
Abstract
Oropharyngeal candidiasis is a common affliction in HIV-positive patients worldwide. Although the incidence has decreased with the advent of potent antiviral combinations, it continues to be a cause of significant morbidity. Historically, fluconazole or itraconazole was the treatment of choice for oropharyngeal candidiasis, but increasing incidence of resistance and high recurrence rates mandate the use of alternative therapies. Posaconazole, a broad-spectrum second-generation triazole antifungal agent, has been studied in both first-line and salvage settings for treatment of oropharyngeal candidiasis. Posaconazole is well-tolerated, yields high response rates and demonstrates durable response rates with long-term use. This review will provide state-of-the-art knowledge of pharmacology and therapeutics of posaconazole focusing on the indication for oropharyngeal candidiasis in HIV-positive patients.
Keywords
Introduction
Oropharyngeal candidiasis (OPC) occurs in a majority of human immunodeficiency virus (HIV)-positive patients and is considered an acquired immunodeficiency syndrome (AIDS)-defining illness. 1 Historically, OPC was one of the first signs of illness, but the incidence has declined with advances in highly active antiretroviral therapy (HAART) in developed countries. It persists in developing countries as an initial presentation.1–3 Patients with AIDS may be burdened by recurrent OPC, including triazole-resistant disease, leading to high morbidity associated with each occurrence. 4 The effects of OPC include localized pain, xerostomia and mucocutaneous breakdown, and these effects can cause dysgeusia and malnutrition contributing to muscle wasting in AIDS patients.5,6
By definition, OPC is caused by overgrowth of naturally-occurring Candida spp., with C. albicans identified in 90% of cases, in the setting of total body or mucocutaneous-localized immune compromise. Beyond individuals with AIDS, OPC is known to occur in patients receiving myelosuppressive chemotherapy and/or immunomodulator therapy, solid-organ transplant recipients, patients with congenital cell-mediated immune dysfunction, patients on chronic systemic glucocorticoids at doses greater than physiologic, and patients using inhaled glucocorticoids.4,7–9 In HIV-positive individuals, OPC occurs when the CD4 count falls below 200 cells/µL and the overall incidence and severity of OPC increases as a function of declining CD4 counts. 7 This manuscript will focus on OPC in HIV-positive patients.
Triazole Resistance in Candida spp
Resistance in Candida spp. to triazole antifungal agents has been steadily increasing in virtually all clinical settings, including HIV-positive patients, due to selective pressure and widespread use of triazole antifungal agents, both as prophylaxis and treatment.4,10 However, triazole-resistant OPC is a greater concern in HIV-positive patients due to high rates of recurrence and persistently declining immune competence over time. 9 De novo resistance to fluconazole by C. albicans is <5%, but breakthroughs with resistant Candida spp. during treatment have been reported. 10 Prior fluconazole use is a risk factor in the appearance of non-albicans Candida infections, including C. krusei and C. glabrata. Despite small numbers in this series, a trend towards fluconazole resistance was demonstrated in patients with fluconazole pre-exposure. 11 Furthermore, serial isolates of OPC in HIV-positive patients reveals heteroresistant Candida may co-exist, each with different triazole sensitivity patterns. 12 Prior triazole exposure is an important determinant for the occurrence of triazole-resistance, mandating careful selection of initial triazole antifungal.
Cross-Resistance
Clinical evidence of triazole antifungal cross-resistance between fluconazole, itraconazole and ketoconazole was first seen in AIDS patients with refractory OPC. 10 Several mechanisms are known to confer triazole cross-resistance, including multi-drug efflux pumps, mutations of target enzyme, overexpression of the target enzyme and DNA mutations. 10 Although C. albicans and C. glabrata are known to use any or all of these resistance mechanisms towards fluconazole, only overexpression of efflux pumps lead to posaconazole resistance. 10 A series of C. albicans isolated from an AIDS patient with refractory OPC demonstrated fluconazole and voriconazole resistance, but initial susceptibility to itraconazole and posaconazole that waned with continued treatment. 13 An in vitro study of C. albicans isolates demonstrated that resistance to fluconazole and/or voriconazole did not confer cross-resistance to posaconazole. 14 This is controversial, as recent data have demonstrated cross-resistance, especially in non-albicans Candida. 15 Posaconazole is Food and Drug Administration (FDA)-approved and European Medicines Agency (EMA)-approved for the treatment of OPC, including first-line treatment and treatment of OPC that is refractory to itraconazole and/or fluconazole. 16
Pharmacotherapy of OPC
Due to cost, side effect profile and minimal drug-drug interactions, fluconazole is currently the recommended drug of choice for primary treatment of OPC.4,17 However, fluconazole as first line is based upon clinical trials conducted in an era prior to second generation triazole antifungal agents and before greater virological control with newer HAART agents. 17 In these trials, fluconazole was favored over ketoconazole, itraconazole, clotrimazole and nystatin for treatment of OPC due to clinical and/or mycological cure, drug tolerability and/or adverse effects. 17 A recent study comparing fluconazole to posaconazole in 366 treatment-naïve subjects showed similar clinical cure, but higher mycological cure for posaconazole, although mycological eradication was not statistically different. 18
While superiority could not be demonstrated in clinical trials, posaconazole may have an advantage over fluconazole, both in the treatment-naïve and refractory OPC setting. When compared to fluconazole, Posaconazole has a broader spectrum of activity, including fluconazole-resistant Candida spp., diminished incidence of recurrent OPC and greater insensitivity to fungal resistance mechanisms.17,18
Posaconazole Pharmacology
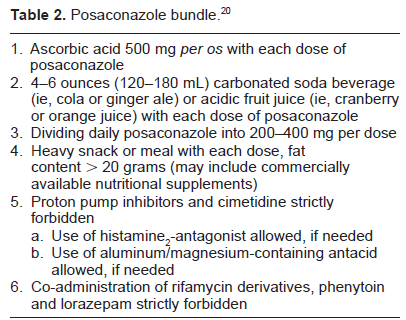
Posaconazole is a second-generation triazole anti-fungal with broad spectrum of action, including yeasts, moulds and Mucormycoses spp. 19 Currently available only in an oral formulation, absorption is a great barrier to clinical use. Several interventions have proven useful to optimize the absorption of posaconazole, particularly when used in combination in a care bundle. This bundle approach may include practicing co-administration with high-fat meals, strict avoidance of proton-pump inhibitors, rifamycin derivatives, and phenytoin, dividing the dosage to a maximum of 200 mg per administration, and co-administration with acidic beverage and ascorbic acid at 500 mg per os. 20
Therapeutic drug monitoring (TDM) of posaconazole is controversial due to poorly elucidated toxic serum levels and lack of correlation with serum levels and outcomes. 21 While recent data in malignant hematology/oncology patients extol TDM for posaconazole when employed for invasive fungal infection treatment and prophylaxis, treatment of OPC may not mandate TDM given that OPC is a superficial fungal infection. 21 However, in select patients where the clinician has reason to suspect poor absorption, TDM may serve to verify medication adherence or absorption.
Clinical Trials
The Infectious Diseases Society of America (IDSA) recommends posaconazole only for fluconazole-refractory OPC. IDSA guidelines recommend posaconazole at a dosage of 400 mg twice daily for 3 days, then 400 mg daily for up to 28 days. 22 Interestingly, the manufacturer's dosing recommendations for posaconazole in fluconazole-refractory OPC are different than those recommended by the IDSA guidelines. The package insert recommends posaconazole 400 mg twice daily for fluconazole-refractory OPC, with the duration of therapy based upon the severity of the patient's underlying disease and clinical response. 16
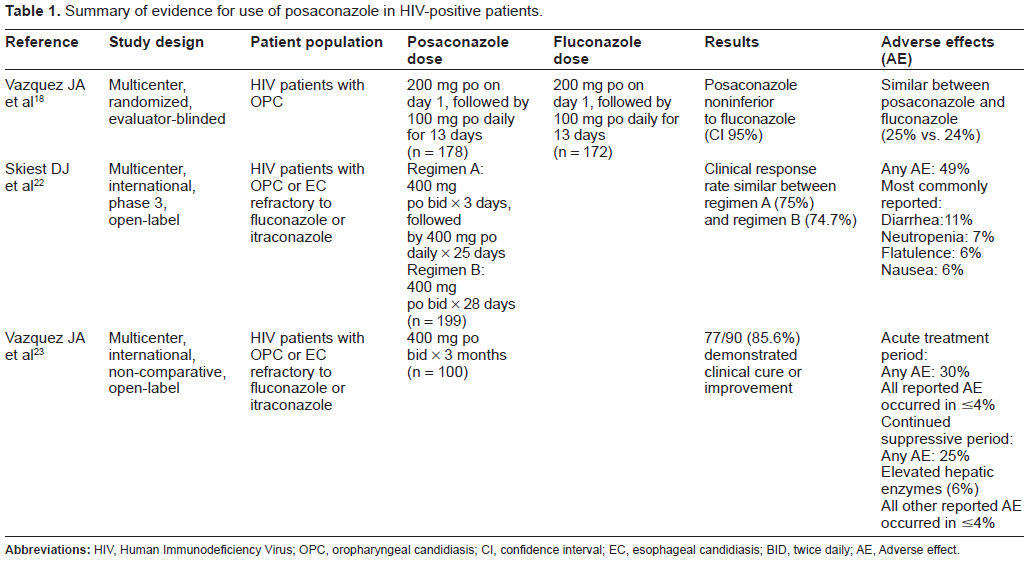
Table 1 summarizes the registration trials for posaconazole in HIV-positive OPC. The first study comparing posaconazole to fluconazole conducted a multi-center, randomized, evaluator-blinded study of HIV-positive patients with antifungal treatment-naïve OPC. 18 The primary objective of the trial was to compare the clinical efficacy of posaconazole to the active comparator (fluconazole) by evaluating clinical cure or clinical improvement rates following 14 days of therapy. Clinical cure was defined as the absence of plaques or ulcers and no or minimal symptoms while clinical improvement was defined as a decrease in sores used to measure lesions and symptoms. Those with cure or improvement at day 14 were subsequently evaluated on day 42 for durability of clinical cure/improvement or clinical relapse as a secondary endpoint. Other secondary endpoints included clinical response rates by visit, evaluated by quantitative mycologic cultures on days 7 and 14 of posaconazole dosing. A total of 350 study subjects were randomly assigned to receive 200 mg of either posaconazole or fluconazole oral suspension on day 1, followed by a 100 mg daily dosage of the same drug for 13 days. On day 7, clinical success was similar between the two groups, with similar success rates at 164/169 (97.0%) of posaconazole patients and 155/160 (96.9%) of fluconazole patients. Clinical success was also similar on day 14 between the two groups, with success rates at 155/169 (91.7%) of posaconazole patients and 148/160 (92.5%) of fluconazole patients. Overall, this trial indicates the non-inferiority of posaconazole to fluconazole. Mycological success on day 14 was similar between both groups, with a success rate of 68%. However, differences in mycologic success were seen at day 42. More patients who received posaconazole demonstrated continued mycologic success, 41/101 (40.6%) vs. 24/91 (26.4%) (P = 0.038). Treatment related adverse events were similar between both treatment arms.
Summary of evidence for use of posaconazole in HIV-positive patients.
Upon subanalysis, triazole-susceptible Candida spp. displayed similar treatment outcomes. In 144 posaconazole and 138 fluconazole patients with C. albicans, clinical response was similar (98% vs. 97%). Although the numbers are small, patients infected with C. glabrata demonstrated clinical response rates of 100% in both groups (5 posaconazole vs. 4 fluconazole patients). When the susceptibility of C. albicans was dose-dependent (fluconazole MIC 8-32 µg/mL), the clinical response rate was 100% with posaconazole (4 patients) and 80% with fluconazole (4 out of 5 patients). When the pathogen was discovered to be C. glabrata (fluconazole MIC 8-32 µg/mL), the clinical response was 86% with posaconazole (7 patients) and 100% for fluconazole (2 patients). When the susceptibility of the infecting Candida spp. was resistant, MIC > 32 µg/mL, the clinical response rates for posaconazole and fluconazole were both 100% for both C. albicans and C. glabrata. The small numbers in the susceptible dose-dependent and non-susceptible categories render difficult the extrapolation of these seemingly perplexing results. 18
A subsequent study evaluated the efficacy and safety of oral posaconazole in a multicenter, international, phase 3, open-label study for HIV-infected patients with OPC or esophageal candidiasis (EC) and who failed oral fluconazole or itraconazole. 22 The primary end point of the trial was rate of cure or improvement after 28 days of posaconazole therapy. Secondary endpoints included clinical response–-either cure or improvement–-on day 14 and clinical response stratified by presence or absence of in vitro resistance to fluconazole or itraconazole among Candida spp. cultured at study entry. A total of 199 patients were enrolled in the trial. Of these, 149 patients had OPC, 18 had EC and 32 had both OPC and EC. In the original protocol (“regimen A”, n = 103), patients received posaconazole suspension 400 mg twice daily for 3 days, followed by posaconazole 400 mg once daily for 25 additional days. Following 28 days of therapy, patients with clinical response and absence of symptoms could continue to receive posaconazole 400 mg twice daily, 3 times per week for an additional 3 months. This protocol was amended for patient simplicity (“regimen B”, n = 96), where new patients received oral posaconazole 400 mg twice daily for 28 days continuously. Patients successfully completing regimen B could be enrolled into a long-term maintenance study for up to 15 months. Overall, 132 of 176 subjects (75%) experienced cure or improvement after 28 days of therapy. Clinical response rates were not different between regimen A (75.3%) and regimen B (74.7%). Subjects were evaluated mid-way through initial therapy (ie, after 14 days), demonstrating that 93 of 176 (52.8%) patients were clinical responders and only 4 of 176 (2.3%) were non-responders. Clinical response rates among patients with azole-resistant Candida spp. at baseline were 67 of 92 (73%) with fluconazole resistance, 49 of 66 (74%) with itraconazole resistance, and 42 of 57 (74%) with resistance to both agents. Adverse events related to treatment were reported in 98 of 199 (49%) of patients. The most common adverse reactions reported were diarrhea (11%), neutropenia (7%), flatulence (6%), and nausea (6%).
A third trial evaluated the safety and efficacy of posaconazole in a multicenter, international, non-comparative, open-label study in HIV-infected patients with OPC, EC or both and whose disease was clinically refractory to oral fluconazole or itraconazole. 23 The primary endpoint of the study was the rate of cure or improvement at the end of the 3 month treatment period. Secondary endpoints included clinical response by baseline susceptibility at the end of the 3 month treatment period, clinical response rates at 1, 2, and 3 months, and relapse rates during the 1 month, treatment-free, follow-up period. All patients received posaconazole 400 mg twice daily for 3 months. After 3 months, clinical responders were eligible to continue therapy with the same dose of posaconazole for up to 12 months at the discretion of the investigator. Clinical responders who did not continue posaconazole were observed for up to 1 month. Patients enrolled into the study included two different populations, the first group being posaconazole-naïve and the second group consisting of subjects who had received prior therapy with posaconazole for 1 month in the acute care study and demonstrated partial or complete resolution of OPC, EC, or a complete response or improvement with relapse upon discontinuation of study drug. Of the 100 patients enrolled, 60 of these subjects were originally treated in the 1 month acute care study and were enrolled into the long-term study. The other 40 patients were posaconazole naïve. For the modified intent-to-treat (MITT) population, 59 were previously treated with posaconazole and 31 were posaconazole-naïve. Overall, after the 3 month treatment period, 77/90 (85.6%) demonstrated clinical cure or improvement. Response rates were similar in the posaconazole-naïve patients, 25/31 (80.6%), as with patients having prior posaconazole exposure, 52/59 (88.1%). Response rates according to Candida spp. and susceptibility in posaconazole-naïve patients with any Candida spp. isolate resistant to fluconazole (MIC > 32 µg/mL), itraconazole (MIC > 0.5 µg/mL), or both were 17/20 (85%), 15/18 (83%), and 14/17 (82%) respectively. Patients previously treated with posaconazole had the respective response rates of 21/22 (95%), 15/18 (83%), and 14/15 (93%). The clinical response rates were 83/85 (97.7%) after 1 month of therapy, 64/70 (91.4%) after 2 months and 42/44 (95.5%) after 3 months. Patients who missed a monthly visit were not included in the response assessment for that month. The majority of patients were not assessed for clinical relapse at the end of 3 months due to treatment being discontinued or because the subject went immediately into the long-term suppressive phase. Upon evaluation, 13/28 (46.4%) suffered clinical relapse and 15/28 (53.6%) continued to maintain clinical response. The most common adverse event in the acute was vomiting, while elevated hepatic enzymes was most common in continued suppressive treatment cohort.
Safety
In general, clinical trials demonstrated that posaconazole is well tolerated. In a pooled safety analysis of 18 controlled trials including 448 healthy patients who received at least one dose of posaconazole, incidence of adverse effects were similar to placebo (57% vs. 63%). 24 The most common adverse events among those receiving posaconazole were headache (17%), dry mouth (9%) and dizziness (6%). Five patients (<1%) discontinued posaconazole due to adverse effects. Liver enzyme increases of > 1-2.5 times the upper limit of normal occurred in 5%-11% of subjects receiving posaconazole. Elevations in liver function tests did not appear to be dependent on posaconazole exposure. Changes were transient and returned to baseline once dosing stopped. The analysis did not find any associated cardiovascular adverse events and ECG analysis suggested minimal potential to prolong QTc interval with a mean and median interval change from baseline of -5 msec.
Furthermore, patients on long term posaconazole appear to be at no greater risk for adverse effects than those that receive short term therapy. In a study of 428 patients with refractory invasive fungal infections or febrile neutropenia, 109 patients received posaconazole for ≥6 months. Patients receiving posaconazole for ≥6 months had a comparable safety profile to those who received posaconazole for >6 months. 25 Overall reports of adverse events occurred in 35% receiving <6 months therapy versus 47% receiving >6 months. This study included overall treatment-related side effects of increased serum glutamic pyruvic tranaminase levels (3%), QTc interval prolongation (1%) and convulsions (<0.5%). There were no unique adverse effects observed with long term posaconazole exposure.
HIV-Positive Subjects with OPC
A randomized study comparing posaconazole (N = 178) and fluconazole (N = 172) in treatment-naïve OPC noted similar incidence of adverse events related to treatment. There were 25% of posaconazole-treated patients and 24% in the fluconazole-treated cohort reporting adverse events, with gastrointestinal adverse events encountered most commonly. 18 Another 239 HIV-positive patients with triazole-refractory OPC received posaconazole in 2 non-comparative trials for refractory OPC.22,23 Of the subjects included, the most common adverse reactions were fever, diarrhea, nausea, headache, and vomiting, all of which occurred in 6% or less of patients. In patients who received 3 months of posaconazole therapy, 30% of participants reported adverse effects related to treatment. 23 The most frequent effect reported was vomiting (4%), while elevated hepatic enzymes occurred in 6% of those who received continued 12-month suppressive therapy (Table 1). One patient suffered from cardiac failure with a possible relationship to posaconazole in the 3-month treatment group and another patient developed jaundice in the 12-month group. There were no observations of neurologic or visual complications associated with posaconazole. When compared to fluconazole, posaconazole demonstrates comparable tolerability in the HIV-positive population for OPC, an important consideration in patients often taking multiple hepatically-metabolized medications concomitantly.18,22,23
Hepatic Toxicity
Mild and transient increases in hepatic enzymes have been observed with posaconazole administration. These occurrences are infrequent, occur more commonly in those >65 year of age and return to baseline upon cessation of posaconazole irrespective of treatment duration. 24 Cases of severe hepatic reactions including cholestasis or hepatic failure have been reported in patients with other serious underlying disease states while concomitantly receiving posaconazole. These severe hepatic reactions were seen in subjects receiving higher posaconazole doses for indications other than OPC. 26 Appropriate patient management should include periodic laboratory evaluation of hepatic function and monitoring for clinical signs and symptoms of liver dysfunction.
Posaconazole Resistance
Primary and secondary posaconazole resistance is rare. Posaconazole structurally has an extended side chain similar to itraconazole while a more compact structure is found in fluconazole and voriconazole. This extended side chain allows for additional points of contact with the azole target, 14-alpha-demethylase (CYP51), thereby blocking ergosterol synthesis. In fact, the side chain for posaconazole is characterized by extensive hydrophobic contacts strengthening the binding affinity. 27 This in turn creates a situation in which single mutations to C. albicans near the CYP51 binding site that profoundly impact resistance to fluconazole will have only a minor impact on posaconazole susceptibility. In a study of the molecular mechanisms responsible for reduced susceptibility to azoles in C. albicans, it was demonstrated that multiple ERG11 (encodes for the CYP51 binding site) mutations are required to significantly reduce posaconazole susceptibility. 7
Furthermore, the most common mechanism contributing to triazole resistance in C. albicans is a reduction in intracellular drug exposure due to increased expression of efflux pumps. 13 While posaconazole is a substrate of efflux pumps encoded by CDR1 and CDR2 in C. albicans, it is not a substrate of the major efflux pumps encoded by MDR1 and FLU1 that efflux fluconazole. 27 Therefore, posaconazole resistance is less likely to develop as a result of efflux pump related resistance when compared to fluconazole.
Drug-Drug Interactions
CYP450 interactions
Inherently, due to the inhibition of fungal cytochrome P450 by which the triazole antifungals exert their activity, the entire drug class is prone to drug-drug interactions. A study evaluating potential drug interactions of posaconazole via the CYP450 enzymatic pathway observed no impact on CYP1A2, CYP2C8/9, CYP2D6 and CYP2E1. 28 The study did however observe a decrease in hepatic CYP3A4 activity associated with posaconazole. In contrast, ketoconazole inhibits CYP1A2, 2C9, 2C19 and 3A4; itraconazole inhibits CYP1A2, 2C9 and 3A4; fluconazole inhibits CYP1A2, 2C9, 2C19 and 3A4; and voriconazole is a known inhibitor of 2C9, 2C19 and 3A4. Thus, overall there is less concern for CYP450 related drug interactions with posaconazole versus other triazole antifungals.
Due to the CYP3A4 inhibition exerted by posaconazole, caution must be observed when administered in the HIV-positive population. Most protease inhibitors and non-nucleoside reverse transcriptase inhibitors are CYP3A4 substrates. A recent study investigated the interaction between posaconazole and the antiretrovirals atazanavir, ritonavir and efavirenz. 29 Co-administration of posaconazole and atazanavir, a substrate and inhibitor of 3A4, resulted in a 2.6-fold and 3.7-fold increase in maximum serum concentration (Cmax) and area-under-the-curve (AUC) for atazanavir, respectively. Administration of posaconazole, atazanavir and ritonavir resulted in a Cmax increase of 1.5-fold and AUC increase of 2.5-fold when compared to atazanavir and ritonavir combination alone. Posaconazole concentrations did not significantly change when co-administered with either combination. When posaconazole was co-administered with efavirenz, the efavirenz exposure did not significantly change.
Other medications with CYP3A4 interactions that are contraindicated for use with posaconazole include sirolimus (9-fold increase in sirolimus blood concentrations), pimozide and quinidine (potential QTc prolongation), 3-hydroxy-3-methylglutaryl-CoA reductase inhibitors (10-fold increase in simvastatin blood concentrations), and ergot alkaloids (potential ergotism). 16
Concomitant administration of posaconazole with narrow therapeutic index medications, such as vinca alkaloids, calcineurin inhibitors and sirolimus, should be avoided or carefully monitored due to potential for increased toxicity by these agents in the presence of posaconazole. 16 The clinician should bear in mind that the degree and duration of drug-drug interaction with all triazole antifungals differ and a significant drug-drug interaction should be assumed unless other data are available. It is also important to note that greater clinical experience exists with fluconazole and itraconazole drug-drug interactions than posaconazole drug-drug interactions. Wherever possible, use of therapeutic drug monitoring should be strongly considered when using interacting medications and/or avoiding concomitant administration.
Unlike other triazoles, posaconazole is not a significant substrate for CYP450 metabolism. Co-administration of inhibitors or inducers of CYP450 enzymes have not shown a significant effect on the pharmacokinetic profile of posaconazole.
UGT 1A4 interactions
In contrast to other triazole antifungals, posaconazole is hepatically metabolized into inactive glucuronides by phase II UDP-glucuronosyltransferase (UGT). Inducers of UGT will result in a reduction in posaconazole exposure with the potential for posaconazole clinical failure. Efavirenz, a UGT inducer, was found to decrease the Cmax and AUC of posaconazole by 45% and 50%, respectively. 29 Co-administration of fosamprenavir, a less potent UGT inducer, resulted in 23% reduction in posaconazole exposure. 30 Furthermore, administration of posaconazole with UGT inducers phenytoin and rifabutin have also yielded reduced posaconazole exposure.31,32
Co-administration of posaconazole with UGT inducers like efavirenz, fosamprenavir, phenytoin and rifabutin should be avoided in order to reduce the risk of posaconazole failure. Other inducers of UGT continue to be identified such as lorazepam which significantly reduced posaconazole exposure. 33 UGT interactions, many of which are not well-characterized, underscore the need for TDM to ensure appropriate drug exposure. Additionally, when posaconazole is used in combination with HAART regimens, frequent monitoring for adverse effects and toxicity related to elevated antiviral concentrations is recommended due to the CYP3A4 and/or UGT interaction.
Patient Preference
As noted previously, rates of adverse effects are similar between posaconazole and fluconazole (25% vs. 24%) with similar rates of discontinuation. 18 Additionally, the current recommended dosing length and schedule of posaconazole for OPC is comparable to that of fluconazole. The primary issues to consider include administration of posaconazole with relation to meals (preferably, high-fat containing), avoidance of certain acid suppressing agents, cost of medication and availability.
In order maximize posaconazole absorption, a posaconazole bundle should be co-implemented upon starting posaconazole (Table 2). This bundle consists of taking each posaconazole dose with a meal containing >20 g dietary fat, avoid use of proton pump inhibitors or cimetidine, limit each dose to 200400 mg and co-administer each dose with ascorbic acid 500 mg to transiently enhance gastric acidity. 20 Cost and insurance status may have the biggest impact on the patient use of posaconazole. Posaconazole remains under patent protection currently in the US while fluconazole and itraconazole both have generic formulations available. In addition, some insurance providers are likely to require a prior authorization before copayment is provided. These issues create an environment in which many pharmacies may not even carry the medication dependent upon the patient population that the pharmacy services.
Posaconazole bundle. 20
Place in Therapy
A recent review found there to be no difference in clinical cure rates between posaconazole and comparator in HIV-positive OPC patients. 17 However, only the study of treatment-naïve patients was included in this analysis.17,18 Posaconazole has gained regulatory agency approval in both the United States and Europe for treatment of first line and treatment-refractory OPC. The early generation triazole antifungals, fluconazole and itraconazole which have been used as comparators in many clinical trials have significant drawbacks. Fluconazole has poor activity against certain Candida spp. while itraconazole has a number of drug-drug interactions and variable bioavailability that changes based upon dosage form. Posaconazole has a narrow toxicity profile compared to older triazoles and, when used for extended period of time, potentially superior clinical outcomes. However, posaconazole exhibits variable bioavailability, is subject to many drug-drug and drug-nutrient interactions, and may carry a higher copay. Clinicians should be mindful that use of posaconazole as prophylactic treatment carries the potential for development of posaconazole resistant Candida spp., the treatment of which is poorly elucidated.
Posaconazole is an option for treatment of OPC in patients who experience fungal breakthrough while taking fluconazole or as first-line in patients who clinically fail prophylactic fluconazole therapy.
Author Contributions
JEW, EW, and MRG were responsible for data collection/synthesis/analysis and assistance with manuscript preparation. MRG was responsible for the design and preparation of the manuscript. All authors read and approved the final manuscript.
Funding
Author(s) disclose no funding sources.
Competing Interests
MRG has received payment from Merck for speaking on Aprepitant. Other authors disclose no potential competing interests.
Disclosures and Ethics
As a requirement of publication author(s) have provided to the publisher signed confirmation of compliance with legal and ethical obligations including but not limited to the following: authorship and contributorship, conflicts of interest, privacy and confidentiality and (where applicable) protection of human and animal research subjects. The authors have read and confirmed their agreement with the ICMJE authorship and conflict of interest criteria. The authors have also confirmed that this article is unique and not under consideration or published in any other publication, and that they have permission from rights holders to reproduce any copyrighted material. Any disclosures are made in this section. The external blind peer reviewers report no conflicts of interest. Provenance: the authors were invited to submit this paper.