
Abstract
Background
In patients with chronic myeloid leukemia subjected to allogeneic hematopoietic stem cell transplant, the possible negative impact of imatinib therapy in the pre-transplant period is still controversial.
Methods and materials
A retrospective study of patients with chronic myeloid leukemia who received allogeneic hematopoietic stem cell transplant between January 2004 and December 2006 at King Faisal Specialist Hospital and Research Centre in Riyadh was conducted. The results of patients who received hydroxyurea or interferon-α (group A) prior to transplant were compared with those of patients who received imatinib therapy (group B). Both groups of patients received the same conditioning therapy and graft versus host disease prophylaxis.
Results
Survival was shorter and mortality rate was higher in group B compared to group A patients. Both acute and chronic graft versus host disease were not only more frequent but also more severe and extensive in group B. Viral, bacterial and fungal infections were more predominant and more serious in group B compared to group A.
Conclusions
In patients with chronic myeloid leukemia who are subjected to hematopoietic stem cell transplant, prior therapy with imatinib mesylate may have an adverse outcome in terms of survival, graft versus host disease and post-transplant infectious complications.
Keywords
Introduction
Chronic myeloid leukemia (CML) is a clonal myeloproliferative disease that evolves when a single pluripotential or long-term hematopoietic stem cell acquires the Philadelphia chromosome.1,2 The goals of treatment of CML are complete hematologic and cytogenetic responses. Rapid achievement of a complete hematologic response is associated with a better outcome, whereas complete cytogenetic response is statistically independent marker for improved survival. 3
Tyrosine kinase inhibitors (TKIS) have revolutionized the treatment of CML, offering patients several targeted therapeutic options that provide the possibility of not only sustained remissions but also prolonged survival. 4 Imatinib was introduced into clinical practice in 1998 and by the year 2000 it was clearly established as being highly effective in inducing complete hematological and cytogenetic remissions in the majority of patients with previously treated chronic phase CML. 1 It offers clear quality of life advantages over interferon as first-line treatment for patients with chronic phase CML and after its introduction in the treatment of CML, the role of hematopoietic stem cell transplantation (HSCT) in CML has become more controversial.5,6 Despite that its early adverse effects are mostly mild and transient, safety issues related to its long-term use have to be taken into consideration.7–9
The study described below was initiated by observing that patients with CML treated with imatinib prior to HSCT developed more transplant related complications eg, acute and chronic GVHD, infections and shorter survival compared to patients pre-treated with hydroxyurea or interferon.
Methods and Materials
King Faisal Specialist Hospital and Research Centre (KFSH/RC) in Riyadh is a major tertiary care centre with speciality services including: intensive care units; cardiac, neurosciences and cancer centers in addition to solid organ and hematopoietic stem cell transplant units. A retrospective study of patients with CML who received allogeneic HSCTs between January 2004 and December 2006 was conducted. The medical records of these patients were retrieved for analysis.
Definitions
Complete hematologic response: normalization of blood counts.
Complete cytogenetic response: eradication of Philadelphia chromosome positive bone marrow cells.
Controlled accelerated phase: restoration of chronic disease or achievement of second chronic phase after controlling the transient phase between chronic disease and acute leukemic transformation.
Cytomegalovirus (CMV) infection: detection of CMV excretion in blood by: conventional culture, shell vial, CMV pp65 antigen and CMV-DNA by polymerase chain reaction.
CMV disease: histological or cultural demonstration of CMV in biopsy specimen obtained from body organs eg, liver and lung.
Bacteremia: demonstration of bacteria in the blood stream detected by taking blood cultures from a central venous catheter or a peripheral vein.
Local bacterial infection: demonstration of bacteria in a body organ or tissue, not blood, by taking local specimens eg, sputum, urine, stools etc.
Invasive Aspergillosis: isolation of Aspergillus species from a body tissue biopsy specimen or from a normally sterile body fluid excluding bronchoalveolar lavage.
Engraftment: achievement of the following blood indices for 3 consecutive days: leukocyte count >1 x 10 9 /L with neutrophils >0.5 x 10 9 /L without growth factor administration; hemoglobin level >100 g/L without packed red blood cell transfusion and platelet count >20 x 10 9 /L without platelet transfusion. Engraftment is usually confirmed by performing chimeric studies at regular intervals after HSCT.
Engraftment failure: failure to achieve a leukocyte count >2.0 x 10 9 /L by day 21 following HSCT.
Mucositis: inflammation of mucous membranes of gastrointestinal tract following chemotherapy or radiotherapy. Mucositis is usually classified according to severity into: mild (grade I, able to swallow); moderate (grade II, unable to swallow) and severe (grade III, unable to swallow with local bleeding, edema and sloughing of mucosa).
Veno-occlusive disease of liver: occlusion of small hepatic veins due to injury to vascular endothelium causing cytokine release, post-sinusoidal hypertension and fluid retention leading ultimately to multiple organ failure and hepatic coma.
Hemorrhagic cystitis: inflammation of the mucous membrane of the urinary bladder due to drugs or viral infections causing presence of blood in the urine.
Forty patients with CML were transplanted during the period of time specified above. Twenty one patients received hydroxyurea treatment prior to HSCT, 4 patients received interferon-α preceded by initial therapy with hydroxdyurea and 15 patients were treated with imatinib mesylate after receiving hydroxyurea and/or interferon-α. Eighteen patients (45%) were males and 22 patients (55%) were females. Their ages ranged between 15 and 52 years with a median age of 24 years and a mean age of 25.8 years.
As patients treated with imatinib prior to HSCT were noted to behave differently following HSCT from patients treated with hydroxyurea or interferon, the study patients were divided into 2 groups: (1) group A patients included those patients who received either hydroxyurea (21 patients) or interferon-α (4 patients) prior to HSCT. Among these 25 patients: 12 were males and 13 were females. (2) Group B patients included patients who received imatinib therapy prior to HSCT. This group included 15 patients, 6 of them were males and 9 were females.
The duration of treatment with hydroxyurea, interferon-α or imatinib prior to HSCT was very variable (median: 244 days for group A and 940 days for group B). Prior to HSCT, treatment with hydroxyurea, interferon or imatinib was stopped 2 weeks prior to transplant except in case of increasing leucocytic count where hydroxyurea was given till the start of conditioning therapy. The conditioning regimens used were as follows: oral busulphan and intravenous cyclophosphamide in 35 patients, intravenous (IV) busulphan and cyclophosphamide in 1 patient, IV busulphan and IV fludarabine in 3 patients and fludarabine and total body irradiation (TBI) in 1 patient. Cyclosporine-A and methotrexate were used as graft versus host disease (GVHD) prophylaxis in 36 patients, while cyclosporine-A and mycophenolate mofetil were used in the remaining 4 patients.
Molecular status was checked at 3 monthly intervals before and after HSCT. Chimerism was checked at 2 monthly intervals after HSCT except in relapse or decreasing donor chimerism where testing was done on monthly basis.
Statistical Considerations
Frequency tables were drawn for all variables. Cross-tabulation of the therapy given (hydroxyurea and interferon versus imatinib) was used for the following variables: organs involved by acute and chronic GVHD, overall grades of acute and chronic GVHD, infectious and non-infectious complications of HSCT encountered, survival details in addition to stem cell dose, engraftment and molecular status of the patients studied.
Chi-square test was used to assess the variations between the two types of therapy given, using Chi-square test @ P ≤ 0.05 as a cut-off point for significance level.
Results
Thirty eight [all group A (100%) and 13 group B (86.6%)] patients received HLA-identical sibling allografts, 1 group B (6.7%) patient received an unrelated allograft with one mismatching antigen and 1 umbilical cord blood transplant patient belonging to group B (6.7%) had two mismatching antigens. Bone marrow was the source of stem cells in 32 patients [21 group A (84%) and 11 group B (73.3%)] and peripheral blood allografts were given to 8 patients [4 group A (16%) and 4 group B (26.7%)]. Twenty two patients received allografts from the same sex [male to male: 9 group A (36%) and 3 group B (20%); female to female: 6 group A (24%) and 4 group B patients (26.6%)]. Seventeen patients received allograft from the opposite sex [male to female: 7 group A (28%) and 4 group B (26.6%) patients; female to male: 3 group A patients (12%) and 3 group B (19.9%) patients]. The median age of donors was 22 years for group A and 23 years for group B. Taking into consideration the comorbidity index, there was no significant difference between the two groups of patients.
Regarding the disease status or stage prior to HSCT: 23 (92%) patients belonging to group A were in controlled first chronic phase, 1 patient (4%) was in uncontrolled first chronic phase and 1 patient (4%) was in controlled accelerated phase while 8 (53.3%) patients belonging to group B were in controlled first chronic phase, 6 patients (40%) were in controlled accelerated phase and 1 patient (6.7%) was in second chronic phase. Prior to HSCT, hematological remission was achieved in 24 (96%) patients belonging to group A and in all group B patients, while cytogenetic remission was encountered in 24 (96%) group A patients and in 14 (93.3%) group B patients. Regarding the molecular status of patients prior to HSCT: 21 patients (84%) belonging to group A and 14 patients (93.3%) belonging to group B were positive and there was no statistical difference between the two groups of patients (Table 1).
Stem cell dose and pre-transplant molecular status of patients.
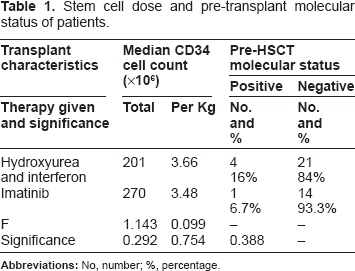
The median total CD34 cell counts were 201 for group A and 270 x 10 6 for group B patients. The median CD34 cell counts per kilogram of body weight were 3.66 for group A and 3.48 x 10 6 for group B. Full engraftment occurred in 21 of group A patients (84%) and 12 of group B patients (80%). Delayed engraftment was encountered in 2 patients belonging to group A (8%) and 2 patients belonging to group B (13.3%) while no engraftment was noted in 2 group A patients (8%) and in 1 group B patients (6.7%). Taking into consideration the stem cell dose, there was no significant statistical differences between the 2 groups of patients (Table 1). At the end of the study: 32 patients (80%) of the entire study patients were alive and 8 patients (20%) were dead. Among these patients, 22 group A patients (88%) were alive while 3 patients (12%) [1 hydroxyurea and 2 interferon] were dead and 10 patients (66.7%) belonging to group B were alive while 5 patients (33.3%) were dead.
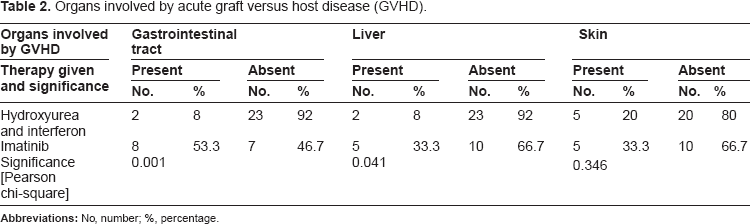
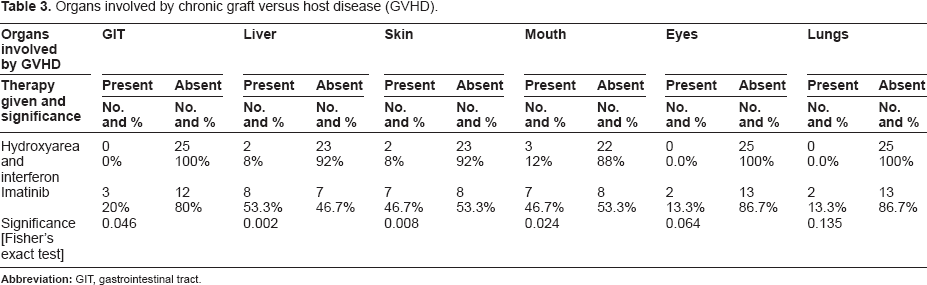
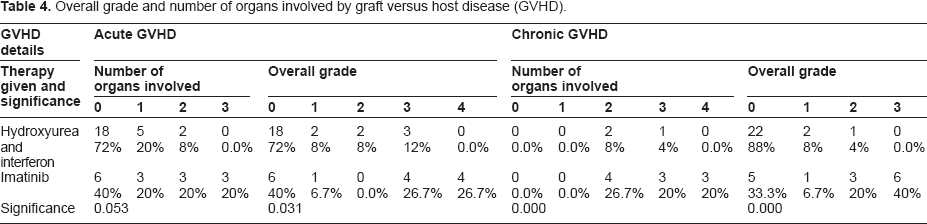
Acute GVHD involved more body organs in group B compared to group A patients (Table 2). Chronic GVHD also involved more body organs in group B compared to group A patients (Table 3). No or single organ involvement by acute GVHD was encountered in 23 group A patient (92%) and in 9 group B patients (60%), while involvement of 2 or 3 organs was seen in 2 group A patients (8%) and in 6 group B patients (40%). Mild involvement by acute GVHD (grades 0 and 1) was encountered in 20 group A patients (80%) and in 7 group B patients (46.7%), while severe involvement (grades III and IV) was encountered in 3 patient belonging to group A (12%) and in 8 group B patients (53.4%) with a P value of 0.031 (Table 4). Involvement by chronic GVHD of 2 or more body organs developed in 3 group A patients (12%) and in 10 group B patients (66.7%) with a highly significant P value of 0.000. Mild involvement by chronic GVHD (grades 0 and 1) was encountered in 24 group A patients (96%) and in 6 group B patients (40%), while severe chronic GVHD (grades 3 and 4) was encountered in 1 group A patient (4%) and in 9 group B patients (60%) with a highly significant P value of 0.000 (Table 4).
Organs involved by acute graft versus host disease (GVHD).
Organs involved by chronic graft versus host disease (GVHD).
Overall grade and number of organs involved by graft versus host disease (GVHD).
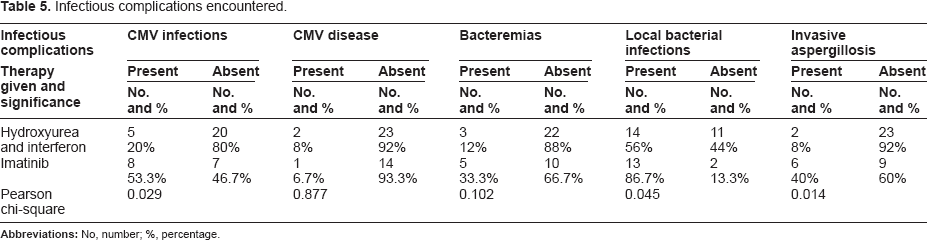
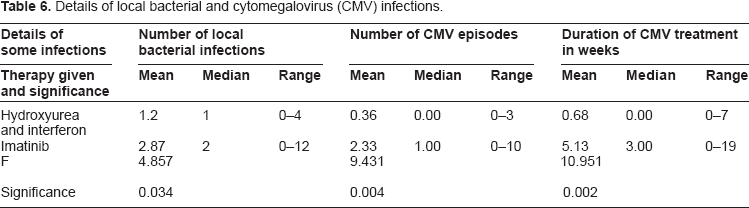
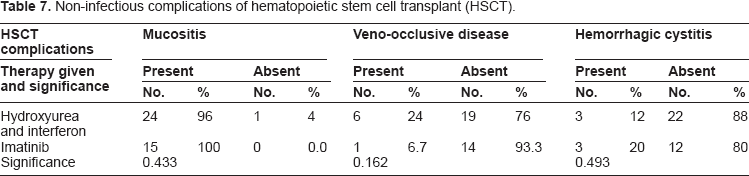
Viral, bacterial and fungal infections occurred in a higher proportion of patients belonging to group B compared to those belonging to group A, with significant P values for CMV, local bacterial and invasive Aspergillus infections (Table 5). The numbers of local bacterial infections and CMV infection episodes were higher in group B compared to group A patients and the duration of CMV infection treatment was longer in group B in comparison to group A patients (Table 6). The non-infectious complications of HSCT eg, oral mucositis, veno-occlusive disease of the liver and hemorrhagic cystitis occurred in almost equal proportions of patients in each group (Table 7).
Infectious complications encountered.
Details of local bacterial and cytomegalovirus (CMV) infections.
Non-infectious complications of hematopoietic stem cell transplant (HSCT).
Taking each treatment modality prior to HSCT separately, full engraftment occurred in a higher proportion in the hydroxyurea group than in the imatinib group of patients [86% vs. 80%] (Fig. 1). The median duration of survival from the date of diagnosis till the end of follow up was higher in the hydroxyurea group compared to the imatinib group of patients (Fig. 2). The median duration of survival from the date of HSCT till the end of follow up was much higher in the hydroxyurea group compared to the imatinib group of patients (Fig. 3).
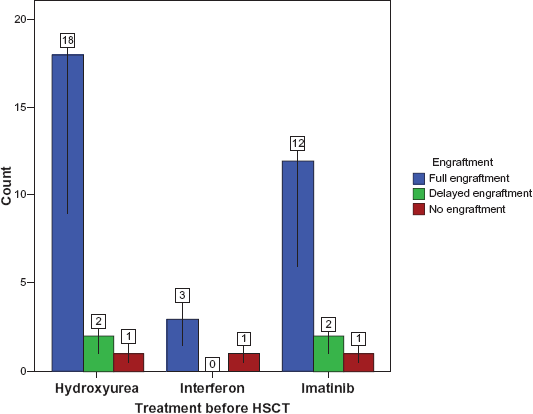
Engraftment details of HSCT recipients.
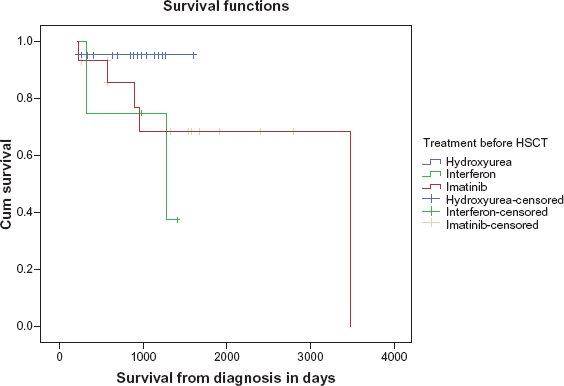
Survival details of HSCT recipients from diagnosis till end of follow up in days.
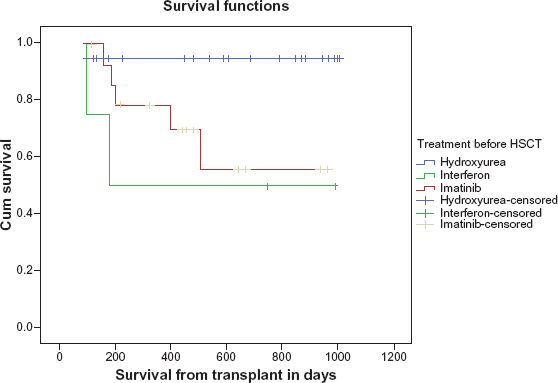
Survival details of HSCT recipients from transplant till end of follow up in days.
Following HSCT: molecular relapses were encountered in: 5 group A (20.8%) patients, 4 at 9 months and 1 at 12 months post-HSCT while 4 group B patients (26.7%) had molecular relapses, 1 at 9 months and 3 at 12 months post-HSCT. In patients having mixed chimerism or increasing recipient type of chimerism, donor lymphocyte infusions (DLIs) were given and imatinib at doses of 400 mg/day was used in the treatment of relapses encountered in the post-transplant setting.
Discussion
Allogeneic HSCT has been used in the management of CML since the 1970s. 2 Until the year 2000, allogeneic HSCT was the recommended treatment for all new patients with CML who were eligible on grounds of age and donor availability. 1 With long-term follow up, there is strong evidence that cure of CML can only be achieved by allogeneic HSCT, but treatment related mortality and morbidity have led to a significant decline in the number of transplants performed over the last 5 to 6 years and most patients prefer to stay on imatinib as a more tolerable and effective therapy. 6 , 10 Nowadays, HSCT is still reserved for patients whose TKI therapy has failed or who have advanced disease ie, accelerated phase or blastic transformation of CML. 7 Some studies have shown that pre-treatment with imatinib is not an independent negative prognostic factor and that patients with advanced forms of CML have dismal prognosis as they are at high risk for transplant-related mortality. 6 Other studies have shown that CML has an excellent outcome after allogeneic HSCT when transplanted in a state of low tumor burden ie, in the phase of cytogenetic response to imatinib. 11 The following factors have been identified to significantly influence long-term survival of CML patients subjected to allogeneic HSCT: age, disease duration, disease status at transplant, source of transplant product, recipient donor gender combinations and degree of histocompatibility between donor and recipient.2,11 Evidence in the pre-imatinib era suggests that allogeneic HSCT is best performed in the early phase of chronic CML. Using blood or bone marrow derived stem cells from an HLA-identical sibling donor performed in the chronic phase of CML, allogeneic HSCT offers 60% to 80% probability of leukemia-free survival at 5 years. If transplant is performed in the accelerated phase of CML, survival decreases by 50%. Conventionally, conditioning therapies involve myeloablative doses of chemotherapy and radiotherapy aiming to facilitate engraftment of healthy donor stem cells via permanent elimination of malignant hematopoiesis. 2
Allogeneic HSCT is the only known curative therapy for patients with CML, but it is associated with significant morbidity and mortality. 12 However, after the introduction of targeted therapy to the BCR/ABL transcript with TKIs in May 2001, the timing of its application has altered significantlty to the extent that it is now considered as second or even third line therapy. 13 In patients with CML who receive allogeneic HSCTs, the probabilities of overall survival at 5 years are: 87%, 52% and 45% in patients who receive grafts from siblings, matched unrelated donors and mismatched donors respectively. Transplant-related mortality and GVHD, but not the type of conditioning therapy, have contributed to the inferior outcome in unrelated donor and mismatched allografts. 14 CML patients who received myeloablative allogeneic grafts in first CP and who remained in remission for at least 5 years had favourable subsequent survival. In such patients, history of chronic GVHD increased risks of late overall transplant-related mortality but decreased risks of relapse of primary disease. 15 In patients with CML who relapse at molecular level or develop minimal residual disease after allogeneic HSCT, imatinib therapy has been shown to be safe, well tolerated and highly efficacious in restoring complete molecular remissions although its use has been associated with myelosuppression and recurrence of severe GVHD.16,17 The use of DLI has been associated with a risk of inducing or re-inducing GVHD, but such risk can be minimized if an escalating dose schedule for DLI is followed. A reasonable compromise may be to restore remission with imatinib and then to introduce DLIs starting at a low dose. 1
The impact of imatinib pre-treatment on the outcome of allogeneic HSCT in CML patients is still controversial and unclear.8,11 A number of studies have shown that pre-HSCT imatinib therapy is not associated with increased transplant-related mortality or poorer outcome. Other studies have shown not only a higher incidence of non-relapse transplant related mortality, but also a higher degree of hepatotoxicity.1,11,18–25 Whether imatinib pre-treatment associated toxicity adds to the toxicity of allogeneic HSCT is still under investigations and has so far revealed conflicting results.1,11
Azole antifungal agents eg, itraconazole and fluconazole, alter the metabolism of cyclophosphamide in unique fashions, through differential inhibition of hepatic cytochrome P-450 isoenzymes, thus causing impacts on toxicities in the early post-HSCT period. 26 Concomitant administration of oral voriconazole increases the bioavailability of neoral, the micoemulsion form of cyclosprine-A, probably due to the inhibition of gut CYP3A4 by voriconazole. Low trough levels of cyclosprine-A and tacrolimus have been found to correlate with the development of acute GVHD. Therefore, monitoring cyclosporine and tacrolimus exposure early after HSCT and adjusting their doses to a prdefined target trough levels and areas under the blood concentration versus time curve may provide a tool to influence GVHD/GVL (graft versus leukemia) balance and clinical outcome.27–29 Imatinib can also interfere with the metabolism of cytotoxic drugs like cyclophosphamide by competing for metabolization by cytochrome P450-3A4. One potential result of such drug interactions could be a higher incidence of extra-medullary toxicities after myeloablative conditioning therapy. It is important for clinicians to know the elimination kinetics of imatinib and its main metabolite [N-desmethylimatinib]. If possible interactions of imatinib need to be avoided, this drug should be stopped at least one week before starting conditioning regimen for HSCT if the underlying disease so allows. 30
Improvements in infection prophylaxis, immunosuppressive therapies, supportive care and DNA-based tissue typing have contributed to improved outcome of allogeneic HSCT. GVHD is a major and a potentially lethal complication of allogeneic HSCT and it limits the use of this potentially curative therapeutic procedure. The severity of acute GVHD is determined by the extent of involvement of the three principal target organs (skin, gastrointestinal tract and liver). The overall grades of acute GVHD are classified as follows: mild (grade I), moderate (grade II), severe (grade III) and very severe (grade IV). Grades III and IV acute GVHD carry poor prognosis with long term survivals of 25% and 5% respectively. The incidence of acute GVHD is directly proportional to the degree of mismatching between HLA proteins and ranges from 35%–45% in recipients of identical sibling donor grafts to 60%–80% in recipients of one-antigen HLA mismatched unrelated donor allografts. 31 Factors significantly associated with development of grades II to IV acute GVHD are: TBI and cyclophosphamide conditioning, primary disease being CML, peripheral blood allografts in patients younger than 39 years, bone marrow grafts in patients 40 years or older, low performance score and CMV seronegativity in both recipient and donor. CML patients subjected to allogeneic HSCT have been found to have higher cytokine levels and hence more advanced forms of acute GVHD than patients with acute leukemia. The cytokine storm, mainly elevated serum levels of interferon-alpha (IFN-α) and interleukin-6 (IL-6), in recipients of HSCT may precipitate not only acute and chronic GVHD but also other major complications of HSCT.32–34
Chronic GVHD is an important late complication of allogeneic HSCT and is a major determinant of long term outcome and quality of life following allografting. Old age of recipient, use of peripheral blood cell grafts, use of unrelated or HLA-mismatched donors and use of DLI have been identified as independent risk factors affecting survival without recurrent malignancy. Extensive skin involvement eg, lichenoid skin lesions, elevated serum bilirubin level, thrombocytopenia, history of prior steroid refractory/dependent acute GVHD and progressive onset of chronic GVHD are poor prognostic variables in chronic GVHD. The influence of chronic GVHD on survival reflects a delicate balance between its negative (increased transplant-related mortality) and positive (fewer disease relapses) effects.35,36
Patients with blastic phase of CML are often refractory to induction chemotherapy and hence their median survival is relatively short. 3 In patients with Philadelphia chromosome-positive acute lymphoblastic leukemia (Ph+ALL), disease-free survival is very poor and allogeneic HSCT is currently considered the only therapeutic intervention with curative potential. The following pre-transplant factors are significantly associated with better survival: young age of recipient, early transplantation, complete remission at the time of transplant, conditioning with TBI and HLA-identical sibling donor. Disease relapse is the major obstacle limiting the success of HSCT in this category of patients. Severe (grades III and IV) acute GVHD is associated with poor outcome, while chronic extensive GVHD is associated with improved survival.37,38 The outcome of allogeneic HSCT in CML patients is determined by the following: (1) recipient-related factors: age, comorbidity index, race, performance status, prior chemotherapeutic regimens, IL-10 pro-motor polymorphism, and disease status (stage, cytogenetic abnormalities and time from diagnosis). (2) donor-related factors: age, gender, KIR genotype and level of HLA mismatching. (3) conditioning therapy: TBI/cyclophosphamide versus busulphan/cyclophosphamide. (4) graft-related factors: CD4/CD8 ratio in bone marrow grafts.(5) transplant-related complications: acute and chronic GVHD. The best outcome is encountered in patients: younger than 30 years having no comorbidities, normal C-reactive protein and early stage of disease (first chronic phase, transplanted within 6–12 months from diagnosis) who receive allografts with low CD4/CD8 ratio and busulphan/cyclophosphamide conditioning therapy and do not develop grades III/IV acute GVHD.12,14,39–42
Our study showed that both acute and chronic GVHD were not only more frequent, but also more severe and extensive in the imatinib group compared to the hydroxyurea and interferon group. Consequently, patients who had been treated with imatinib in the pre-transplant period required heavier and more prolonged immunosuppressive therapies and this led to higher proportions of infectious complications and all such post-HSCT consequencies were ultimately translated into higher mortality and shorter post-transplant survival.
We believe that a single or multiple interactions between any of the following medications: imatinib, azole antifungals eg, fluconazole and voriconazole used in fungal infection prophylactic and therapeutic HSCT regimens, immunosuppressive agents eg, cyclosprine used in GVHD prophylaxis and cytotoxic medications eg, cyclophosphamide used in the preparative conditioning therapies of HSCT could account for the extramedullary toxicities of imatinib and its metabolits encountered in the post-transplant period and that the underlying disease, CML, as well as imatinib therapy might be responsible for the induction of a series of immunological changes that paved the way for the evolution of severe acute and chronic extensive GVHD. As a consequence of difficulties in controlling advanced grades of GVHD, potent and prolonged immunosuppressive therapies were needed. Moreover, profound suppression of immunity in such patients, whose immune systems had already been adversely affected by the primary malignancies and by the medications used to control them, could be responsible for the development of serious infectious complications that led to higher mortality rates and shorter survival in CML patients subjected to HSCT. We acknowledge the following facts: retrospective studies have their own limitations, the number of patients included in our study was rather small and patients treated with imatinib were probably a sicker cohort taking into account the longer disease duration prior to HSCT and the use of other agents before the initiation of imatinib therapy.
Conclusion
Once subjected to HSCT, CML patients treated with imatinib mesylate are likely to suffer serious consequences paticularly GVHD, infections and short survival. These findings may be explained by multiple drug interactions and immunological changes induced by imatinib therapy, allogeneic HSCT or the primary disease (CML). Further multicentre clinical, pharmacological and immunological studies are needed not only to validate our findings, but also to make satisfactory explanations for the results of our study.
Disclosure
This manuscript has been read and approved by all authors. This paper is unique and is not under consideration by any other publication and has not been published elsewhere. The authors and peer reviewers of this paper report no conflicts of interest. The authors confirm that they have permission to reproduce any copyrighted material.
Footnotes
Acknowledgements
We are grateful to all medical, nursing and technical staff at KFSH&RC in Riyadh, Saudi Arabia, who participated in the management of the patients studied.