino acid sequence identity with endogenous human GLP-1. Liraglutide has one amino acid substitution (arginine substituted for lysine at position 35) and the addition of a C16 fatty acid chain which prolongs its duration of action to 24 hours, enabling once daily dosing.25,26 The increased half-life (13 hours) is achieved via reversible binding to albumin and increased stability, through heptamer formation mediated by the fatty acid side chain. This makes it suitable as a once-daily injectable treatment for people with T2DM,24,27 as an adjunct to lifestyle therapy and in combination with oral antidiabetic drugs.
The glucoregulatory effects of liraglutide appear to mimic human GLP-1 and enhance glucose-dependent insulin secretion, inhibition of postprandial glucagon secretion, inhibition of gastric emptying and reduction of food intake. Studies using animal models (diabetic mice and rats) and in vitro studies have shown that liraglutide stimulates an increase in β-cell proliferation/mass, and a reduction in β-cell apoptosis. 20 The beneficial effects of liraglutide on appetite, calorie intake and weight make it a suitable alternative for combination therapy in patients with T2DM who are typically overweight or obese.
In addition to its hypoglycemic effects, liraglutide also appears to have a positive impact on the cardiovascular system. In-vitro trials show that liraglutide attenuates plasminogen activator inhibitor (PAI-1) and vascular cell adhesion molecule induction, which are caused by hyperglycemia and stimulation of tumor necrosis factor alpha (TNF-α) in vascular endothelial cells. 19 These effects of liraglutide on the vascular endothelium appear to be independent of glycemic control. 28
Clinical Trials
The earliest clinical study looking at the effects of escalating doses of liraglutide in combination with metformin was a randomized double-blind placebo-controlled study by Nauck and colleagues. 29 144 patients with T2DM (baseline HbA1c ~9.4%) on metformin treatment (1000 mg twice a day) were randomized to 5 weeks of treatment with liraglutide plus metformin, liraglutide only, metformin only, or metformin plus glimepiride. The dose of liraglutide was increased by 0.5 mg increments every week to a maximum of 2 mg OD. The addition of liraglutide to metformin resulted in a further reduction in FPG (3.9 mmol/L) as compared to metformin mono-therapy, and was accompanied by a 0.8% reduction in HbA1c. Body weight was significantly lower with metformin plus liraglutide than with metformin plus glimepiride even after only 5 weeks (-2.9 kg).
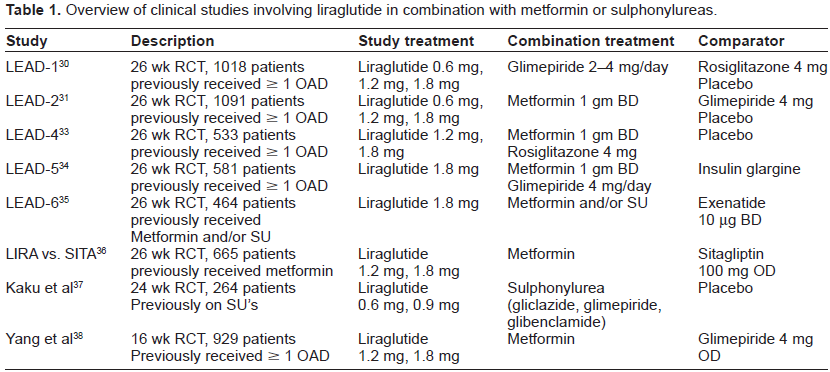
The efficacy and safety of liraglutide has been investigated in the extensive phase 3 Liraglutide Effect and Action in Diabetes (LEAD) program.30–35 This consisted of six randomized controlled trials involving 4,456 patients with T2DM recruited from more than 600 sites in 40 countries. The LEAD studies were designed to investigate the effects of liraglutide as monotherapy 32 or in combination with commonly prescribed glucose lowering therapies (oral anti-diabetic drugs) compared with standard diabetes treatments. The most common combination of liraglutide in these trials was with single oral anti-diabetic drugs such as metformin or sulphonylureas, or with 2 OADs such as metformin and thiazolidinediones or metformin and a sulphonylurea. The LEAD-6 trial 35 studied the effects of liraglutide in combination with metformin or/and a sulphonylurea. Three other studies looked at the efficacy and safety of liraglutide in combination therapy-1) liraglutide versus sitagliptin both in combination with metformin, 36 2)liraglutide versus placebo both added to a sulphonylurea in Japanese patients with T2DM 37 and 3) liraglutide versus glimepiride, both in combination with metformin in Asian patients (China, Korea and India) with T2DM. 38
Study Measurements
All the clinical trials conducted above assessed the efficacy of liraglutide with the primary end-point being change from baseline HbA1c. Secondary end-points included percentages of patients reaching HbA1c of < 7.0% (American Diabetes Association target), fasting plasma glucose (FPG), post-prandial plasma glucose (PPG), changes in body weight, indices of pancreatic β-cell function (proinsulin-to-insulin ratio and homeostasis model assessment (HOMA-B), HOMA-insulin resistance (HOMA-IR) and blood pressure (BP).
Safety variables included hypoglycemic episodes based on plasma glucose levels, liraglutide antibodies, tolerability (gastrointestinal complaints) and pulse. Adverse effects, vital signs, electrocardiogram (ECG), biochemical and hematology measures including calcitonin were also measured.
Combination Treatments
Glycemic control Combination of liraglutide with metformin
The LEAD-2 trial was a 26-week placebo-controlled study of 1,091 patients with T2DM (baseline HbA1c ~8.4%) evaluating the efficacy and safety of liraglutide in combination with metformin compared with glimepiride in combination with metformin, or a placebo of metformin monotherapy. Patients were randomized to receive liraglutide (0.6, 1.2 and 1.8 mg/day), glimepiride (4 mg/day), or placebo (metformin 1 gm twice daily). 31 Glycemic control after 26 weeks with liraglutide was superior to placebo (HbA1c decreased on average by -0.7%, -1.0%, -1.0% for 0.6, 1.2 and 1.8 mg doses of liraglutide respectively). The higher doses of liraglutide appeared to be similar in efficacy to glimepiride (-1.0%). The reductions in HbA1c occurred within 8-12 weeks for the 1.2 and 1.8 mg doses of liraglutide and were maintained over 26 weeks.
Following 26 weeks of treatment, 42% of subjects treated with liraglutide 1.8 mg and 36% on glimepiride reached a target HbA1c of <7% compared to placebo (11%). Fasting plasma glucose (FPG) was reduced in all active treatment arms (liraglutide and glimepiride) to a similar extent (-1.1 to -1.7 mmol/L versus +0.4 mmol/L for placebo). Post-prandial glucose (PPG) decreased from baseline in all treatment groups compared with placebo with 1.2 and 1.8 mg doses of liraglutide (-2.3 and -2.6 mmol/L) and glimepiride (-2.5 mmol/L).
A similar study conducted by Yang and colleagues 38 compared the effects of liraglutide with glimepiride, both in combination with metformin for the treatment of T2DM (baseline HbA1c 8.6%) in Asian populations form China, South Korea and India. 929 subjects were randomized to receive liraglutide (0.6, 1.2 and 1.8 mg) or glimepiride 4 mg once daily, each in combination with metformin, over a period of 16 weeks.
HbA1c was significantly reduced in all groups compared to baseline, with similar results to the LEAD-2 study. Treatment with the higher doses of liraglutide (1.2 and 1.8 mg) was non-inferior to glimepiride (mean HbA1c reduction 1.36%, 1.45% and 1.39% respectively). 43% and 45% of liraglutide subjects (on 1.2 and 1.8 mg) attained a target HbA1c of <7%, which was comparable to the glimepiride group (44%). Changes in FPG in the patients on liraglutide 1.2 mg (-2.05 mmol/L) and 1.8 mg (-2.12 mmol/L) were comparable to those of the glimepiride group (-2.18 mmol/L). The 1.8 mg dose of liraglutide showed greater PPG decrease (-3.51 mmol/L) in contrast with glimepiride (-2.60 mmol/L), with the lower doses eliciting changes comparable to glimepiride.
The LIRA-DPP-4 study evaluated the efficacy and safety of liraglutide compared with the DPP-4 inhibitor sitagliptin, each added to metformin over 52 weeks in individuals with T2DM (baseline HbA1c 8.4%). 36 In this randomized controlled trial, 665 patients on metformin were randomized to receive liraglutide (1.2 and 1.8 mg once a day) or sitagliptin 100 mg once a day for 26 weeks followed by an extension phase of 26 weeks.
Liraglutide (1.2 mg or 1.8 mg) showed superior HbA1c (-1.29% and -1.51%) reduction compared with sitagliptin (-0.88%). FPG was significantly decreased in patients treated with liraglutide (-2.14 mmol/L with 1.8 mg and -1.87 mmol/L with 1.2 mg) compared with sitagliptin (-0.83 mmol/L).
Combination of liraglutide with metformin and thiazolidinedione
The LEAD-4 trial was a 26-week placebo-controlled study in 533 patients that investigated the effects of adding liraglutide (1.2 and 1.8 mg) to the treatment plan of patients with T2DM (baseline HbA1c 8.3%) whose T2DM was inadequately controlled on two oral antidiabetic drugs (metformin 1 gm twice a day and rosiglitazone 8 mg/day). 33 Effective reduction in HbA1c was seen with liraglutide (-1.5% vs. -0.54% for placebo). 58% and 54% of patients on liraglutide 1.2 mg and 1.8 mg respectively achieved a target HbA1c of < 7%, in contrast to 28% with placebo. The addition of liraglutide also lead to reductions in FPG (-2.2 to -2.4 mmol/L) and PPG (-2.6 to -2.7 mmol/L) in contrast to placebo (0.4 to 0.8 mmol/L; P < 0.001).
Combination of liraglutide with metformin and/or sulphonylurea
The LEAD-5 study examined the effect of adding liraglutide (1.8 mg once daily) to metformin (1 g twice daily) plus glimepiride (2-4 mg/day) in 581 patients with T2DM (baseline HbA1c 8.2%). 34 The trial was placebo-controlled with insulin glargine used as an active comparator (open label). After 26 weeks, the HbA1c reduction from baseline was 1.33% with liraglutide, 1.09% with insulin glargine and 0.24% with placebo. 52% of patients on liraglutide reached a target HbA1c of <7%, compared to 44% with insulin glargine and 15% with placebo. Both active treatments reduced FPG to a similar degree in contrast to placebo, which showed a mild increase (+0.6 mmol/L). Likewise, the reduction in PPG from baseline was comparable between liraglutide and insulin glargine.
The LEAD-6 trial looked at the efficacy and safety of adding liraglutide (1.8 mg) in comparison to another GLP-1 analogue (exenatide 10 Lig twice a day) in 464 patients with T2DM who had inadequate glycemic control (baseline HbA1c 8.2%) with maximally tolerated doses of metformin, sulphonylureas or both. 35 In this study, there was a greater reduction in HbA1c with liraglutide in contrast with exenatide (1.12% versus 0.79%) at the end of 26 weeks of treatment. 54% of patients on liraglutide versus 43% on exenatide reached a target HbA1c of <7%, with significantly greater reduction in FPG (-1.61 mmol/L versus -0.60 mmol/L).
Combination of liraglutide with sulphonylurea
The LEAD-1 trial was a 26-week placebo-controlled study of 1,041 patients with T2DM on a baseline treatment of a sulphonylurea (glimepiride : 2-4mg/day) where the efficacy of liraglutide in 3 different doses (0.6, 1.2 and 1.8 mg once daily) was compared with rosiglitazone (4 mg/day) as an-add on therapy to glimepiride and placebo (glimepiride monotherapy). 30 There was a significant decrease in HbA1c with all 3 doses of liraglutide in combination with glimepiride as compared to placebo. The 1.2 and 1.8 mg doses of liraglutide resulted in superior HbA1c reduction (-1.08% and -1.13% respectively) compared with rosiglitazone. Combining rosiglitazone or liraglutide (0.6 mg) with glimepiride showed similar efficacy in HbA1c reduction (-0.44% and -0.60% respectively). Following 26 weeks of treatment, 42% of subjects treated with 1.8 mg of liraglutide reached an HbA1c < 7.0% compared with 8% for placebo therapy.
A reduction in FPG was observed with both liraglutide and rosiglitazone combinations, compared to placebo, but with no significant differences between the active treatments arms (reductions of -0.7 to -1.6 mmol/L).
A Japanese randomized controlled study by Kaku and colleagues 37 examined the effects of liraglutide in 264 subjects with T2DM (mean HbA1c: 8.4%) who were randomized to receive 0.6 mg or 0.9 mg of liraglutide, each added to sulphonylurea monotherapy (glibenclamide, gliclazide or glimepiride) over a duration of 24 weeks.
HbA1c levels were significantly reduced and sustained with both liraglutide doses (P < 0.001). The mean change in HbA1c was -1.56% and -1.46% with liraglutide 0.9 and 0.6 mg respectively, and -0.40% with placebo. More subjects reached a HbA1c of < 7% with liraglutide (0.6 mg: 46.5%; 0.9 mg: 71.3% versus placebo (14.8%). A significant reduction in FPG was seen with liraglutide (-1.47 mmol/L and -1.8 mmol/L with 0.6 mg and 0.9 mg versus placebo; P < 0.0001).
The LEAD-1 30 and LEAD-2 31 studies as well as the study by Yang and colleagues 38 demonstrated that liraglutide, in combination with a sulphonylurea or metformin, showed a superior reduction in HbA1c in patients previously on monotherapy compared to combination therapy.30,31 This finding may, however, be attributed to the study design of these trials, as patients were not necessarily on the oral antidiabetic medication used in the study prior to enrolment. Therefore, the effect of the medication used in combination and that of liraglutide is difficult to assess.
Overview of clinical studies involving liraglutide in combination with metformin or sulphonylureas.
Body Weight
Treatment with liraglutide results in sustained weight loss as compared to placebo. The weight loss tends to be dose-dependent, both as monotherapy and in combination regimens. This phenomenon was observed in the LEAD studies,30–35 the LIRA-DPP4 study, 36 and the study by Yang and colleagues, 38 but not in the LEAD-1 study. 30 In LEAD-1 (liraglutide vs. rosiglitazone in combination with sulphonylurea), weight gain was noted with liraglutide (0.6 mg: 0.7 kg, 1.2 mg: 0.3 kg) and rosiglitazone (2.1 kg). A modest reduction of 0.2 kg was observed with the 1.8 mg dose of liraglutide. The addition of liraglutide 1.2 and 1.8 mg to metformin led to a weight loss of between 2.6 and 2.8 kg, in contrast to the 1.0 kg weight gain observed for glimepiride. 31
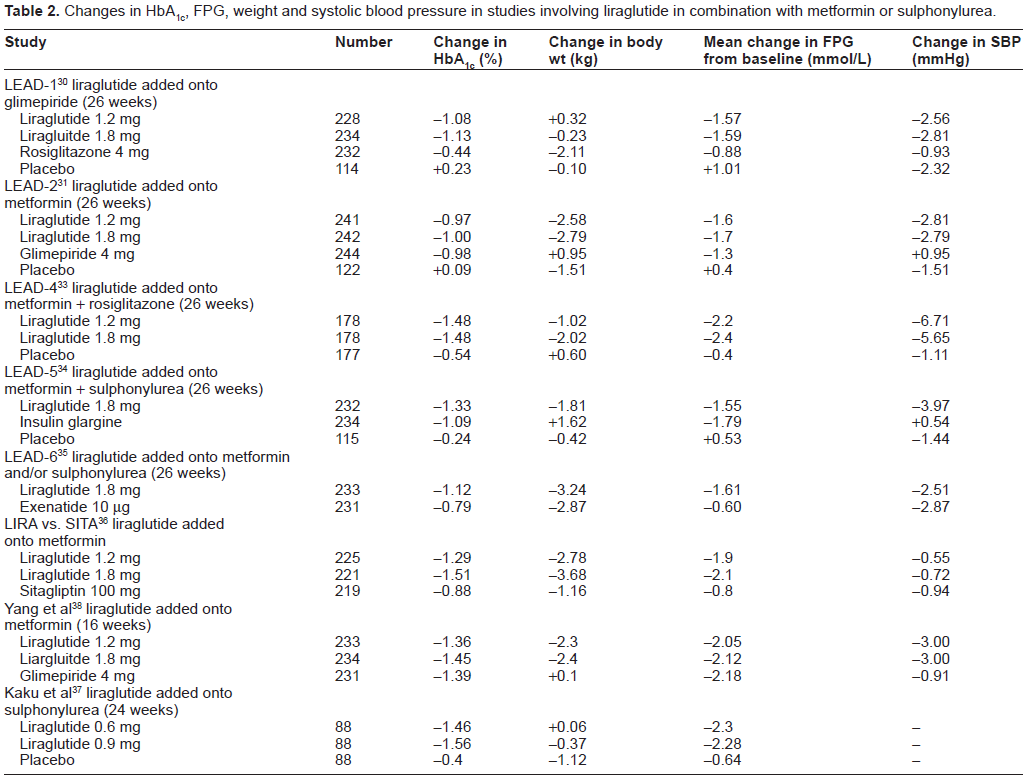
The effect on body weight reported for liraglutide 1.8 mg plus glimepiride was significantly better than that observed for rosiglitazone (P < 0.0001; Table 2). Liraglutide treatment with metformin (LEAD-2) 31 or metformin plus rosiglitazone (LEAD-4) 33 showed significant weight loss that was apparent at 8 weeks of treatment, and these results are consistent with 2-year data from the LEAD-2 trial. The weight loss observed for liraglutide in combination with metformin mono-or combination therapy may reflect the fact that metformin is weight neutral. In contrast, glimepiride has been associated with weight gain, which may counterbalance the weight benefit of liraglutide. Liraglutide (1.8 mg) caused significant reduction in weight, in contrast to insulin glargine, which was associated with weight gain when combined with metformin and a sulphonylurea. 34 No significant weight reduction was observed by Kaku and colleagues 37 in the Japanese population who received smaller doses of liraglutide (0.6 mg, 0.9 mg) in combination with sulphonylurea despite a significant improvement in glycemic control. This might be attributed to the lower BMI (24-26) in this population compared to the Caucasian population with T2DM, as well as the predominant pathology of β-cell dysfunction rather than insulin resistance.
Changes in HbA1c, FPG, weight and systolic blood pressure in studies involving liraglutide in combination with metformin or sulphonylurea.
β-Cell Function
Liraglutide treatment has beneficial effects on markers of β-cell function in patients with T2DM. These effects, as measured by HOMA-B, on the proinsulin-to-insulin ratio have been observed across all the LEAD trials. With liraglutide (1.2 mg and 1.8 mg) in combination with glimepiride, 30 HOMA-B increased significantly compared with glimepiride plus rosiglitazone. Improvements of 62%-71% in HOMA-B were reported from baseline values of 40%-47% in all liraglutide treatment groups in combination with metformin. In the LEAD-2 study, 31 when liraglutide was added to metformin, HOMA-B increased to the same extent as with glimepiride (68%) with no improvement in the placebo group. A head-to-head trial of liraglutide (1.2 mg, 1.8 mg) with sitagliptin (100 mg) in combination with metformin 36 showed a significant improvement in HOMA-B as opposed to sitagliptin (treatment difference: 18.6 and 21.77; P < 0.001).
Improvements in HOMA-B were also seen with liraglutide 1.8 mg in combination with 2 OADs (including metformin and rosiglitazone) with an increase of 28% from baseline, compared to a 5.8% increase from baseline with placebo in combination with rosiglitazone and metformin (P < 0.0001). 33
Dose-dependent reductions in the proinsulin-to-insulin ratio have been observed with liraglutide treatment combined with sulphonylurea or metformin. These changes were demonstrated with liraglutide (1.2 and 1.8 mg) in combination with glimepiride, which was significantly greater than with glimepiride or placebo. 30
Cardiovascular Risk
Systolic blood pressure
Addressing blood pressure control remains one of the key challenges, especially in the context of T2DM, which is an independent risk factor for cardiovascular disease. Most of the LEAD studies and trials by Yang and colleagues showed these effects early (2 weeks) following initiation of liraglutide 1.2 and 1.8 mg treatment.30–35,38 There were substantial reductions in systolic BP up to 6.7 mm and 5.6 mm of Hg respectively, in combination with metformin and thiazolidinedione. 33 The observed reductions in systolic blood pressure (SBP) were consistently maintained for the duration of the trial, and were statistically significant compared with baseline blood pressure at all time points. The reductions in blood pressure appear to be independent of weight, with consistent reduction in SBP but no significant change in diastolic blood pressure (DBP).
Safety and Tolerability
Liraglutide was generally well tolerated in all trials of liraglutide in combination with metformin or sulphonylurea. The most common adverse events were gastrointestinal in nature (nausea, vomiting and diarrhea). The proportion of patients experiencing nausea was dose-dependent for patients on liraglutide (1.2 mg and 1.8 mg). However, the majority of these side effects were transient, with nausea being reported by 6.8%-40%,30–37 gradually decreasing within 2 to 4 weeks of treatment. 39
Diarrhea was reported by 8%-19% of subjects,30–37 and appeared to be increased in combination with metformin in the LEAD-2 study, 31 as compared with 4% of patients in the placebo and glimepiride treatment arms.
Hypoglycemia
Liraglutide mimics the action of human GLP-1 in a glucose-dependent manner. Therefore, the incidence of hypoglycemic events are rare when used as monotherapy. This was demonstrated in earlier clinical studies, with liraglutide showing no impairment of glucagon response during hypoglycemia or hypoglycemia counterregulation. 40 The frequency of hypoglycemia varies depending on its combination with metformin, sulphonylurea or with 2 OADs.
In the LEAD studies, hypoglycemic events were classified as either major (subject unable to resolve with self-treatment) or minor (symptoms plus a plasma glucose less than 56 mg/dL or 3.1 mmol/l).30–35 Researchers measured the rate of hypoglycemic events as a function of A1c values after 26 weeks of treatment. Few minor and major hypoglycemic episodes have been reported with liraglutide across the LEAD studies. None of the major episodes resulted in coma or seizures.
Liraglutide as monotherapy was noted to be safe with no reports of major hypoglycemic events, and only 12% and 8% of patients on liraglutide 1.2 mg and 1.8 mg respectively reported minor hypoglycemia compared with 24% in the glimepiride group. 32 The rate of minor hypoglycemia was significantly lower (P < 0.0001) for both liraglutide treatment groups (0.30 and 0.25 events per year for liraglutide 1.2 mg and 1.8 mg respectively, compared with 1.96 events per year for glimepiride).
The rate of minor hypoglycemia reported by patients treated with liraglutide in combination with metformin in the LEAD-2 trial was comparable to placebo (~3% of subjects in either group versus 17% in the glimepiride group) resulting in a relatively low rate of minor hypoglycemia (0.03-0.14 events/year for the placebo and liraglutide groups and 1.23 events/year for the glimepiride group). 31 This indicates that liraglutide can be safely used in this combination. This assumption is further supported by the LEAD-6 trial, 35 which reported no major episode of hypoglycemia in patients who began taking liraglutide in combination with either metformin and/or sulphonylurea. Patients receiving metformin as background therapy were noted to have fewer minor hypoglycemic episodes (6%) than those taking a sulphonylurea with or without metformin (33%). Liraglutide was associated with a 10-fold lower incidence of minor hypoglycemia (0 to 0.091 events per subject year) than glimepiride (1.16 events per subject year) when used in combination with metformin. 38
However, the combination of liraglutide (1.8 mg) and a sulphonylurea might predispose patients to an increased risk of hypoglycemia, as there were 6 reported cases of major hypoglycemia.30,34 These cases may be attributed to uncoupling of glucose-dependent insulin secretion of GLP-1 when combined with a sulphonylurea. 41 In the LEAD-1 study, 30 one major hypoglycemic episode was reported (self measured blood glucose = 3.0 mmol/L), which occurred 9 days after treatment in a subject started on liraglutide 1.8 mg in combination with glimepiride, who required third party assistance. The hypoglycemia was attributed to the glimepiride, with subsequent dose reduction from 4 mg to 3 mg after the incident. A higher proportion of patients on liraglutide 1.2 mg (9.2%) and 1.8 mg (8.1%) in combination with glimepiride experienced minor hypoglycemia, which was significantly greater than the patients on rosiglitazone in combination with glimepiride (4.3%).
When liraglutide was used in combination with metformin and glimepiride, 34 five patients reported major hypoglycemia with one patient requiring medical assistance. A similar effect was not seen in the LEAD-4 study, 33 when liraglutide was used in combination with metformin and rosiglitazone. This phenomenon of increased hypoglycemic risk in combination with a sulphonylurea has also been reported with exenatide. 42
Summary
Liraglutide is a GLP-1 mimetic and has been in clinical use for over two years. Due to its prolonged half-life, it can be administered as a once-daily subcutaneous injection. It is known to be effective as monotherapy, 32 although it has only been licensed to be used in combination with other validated core therapies such as metformin, sulphonylurea and thiazolidinediones. It is a safe and effective option for treatment of patients with T2DM early in the course of disease, and would be useful as mono-therapy in patients who are intolerant to metformin or sulphonylureas, or in patients who would benefit from weight loss. Pharmacokinetic data supports its use in patients with moderate to severe renal impairment, 43 but liraglutide is only licensed in the UK for patients with mild renal impairment. Additional trials in patients with renal impairment are ongoing.
The antihyperglycemic efficiency associated with liraglutide (1.2 and 1.8 mg) doses have been demonstrated in combination therapy with metformin or sulphonylurea, with improvement in β-cell function, as measured by HOMA-B and the proinsulin-to-insulin ratio.
A consistent reduction in HbA1c of up to 1.6% has been seen across the LEAD trials, which persisted at the end of one year. This improvement in glycemic control is accompanied by minimal or no side effects of hypoglycemia in combination with metformin, whilst reported cases of hypoglycemia in combination with sulphonylureas have generally been attributed to sulphonylureas.
One of the biggest advantages of liraglutide therapy is the significant weight loss it appears to cause, in contrast to other antihyperglycemic therapies. This advantage makes it a suitable agent of the pharmacotherapy armamentarium for the management of patients with T2DM. Furthermore, liraglutide was found to be associated with a reduction in systolic blood pressure, which may be beneficial in reducing cardiovascular risk.
Liraglutide appears to be generally well tolerated, as demonstrated in studies of combination therapy with metformin and sulphonylurea. Nausea was the most common adverse effect identified followed by diarrhea, although these were mild and transient with easing of symptoms after 4 weeks of treatment.
Liraglutide appears to address most of the key challenges that a physician is faced with in the management of overweight or obese individuals with T2DM, and its effects have been supported in combination with metformin or a sulphonylurea.
Funding sources
Author(s) disclose no funding sources.
Competing Interests
SCB and/or his institution have received consulting fees from Novo Nordisk, Eli Lilly, Boehringer Ingelheim, AstraZeneca, BMS, GlaxoSmithKline, Takeda, MSD, Sanofi-Aventis and payment for lecturing or speaking from Boehringer Ingelheim, Eli Lilly, GlaxoSmithKline, MSD, Novartis, Novo Nordisk, Pfizer, Sanofi-Aventis, Servier, Takeda and payment for development of educational presentations from Doctors.net, Onmedica, Cardiff University. MVU discloses no potential competing interests.
Author Contributions
Conceived and designed the experiments: MVU. Analysed the data: MVU, SCB. Wrote the first draft of the manuscript: MVU. Contributed to the writing of the manuscript: MVU, SCB. Agree with the manuscript results and conclusions: MVU, SCB. Jointly developed the structure and arguments for the paper: MVU, SCB. Made critical revisions and approved final version: MVU, SCB. All authors reviewed and approved of the final manuscript
Disclosures and Ethics
As a requirement of publication author(s) have provided to the publisher signed confirmation of compliance with legal and ethical obligations including but not limited to the following: authorship and contributorship, conflicts of interest, privacy and confidentiality and (where applicable) protection of human and animal research subjects. The authors have read and confirmed their agreement with the ICMJE authorship and conflict of interest criteria. The authors have also confirmed that this article is unique and not under consideration or published in any other publication, and that they have permission from rights holders to reproduce any copyrighted material. Any disclosures are made in this section. The external blind peer reviewers report no conflicts of interest. Provenance: the authors were invited to submit this paper.