
Abstract
Ruboxistaurin (Eli Lilly, Indianapolis, IN), an orally active inhibitor of the β isoform of protein kinase C (PKC), has been studied as a systemic treatment for diabetic retinopathy. PKC-β appears to be overactivated in response to hyperglycemia. This overactivation associates with various pathological effects within the retinal vascular system, including ischemia, vascular leakage, and angiogenesis. Several randomized clinical trials of ruboxistaurin have been performed. In most trials, the primary outcomes were not achieved. Analysis of secondary outcomes data from these trials has demonstrated some evidence of safety and efficacy in the treatment of diabetic retinopathy. At this time, ruboxistaurin has not received approval from the US Food and Drug Administration.
Keywords
Introduction
Chronic hyperglycemia in diabetes mellitus leads to the development of microvascular complications in different organs. Reducing the incidence and slowing the progression of diabetic-related microvascular complications remains a challenge. Two large randomized clinical trials (RCTs), the Diabetes Control and Complications Trial (DCCT), 1 and the United Kingdom Prospective Diabetes Study (UKPDS), 2 have established the importance of intensive glycemic control in reducing the occurrence and progression of diabetic vascular complications in type 1 and type 2 diabetes mellitus. Follow up data from the DCCT showed that the benefits of early intensive glycemic control on the development and progression of vascular complications persist for years despite deterioration in the level of control. This has been postulated to represent “metabolic memory” and it illustrates the chronic (years to decades) nature of the treatment and prevention of complications of diabetes. 3
An increased understanding of the pathophysiology of hyperglycemia-induced damage in diabetes has led to the development of new therapeutic agents to decrease microvascular complications. This review will highlight the role of protein kinase C (PKC) in diabetes and the efficacy and tolerability of a PKC β inhibitor, ruboxistaurin (Eli Lilly, Indianapolis, IN), in the treatment of diabetic retinopathy.
Protein Kinase C
PKC belongs to the superfamily of calcium- and/or lipid-activated serine-threonine kinase enzymes that are involved in the physiological regulation of intracellular signaling. In response to an extracellular signal (usually transduced through phospholipase C) PKC catalyzes the diacylglycerol (DAG)- and/or calcium-dependent transfer of a phosphate group from ATP to various substrate proteins, thereby modifying their function. 4 More than 10 different isozymes comprise the PKC family and are classified into three groups (conventional, novel, and atypical) according to their regulatory domain structure (Table 1).5,6
Different isoenzymes of protein kinase C.
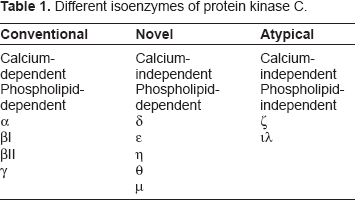
Chronic hyperglycemia is thought to lead to a pathologically elevated rate of synthesis of diacylgylcerol (DAG), which then activates one or more PKC isoforms in different tissues in an extracellular signal-independent manner. 7 Of the various PKC isoforms, PKC β and δ isoforms (aorta and heart), PKC-α, β2, and ε isoforms (retina) and PKC-α, β1, and δ isoforms (glomerulus) appear to be pathologically overactivated in diabetes.8,9
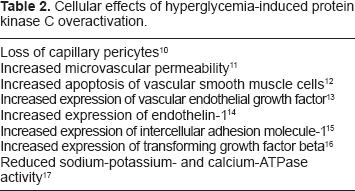
Hyperglycemia-induced PKC overactivation can lead to structural and functional changes in multiple tissues and organs (Table 2). 10 – 17
Cellular effects of hyperglycemia-induced protein kinase C overactivation.
PKC in Diabetic Retinopathy
Activation of PKC appears to play an important role in the development and progression of diabetic retinopathy (Table 3)14,15,18–21,23–25 PKC β is the dominant isoenzyme in the retina, 22 and its overactivation can often be detected early in diabetes before any clinically apparent diabetic retinopathy. 21
Protein kinase C and diabetic retinopathy.

Hyperglycemia-induced pathological chronic PKC overactivation can adversely affect vascular function through increased permeability, endothelial cell activation, alteration in blood flow, leukocyte adhesion, and abnormal growth factor signaling. In addition, PKC overactivation has been implicated in vascular dysfunction produced by hypertension 26 and the potential beneficial effects of statins and renin-angiotensin system blockers on the diabetic vasculature are both thought to be mediated, at least in part, by downregulation of PKC signaling.27,28 Thus, PKC appears to play a role in a wide array of the vascular abnormalities induced by diabetes. Insulin has been shown to regulate PKC β2 splicing in non-ocular cells. 29 PKC inhibition has therefore been approached as a systemic treatment for many complications of diabetes, including diabetic retinopathy.
PKC Inhibitors
Several compounds with inhibitory effects on PKC and non-PKC kinases have been studied in clinical trials for diabetic microangiopathies. Staurosporine and isoquinolinesulfonamide GF-109203X are first- and second-generation PKC inhibitors, respectively.30,31 Since these compounds inhibit PKC isoforms nonselectively, they are associated with systemic toxicity. Midostaurin is an orally available staurosporine derivative that showed some beneficial effects in diabetic macular edema; however, due to its toxicity, its clinical application for diabetes was excluded. 32 Ro-32-0432 is a PKC α-inhibitor that has been studied for diabetic nephropathy.33–35 JTT-010 is a PKC β-selective inhibitor that has been studied for diabetic neuropathy. 36 Ruboxistaurin (LY333531) mesylate is a selective antagonist of PKC βI and PKC βII. 37
Amongst various inhibitors of PKC, α- and β-inhibitors have been studied in detail in vitro and in vivo. Ruboxistaurin has shown the most potential in the prevention of diabetic vascular complications. 38 Ruboxistaurin acts as a competitive inhibitor by interacting with the ATP binding site. The mesylate monohydrate salt was chosen for its favorable bio-availability parameters. 39 Ruboxistaurin is metabolized by the liver to N-desmethyl ruboxistaurin (LY338522), which is also an effective inhibitor of PKC β. 37
Ruboxistaurin has shown promising preclinical results in animal models of diabetic retinopathy and macular edema.27,40 In animal models of proliferative retinopathy, ruboxistaurin has been reported to inhibit preretinal and optic nerve head neovascularization in a pig model of branch retinal vein occlusion 41 and to reduce the retinal neovascularization in an oxygen-induced retinopathy model in mice. 42
Ruboxistaurin: Efficacy
A phase 1 tolerability and pharmacokinetic study in healthy volunteers 43 was followed by a phase 1b pharmacodynamic study in patients with diabetes. 44 In patients with type 1 or type 2 diabetes and minimal or no evidence of diabetic retinopathy, 32 mg ruboxistaurin orally per day for 28 days produced a dose-dependent increase in retinal blood flow. Taken together, these studies indicated that ruboxistaurin was orally bioavailable and produced a pharmacological effect in the target organ of the retina.
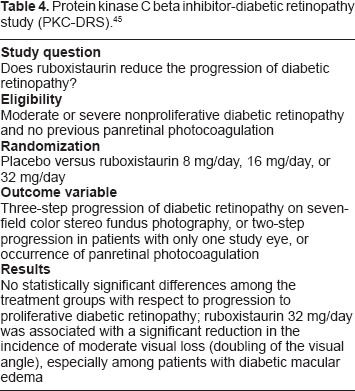
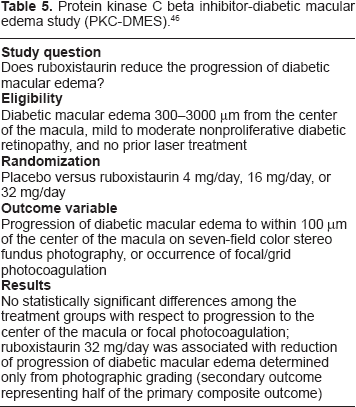
Two phase 2/3 RCTs of ruboxistaurin, the first in patients with moderate to severe nonproliferative diabetic retinopathy (NPDR) named the Protein Kinase C Beta Inhibitor-Diabetic Retinopathy Study (PKC-DRS, Table 4), 45 and the second in patients with mild to moderately severe NPDR and diabetic macular edema (DME) > 300 microns from the center of the macula named the Protein Kinase C Beta Inhibitor-Diabetic Macular Edema Study (PKC-DMES, Table 5), 46 were initiated in 1998 and completed in 2002. Both trials failed to achieve their primary outcomes, which were progression from NPDR to proliferative diabetic retinopathy (PDR) or panretinal photocoagulation in the PKC-DRS and progression of DME to within 100 microns of the center of the macula or focal photocoagulation in the PKC-DMES. Key secondary outcomes for which differences between ruboxistaurin and placebo did reach (PKC-DRS) or approach (PKC-DMES) statistical significance were moderate visual loss (a decline in 3 lines/15 letters in best-corrected ETDRS visual acuity) and progression of DME to within 100 microns of the center of the macula, respectively. In order to accommodate the change in hypothesis regarding ruboxistaurin's mechanism from being an inhibitor of DR progression to having effects to prevent vision loss and DME progression, the Protein Kinase C Beta Inhibitor–-Diabetic Retinopathy Study 2 trial (PKC-DRS 2) was modified to change the primary endpoint from DR progression to vision loss (Table 6). 47
Protein kinase C beta inhibitor-diabetic retinopathy study (PKC-DRS). 45
Protein kinase C beta inhibitor-diabetic macular edema study (PKC-DMES). 46
Protein kinase C beta inhibitor-diabetic retinopathy study 2 (PKC-DRS 2). 47
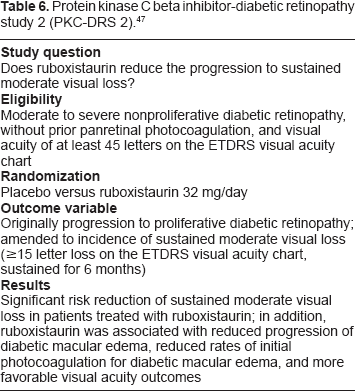
Following completion of the PKC-DRS2, all patients went off study drug for periods ranging from approximately 250 to 1300 days. Following the off-drug period, approximately 200 (of the originally randomized 685) patients entered an open-label extension where they received 32 mg/day ruboxistaurin for an additional 2 years. By the completion of the extension period (6 or more years post initiation of PKC-DRS2), approximately 28% of the patients who received placebo during PKC-DRS2 and ruboxistaurin only for the 2-year extension experienced a sustained 3 line loss of vision (using PKC-DRS2 initiation as baseline) versus only 6% of the patients who received ruboxistaurin during PKC-DRS2 and during the extension. 48 Thus, while the absolute treatment difference between ruboxistaurin and placebo in PKC-DRS2 was relatively modest (5.5% vs. 9.1% with sustained vision loss at 3 years), the results of the extension study suggest that vision loss may become a much bigger problem over longer durations of disease and that ruboxistaurin may have the potential to impact this.
There are two ongoing phase 3 clinical trials evaluating the effect of ruboxistaurin 32 mg/day on diabetic macular edema and vision loss.
Effect of Ruboxistaurin in Diabetic Nephropathy and Neuropathy
The therapeutic potential of ruboxistaurin has been evaluated in diabetic nephropathy and neuropathy as well.
In animal models of diabetic nephropathy, ruboxistaurin demonstrated benefit with reduction of albuminuria and adverse histological changes.48,49 A randomized, double-blind, placebo-controlled pilot trial of 123 subjects with type-2 diabetes and persistent albuminuria on angiotensin-converting enzyme (ACE) inhibitors or angiotensin II receptor blockers (ARBs) (or both) evaluated the effect of oral ruboxistaurin 32 mg on diabetic nephropathy. 50 During the study period, all patients were on either an ACE inhibitor or an ARB (or both) as well as optimum medical therapies to ensure tight control of glycemia and blood pressure. In the ruboxistaurin-treated group the urinary albumin/creatinine ratio (ACR) fell by 24% (±9%) compared with 9% (±11%) in the placebo group. There was also a slower decline in renal function, with the estimated glomerular filtration rate (eGFR) not declining significantly in the ruboxistaurin group (-2.5 ± 1.9 mL/min per 1.73 m2) but falling significantly (-4.8 ± 1.8 mL/min per 1.73 m2) in the placebo group. This pilot study was not powered to show a statistical significant difference between the ruboxistaurin and placebo groups, but did suggest that there could be a beneficial effect of ruboxistaurin on diabetic nephropathy and that an appropriately powered clinical trial is warranted to assess this further.
The effect of ruboxistaurin in symptomatic diabetic peripheral neuropathy has been examined in a multinational phase 2 RCT 51 A total of 250 patients with type-1 or type-2 diabetes were randomized to either 32 or 64 mg ruboxistaurin or placebo for 1 year. No change was seen in the primary endpoint of improvement in quantitative sensory testing for vibration detection threshold. However, in the 83 patients with clinically significant symptoms at baseline, there was a statistically significant reduction from baseline in a secondary endpoint, i.e. the Neuropathy Total Symptom Score 6 (NTSS-6), in the 64-mg ruboxistaurin group compared with placebo (P = 0.015). This suggests that treatment of patients with neuropathy with ruboxistaurin may reduce sensory symptoms. However, phase 3 studies of ruboxistaurin in patients with diabetic peripheral neuropathy did not meet their primary endpoints, at least in part due to a larger than expected placebo response rate. 52
Ruboxistaurin: Safety
Treatments with non-selective agents such as inhibitors of multiple kinases and PKC isoforms have been associated with side effects such as liver enzyme elevations, nausea, vomiting, and diarrhea. 53
Ruboxistaurin is a highly selective β-isoform inhibitor, and so far in clinical trials, few clinically significant systemic side effects have been identified. Over 1400 patients have now been treated with 32 mg per day ruboxistaurin for up to 4 years in controlled clinical trials that included patients with various microvascular complications due to diabetes. In all safety data combined from the phase 2 and phase 3 trials, there were fewer deaths in the ruboxistaurin-treated patients (21 patients, 1.5%) than in the placebo group (30 patients, 2.1%). 54 No death was reported to be due to the study drug. Adverse events were reported by 23.2% of placebo-treated patients compared with 20.8% of patients treated with ruboxistaurin 32 mg. Common (1%–10% of patients) adverse drug reactions occurring more frequently in ruboxistaurin-treated patients included dyspepsia and blood creatine kinase increases. An analysis of ECG results from >1500 patients in the phase 2 and 3 trials revealed a small increase in QT interval (corrected for heart rate using Bazett's method) of 2.4 ms. However, detailed analysis of adverse events related to repolarization abnormalities as well as other cardiac conditions did not reveal any clinical correlates of this ECG finding.
Conclusion
Hyperglycemia-induced PKC overactivation appears to play an important role in the pathogenesis of microvascular ischemia, leakage, and angiogenesis in diabetic retinopathy. Ruboxistaurin, an orally active β-selective PKC inhibitor is a generally well tolerated medication that has shown promising potential as therapy for prevention of vision loss due to diabetic macular edema in patients with diabetic retinopathy. Multiple phase 3 RCTs of ruboxistaurin have demonstrated reduction in visual loss and a reduced need for laser treatment in patients with moderate to severe nonproliferative diabetic retinopathy over a 3-year period. So far, there have been no significant concerns over the safety profile of ruboxistaurin in the clinical trials. While ruboxistaurin has not yet received approval from the US Food and Drug Administration (FDA), it is hoped that the ongoing phase 3 trials will provide sufficient additional efficacy data to support its approval.
Disclosures
This manuscript has been read and approved by all authors. This paper is unique and is not under consideration by any other publication and has not been published elsewhere. The authors and peer reviewers of this paper report no conflicts of interest, except as specified below. The authors confirm that they have permission to reproduce any copyrighted material.
Footnotes
Acknowledgement
Partially supported by NIH P30 Core Center Grant EY014801 and by an unrestricted grant to the University of Miami from Research to Prevent Blindness, New York, NY.
Lloyd Paul Aiello is a former consultant for Eli Lilly. Matthew J Sheetz is an employee of Eli Lilly.