
Abstract
Esomeprazole (S-omeprazole) is a single optical enantiomer proton-pump inhibitor (PPI) approved for the management of gastro-oesophageal reflux disease, the prevention and treatment of Non-Steroidal Anti-Inflammatory Drugs (NSAID) associated gastric ulcer disease, treatment of duodenal ulcer disease associated with Helicobacter pylori infection, and the treatment of Zollinger-Ellison syndrome. Esomeprazole has been shown to be safe and effective during pregnancy and was introduced to the market in 2001. PPI therapy may interact with clopidogrel by cytocrome 2C19. Clopidogrel is a prodrug which is partially activated by cytochrome 2C19 and esomeprazole is a competitive inhibitor of 2C19. Esomeprazole is more effective than other PPIs in controlling esophageal and gastric pH, but efficacy in symptom relief is less clear.
Keywords
Introduction
Proton pump inhibitors inhibit the gastric H+/K+-ATPase enzyme (the proton pump) and are the most potent suppressors of gastric acid secretion, diminishing daily production of gastric secretion and increasing intragastric pH.1,2 Five proton pump inhibitors are available clinically: omeprazole, esomeprazole, lansoprazole, rabeprazole, and pantoprazole,3–6 with a new PPI, tenatoprazole, having a 5- to 7-fold longer elimination half-life than other PPIs. 7 Esomeprazole, the S-isomer of omeprazole (a racemic mixture of S- and R- optical isomers), is the first proton pump inhibitor to be developed as a single optical isomer, has a better pharmacokinetic profile, and provides greater acid suppression than omeprazole. 8 Esomperazole is a white to slightly coloured crystalline powder, containing 3 water molecular of hydration. The solubility in water is 0.3 mg/ml. The pKa of benzimidazole (omeprazole base) is 8.8. The molecular mass of esomeprazole is 767.2 g/mol (trihydrate) and 713.1 g/mol (anhydrous bases). The molecular formula is C34H36N6O6S2MG•3H2O and the chemical name is Di –(s)-5-methoxy-2-[[(4-methoxy-3,5-dimethyl-2-pyridinyl)methyl]-sulfinyl]-1H-benzimidazole magnesium trihydrate. 9 This article reviews the pharmacological profile, tolerability, safety, and efficacy of esomeprazole, It also provides an update on the use of the drug in common clinical practice as well its use in rare conditions such as Zollinger-Ellison syndrome.
Mechanism of Action, Metabolism, and Pharmacokinetic Profile
Mechanism of action
Like other PPIs, esomeprazole suppresses gastric acid secretion from gastric parietal cells. Esomeprazole is a weak base that is concentrated in the acidic environment of parietal cells and converted to the active inhibitor, achiral sulphonamide. This inhibitor binds irreversibly to specific cysteines, resulting in an inhibition of H+/K+-ATPase enzyme activity. 10 Inhibition of gastric acid secretion is dose dependent, being observed in the range of 20–40 mg/day. 11
Metabolism and pharmacokinetic profile
Esomeprazole is rapidly absorbed orally, with a peak concentration in the plasma (Cmax) occurring at 0.5 h post-administration with an oral solution containing 20 mg, and after up to 3.5 h with a 40 mg capsule. 12 The bioavailability of the drug is 64% and is highly dependent on concomitant food intake, which delays and decreases absorption but does not appear to have an effect on intragastric acidity. 13
PPIs are metabolized via hepatic cytochrome P450 enzymes, primarily CYP2C19. 14 Both optical isomers of omeprazole are converted to hydroxyl and 5-0-desmethyl metabolites by the CYP2C19 isoenzyme, and to the sulphone by CYP3A4. 15 Approximately 80% of the drug is eliminated by the kidney and the rest through feces. 14 Esomeprazole is metabolized more by CYP3A4 than CYP2C19, 15 has a lower total intrinsic clearance than omeprazole and the R-isomer, and shows less first-pass metabolism than omeprazole. Esomeprazole therefore shows a higher area under the plasma concentration-time curve (AUC) and may achieve better acid suppression than omeprazole in clinical practice.14,15
CYP2C19 affects PPI metabolism. 16 CYP2C19 activity is influenced by gene polymorphisms, with two inactivating mutations occurring most commonly in Asian populations. 17 Five percent of Caucasians are homozygous for this mutation, exhibiting a poor metabolizer phenotype. Bioequivalence data for esomeprazole indicates that area under the curve (AUC) values differ by less than two-fold between poor metabolizers and the rest of the population, and a dose reduction is not necessary in these individuals. 18
Esomeprazole shows similar pharmacokinetics in the elderly 19 or in patients with renal impairment 20 or mild to moderate hepatic impairment. However, esomeprazole levels increase in patients with severe hepatic impairment. 21 Esomeprazole is available as a tablet, capsule, and oral suspension, with similar absorption for all three,22,23 as well as for intravenous usage. 24
Esomeprazole has a low potential for interaction with other drugs, 14 but may interact with inducers or inhibitors of CYP2C19 and CYP3A4, such as voriconazole and clarithromycin, which can double esomeprazole systemic exposure. Esomeprazole may also interfere with gastric absorption that is influenced by gastric pH (e.g. ketoconazole, iron salts, and digoxin), and international normalized ratio (INR) may need to be monitored if given with warfarin.25–27 Esomeprazole may increase the plasma concentration of diazepam phenytoin, warfarin, cisapride, digoxin and may reduce plasma levels of antiretroviral agents (atazanavir, nelfinavir, ininavir, lopinavir and tipranavir). However, none of those drug interactions were clinically relevant.28,29
Clopidogrel is prodrug which is converted to active metabolites by CYP2C19. PPIs may interfere with clopidogrel function via CYP2C19,30,31 which could lead to cardiovascular events.32,33 A 40% relative increase in the risk of recurrent myocardial infraction was observed in a case-control study 34 but other studies did not reveal any drug-drug interactions.35,36 Omeprazole is the PPI most likely to have a significant interaction with clopidogrel but more studies are needed to determine that the clinical implications of that interaction. 37
The effect of esomeprazole on serum gastrin was evaluated in approximately 2700 patients in clinical trials for up to 8 weeks and in over 1300 patients for up to 12 months. The mean gastrin level plateaued within 3 months and returned to baseline within 4 weeks after discontinuation of therapy. 38
Clinical studies
Several studies have compared the effects of esomeprazole and other PPIs in gastro-esophageal reflux disease (GERD) management as well peptic ulcer disease. Below the efficacy of esomeprazole has been updated in common gastrointestinal disorders and NSAID-induced gastric ulcer disease, as well as non-ulcer dyspepsia, non-variceal upper gastrointestinal bleeding, and Zollinger-Ellison syndrome.
GERD
GERD is characterized by the reflux of gastric contents into the esophagus, leading to reflux symptoms sufficient to affect patients’ well being and/or cause complications. 39 Esomeprazole efficacy and activity on intra-esophageal pH profiles have been compared to other PPIs.40,41 One study compared 40 mg of esomeprazole to 30 mg of lansoprazole in 30 patients with complicated GERD. 42 Esomeprazole was superior to lansoprazole in both total (75% vs. 28%, P = 0.026) and supine position (93% vs. 50%, P = 0.012) nocturnal esophageal acid exposure. 42 A number of randomized, double blind, multicenter trials have compared the effects of esomeprazole with other PPIs in erosive GERD using intent-to-treat analysis of healing rates and GERD symptoms (Table 1).43–50 All patients had endoscopy to confirm erosive GERD at baseline and most of them had a follow-up endoscopy 4 and 8 weeks later. The Los Angeles (LA) classification system was used to grade the severity of reflux esophagitis. 51 The main exclusion criteria were other gastrointestinal diseases, or severe or unstable cardiovascular, pulmonary, or endocrine diseases.
The efficacy of esomeprazole vs. other PPIs in the management of erosive gastroesophageal reflux disease.
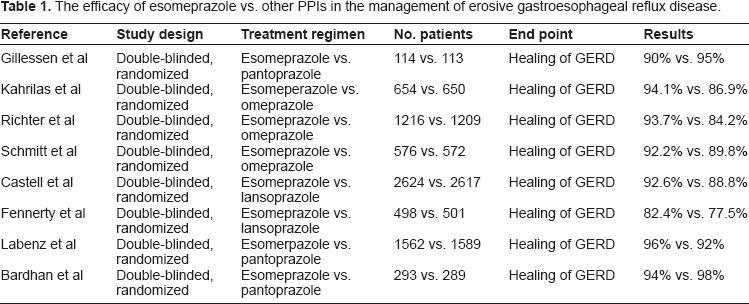
Two studies compared esomeprazole to lansoprazole.47,48 Esomeprazole (40 mg, n = 2624) showed a higher healing rate and was more effective then lansoprazole (30 mg, n = 2617) in resolving heartburn. 47 A smaller study (total n = 999) showed similar outcomes. 48 Two studies indicated that esomeprazole had a higher healing rate and better symptom control than omeprazole in mild reflux esophagitis,44,45 but a third one did not, 46 although esomeprazole was superior to lansoprazole at 4 weeks (60.8% vs. 47.9%, P = 0.02) and 8 weeks (88.4% vs. 77.5%, P = 0.007) in patients with moderate to severe esophagitis. Esomeprazole may have a better effect in more severe disease than other PPIs.47,49 In one trial, 3170 patients were randomly assigned to either esomeprazole or pantoprazole. Esomeprazole had higher healing rates than pantoprazole at 4 weeks (81% vs. 75%, P < 0.001) and 8 weeks (96% vs. 92%, P < 0.001) and provided better resolution of GERD symptoms, 49 but there was no difference in another study.43,46
Heliobacter pylori infection did not affect the healing rates in multiple studies after 8 weeks of treatment,38,45–47,52 but other studies showed that H. pylori-positive patients may have higher healing rates.49,50 Several meta-analyses showed that esomeprazole had higher healing rates than other PPIs,53–58 particularly for severe esophagitis, producing numbers needed to treat for LA grades A, B, C, and D of 50, 33, 14, and 8, respectively. 57
Maintenance therapy of healed erosive GERD
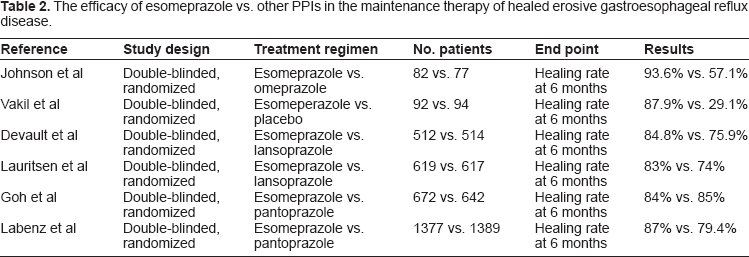
Patients with severe erosive esophagitis have a higher relapse rate than patients with moderate or mild disease, but the overall relapse rate is 80% within 12 months of stopping therapy.59,60 Another study found that 20% of GERD patients could discontinue their PPIs without developing symptoms. 61 Esomeprazole 40 mg is superior to 20 mg and 20 mg superior to placebo in maintenance therapy for patients with healed erosive GERD.62,63 In one study, 375 patients with endoscopically healing esophagitis were randomized to receive esomeprazole (40 mg, 20 mg or 10 mg od) or placebo. 63 After 6 months, more patients remained healed with esomeprazole 40 mg (87.9%), 20 mg (78.7%), and 10 mg (52.4%) compared to placebo (29.1%) (P < 0.001). Esomeprazole (20 mg) was more effective in maintaining therapy than lansoprazole (15 mg) 6 months after endoscopy-confirmed healing. 64 A similar second study found 83% of the esomeprazole group was in remission compared to 74% of the lansoprazole group at 6 months (P < 0.0001), and more patients were symptom-free. 65 Esomeprazole was superior to pantoprazole in one study, but not another, in maintaining healed erosive esophagitis and relief of gastroesophageal symptoms (Table 2).66,67 Heartburn relapse rates after esophagitis were lower with esomeprazole than pantoprazole (ratio 2.08; P < 0.0001). 68
The efficacy of esomeprazole vs. other PPIs in the maintenance therapy of healed erosive gastroesophageal reflux disease.
Barrett's esophagus
Barrett's esophagus results from long standing GERD and is an important risk factor for esophageal adenocarcinoma.69,70 In a study involving 41 patients with Barrett's esophagus that received open-label consecutive treatment with esomeprazole and lansoprazole with no washout period, 24-h intragastric pH was measured on the last day of each treatment. 71 Esomeprazole was more effective in controlling the intragastric pH, measured as the time with intragastric pH > 4.0, in patients with Barrett's esophagus (P = 0.016).
Laryngopharyngeal reflux disease
On a recent double blind, prospective, randomized trial, 62 patients with laryngopharyngeal reflux disease (LRP) were randomized to either esomeprazole 20 mg PO BID or placebo for 3 months. The total reductions of the reflux finding score and reflux of symptom index were higher in the esomepraozle group compared to placebo after three months (P < 0.01). 72 However, in the treatment group a high placebo effect can be observed. In another study, the efficacy of esomeprazole 40 mg once daily together with lifestyle modification was determined in 49 patients by 24 hours pH monitoring before and after treatment. 73 In conclusion, esomepraozle 40 mg once daily with life style modification may improved LRP disease. On the other hand, one study showed no therapeutic benefit of esomeprazole (40 mg) once daily for 16 weeks compared to placebo in patients with laryngopharyngeal reflex disease. 74 The diagnosis of LRP is still controversial and the treatment with PPI therapy is based on weak evidence. 75
Eosinophilic esophagitis
Although topical or oral steroids have been assessed in eosinophilic esophagitis, 76 only one study compared the efficacy of esomeprazole to fluticasone. This small study (n = 41) did not show improvement in dysphagia or eosinophilic infiltrate with esomeprazole therapy. 77
Non-erosive reflux disease
PPIs are the first line therapy in patients with functional dyspepsia or non-erosive reflux esophagitis. Rabeprazole had similar efficacy to esomeprazole in suppressing GERD-related symptoms in Asian patients with non-erosive esophagitis. 78 Esomeprazole and omeprazole gave similar symptom-free (heartburn) outcomes (60% of patients) in endoscopy negative reflux disease at 4 weeks. 79 Esomeprazole and pantoprazole showed similar symptom relief in daily assessments using a questionnaire. 80 Esomeprazole was more effective then placebo in the resolution of heart burn and time to symptom-free status. 81
On-demand therapy
Most patients with GERD will have symptom relapse within a year.59,60 Esomeprazole (20 mg) was superior to placebo for on-demand therapy in patients with endoscopy–-negative GERD.82,83 In those studies, patients received 4 weeks of esomeprazole or omeprazole and then were randomized to placebo or esomeprazole groups after they had achieved complete resolution of heartburn and had a normal endoscopy. Esomeprazole was more effective in controlling heartburn and less patients discontinued therapy compared to placebo due to inefficacy.82,83 Esomeprazole (20 mg) on-demand therapy was economically more effective then lansoprazole 15 mg daily after 6 months in endoscopy-negative GERD. 84 Patients received a short course of esomeprazole for 4 weeks and then were randomized to continue therapy with lansoprazole or on-demand therapy with esomeprazole. Esomeprazole showed better symptom control and more patients were willing to continue on-demand therapy than use lansoprazole on daily basis (93% vs. 88%, P < 0.02). On demand therapy required treatment only 38% of the time, producing direct cost savings of 36%. Daily esomeprazole (40 mg) showed better efficacy than an on-demand regimen: 81% of patients on daily therapy were still in remission compared to 58% who took on-demand therapy 6 months after endoscopy-confirmed healing (P < 0.0001). 85
Uninvestigated dyspepsia and health-related quality of life
The efficacy of esomeprazole in uninvestigated dyspepsia was assessed in two studies86,87 by evaluating if one week of esomeprazole could produce a response at 8 weeks in patients with functional or uninvestigated dyspepsia. Patients were randomized to either 40 mg od, bid, or placebo for one week followed by esomeprazole 40 mg po od or placebo for 7 weeks. Patients rated the severity of their symptoms (epigastric pain and/or burning) on a daily basis. The primary efficacy endpoint in both studies was the percentage of patients who responded after 8 weeks of treatment, as a function of the sum of symptom scores during the first week of acid suppression. Esomeprazole was more effective then placebo in symptom control at 4 and 8 weeks, but the response to esomeprazole treatment at one week did not predict the clinical response at 8 weeks.
Patients with GERD experience impaired health-related quality of life and are less productive compared to the general population,88–91 especially patients with night symptoms. 89 Esomeprazole can improve quality of life and work productivity.91–94 GERD patients (n = 1902) were treated for 4 weeks with esomeprazole (40 mg od) followed by 6-month treatment with 20 mg of esomeprazole od, on demand therapy, or ranitidine 150 mg bid. 92 Both esomeprazole treatments were more effective than ranitidine in improving the quality of life and patient satisfaction (80.2% vs. 77.8% vs. 47%; P < 0.001). Short-term therapy with esomeprazole for 4 weeks was more effective then placebo in improving sleep quality and saved more work hours per week than at baseline (11.6 h vs. 6.2 h; P < 0.001). 94
H. pylori eradication and prevention
Esomeprazole is effective in intragastric acid control and eradication of H. pylori,95,96 and is more effective than other PPIs in controlling intragastric pH in healthy volunteers.1,95 The IV formulation of esomeprazole provides faster and more effective intragastric acid control than 40 mg of IV pantoprazole. 97 In one of the studies, 24 H. pylori-negative subjects were randomized in a two-period crossover study: tenatporazole or esomeprazole 40 mg daily were given before breakfast for 2 consecutive days with a 2-week wash out period. Tenatoprazole showed better efficacy than esomeprazole on intragastric acid control during the first 48 h in healthy volunteers (median pH: 4.3 vs. 3.9, P < 0.08; percent of time above pH 4: 57% vs. 49%, P < 0.03; proportion of subjects with at least half of the time above pH 4: 71% vs. 46%). Tenatoprazole has better night-time acid control than esomeprazole (first night median pH: 4.2 vs. 2.9, P < 0.0001; second night: 4.5 vs. 3.2, P < 0.0001) but acid control was similar during the day. 98 In a similar study comparing tenatoprazole to esomeprazole 40 mg once daily for 7 days in controlling the intragastric pH in healthy volunteers, tenatoprazole was more effective than esomeprazole in acid inhibition (24 h median pH: 4.6 vs. 4.2, P < 0.05; night time: 4.7 vs. 3.6, P < 0.01). 99 In an open label, crossover study of 130 patients with symptoms of GERD received esomeprazole 40 mg or omeprazole 40 mg once daily for 5 days. The 24-hr intragastric pH was monitored in day 1 and 5 of each treatment. Esomeprazole was more effective than omeprazole in acid control (mean percent of pH on day one: 48.6% vs. 40.6%, day 5: 68.4% vs. 62%, P < 0.001). 100
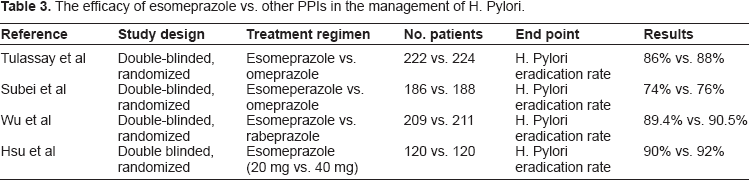
First-line treatment for H. pylori infection is triple therapy with a PPI, amoxicillin/metronidazole, and clarithromycin. Esomeprazole-based triple therapy induces H. pylori eradication and healing of duodenal and gastric ulcers.96,101 H. pylori patients (n = 446) with active duodenal ulcer disease were randomly assigned to esomeprazole 20 mg BID or omeprazole 20 mg BID in combination with amoxicillin 1 gram and clarithromycin 500 mg for one week, followed by continuation of omeprazole or placebo for the esomeprazole group. Ulcer healing was assessed by EGD after completing the therapy and H. pylori status was assessed by the C-urease breath test and histology 4–6 weeks later. Ulcer healing rates were similar: 91% for esomeprazole versus 92% in the omeprazole group, and H. pylori eradication rates of 86% in the esomeprazole group compared with 88% in the omeprazole group (Table 3). 101 Similarly, a one-week regimen of esomeprazole-based H. pylori therapy was as effective as omeprazole-based triple therapy followed by an additional 3 weeks of monotherapy for duodenal ulcer healing and eradication of H. pylori. 102 Esomeprazole-based triple therapy led to H. pylori eradication, ulcer healing, and prevented relapse. 96 High and low-dose esomeprazole triple therapy in Taiwanese patients showed similar H. pylori eradication rates (92% high dose vs. 90% low dose, P > 0.05). 103 Esomeprazole and rabeprazole showed similar efficacy in H. pylori eradication (89.4% esomeprazole vs. 90.5% rabeprazole, P = 0.72). 104 A meta-analysis of PPIs in eradication of H. pylori included 11 trials and 2159 subjects, showing eradication rates with esomeprazole and antibiotic of 86% and 81%, an odds ratio of 1.38 (95% CI = 1.09–1.75). 105 A similar result was obtained from another meta-analysis. 106
The efficacy of esomeprazole vs. other PPIs in the management of H. Pylori.
Non variceal bleed
Patients (n = 70) with active bleeding ulcers or ulcers with non-bleeding visible vessels were treated with epinephrine injection followed by thermocoagulation and treated with esomeprazole 40 mg po BID for 3 days or placebo.107,108 Bleeding reoccurred within 30 days in 2 patients (5.7%) in the esomeprazole group compared to 3 (8.6%) in the placebo group (P = 0.999), and blood transfusion requirements and the duration of hospitalization were similar. 108 Intravenous esomeprazole after endoscopic therapy in patients with high risk peptic ulcer disease was more effective than placebo in reducing the risk of recurrent bleeding at 7 and 30 days (P = 0.012), although endoscopic therapy was not completely standardized and some patients received monotherapy with an epinephrine injection, thermal coagulation, or hemoclips, and others received combination therapy. 107
NSAID-associated gastrointestinal symptoms and gastric ulcer healing or prevention
NSAIDs are often associated with upper gastrointestinal symptoms, including heartburn and acid regurgitation, and esomeprazole controls these symptoms.109–111 Two studies (NASA1, n = 794; and SPACE1, n = 848) recruited patients taking NSAIDs that were free of peptic ulcer, erosive esophagitis, and H. pylori. Patients received 4 weeks of esomeprazole (20 or 40 mg) or placebo once daily. Patients reported their GI symptoms (pain, discomfort, or burning in the upper abdomen) 7 days before therapy and in the last 7 days using a score sheet for severity. Symptom improvement was 2.3 on esomeprazole (20 mg) and 2.03 on 40 mg versus 1.84 in placebo in the NASA1, and 2.17 on 20 mg, 2.12 on 40 mg, and 1.56 in placebo (P < 0.001). 109 In another study, heartburn resolved in 61% and 62% of the patients taking esomeprazole 20 and 40 mg with NSAID compared with 36% on placebo (P < 0.001). Acid regurgitation resolved in 65% and 67% in the esomeprazole 40 and 20 mg groups compared to 48% in the placebo group (P < 0.001). 111 Esomeprazole was more effective then placebo in preventing symptoms for 6 months in patients taking NSAIDs or selective cyclo-oxygenase-2 (COX-2) inhibitors. Symptom relapse was higher in the placebo group (39.1%) than the 20 mg esomeprazole group (29.3%) (P = 0.006) and 40 mg group (26.1%) at 6 months of treatment (P < 0.001). 110
In one study, patients with gastric ulcer confirmed by EGD and receiving non-specific or COX-2-selective NSAIDs were randomly assigned to esomeprazole 20 mg or 40 mg or ranitidine for 8 weeks. Gastric ulcer healing was confirmed at 4 weeks by EGD and the healing rate at 8 weeks was 91.5% with esomeprazole 40 mg vs. 88.4% with 20 mg vs. 74.2% with ranitidine (P < 0.05). 112 A second study compared endoscopic healing rates at 4 and 8 weeks after treatment with esomeprazole 20 or 40 mg once daily or ranitidine 150 mg twice daily in patients (n = 444) with gastric ulcer confirmed by EGD and receiving cyclooxygenase-2-selective or non-selective NSAID therapies. The gastric ulcer healing rate at 8 weeks was 85.7% in the 40 mg esomeprazole group vs. 84.8% for 20 mg esomeprazole vs. 76.3% in the ranitidine group, with esomeprazole superior to ranitidine at 4 weeks (P < 0.01). 113
Esomeprazole also reduces the risk of gastric ulcer formation in patients using nonselective NSAIDs and COX-2 inhibitors (Table 4).114,115 Gastroduodenal ulcer free patients (n = 991) on daily aspirin were randomly assigned to esomeprazole 20 mg or placebo for 26 weeks; 27 patients (5.4%) in the placebo group developed gastric or duodenal ulcers compared to 8 patients (1.6%) in the esomeprazole group (P < 0.0007). 114 In two similar studies (VENUS and PLUTO), patients over 60 years old and with an ulcer history using non-selective NSAIDs or COX-2 inhibitors received esomeprazole 20 or 40 mg or placebo daily for 6 months. For VENUS, 20.4% of patients developed an ulcer at 6 months on placebo, 5.3% on esomeprazole 20 mg (P < 0.001), and 4.7% on esomeprazole 40 mg (P < 0.0001). The PLUTO study found 12.3% on placebo, 5.2% on esomeprazole 20 mg (P = 0.018), and 4.4% with esomeprazole 40 mg (P = 0.007). 115 The combination of ASA and esomeprazole was superior to clopidogrel alone in prevention of recurrent ulcer bleeds in 2 studies performed in Hong Kong.116,117
The efficacy of esomeprazole in the management NSAID-associated gastrointestinal symptoms and gastric ulcer healing or prevention.
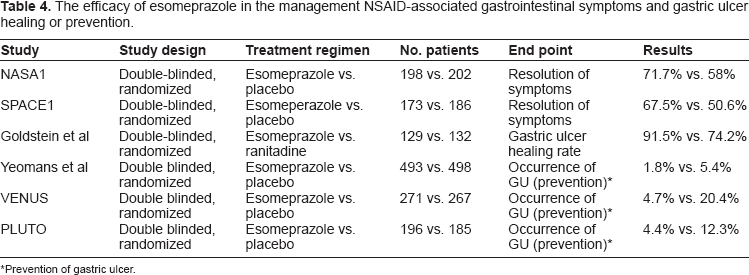
Prevention of gastric ulcer.
Zollinger Ellison syndrome
Zollinger Ellison Syndrome is characterized by ulceration of the proximal jejunum, hypersecretion of gastric acid, and non-beta islet cell tumors of the pancreas. 118 An open-label, multicenter study using 40 mg or 80 mg esomeprazole twice a day measured acid output at baseline, day 10, and at months 3, 6, and 12. 119 EGD was performed at baseline and at 6 and 12 months. Esomeprazole was titrated up to 240 mg/day to achieve better control of the acid output, and no patients had endoscopic evidence of mucosal disease at 6 or 12 months. One patient developed a serious adverse event (hypomagnesaemia).
Safety
The safety of esomeprazole has been evaluated in several trials. 57 Long term use of PPIs may lead to hypomagnesemia120,121 via an unclear mechanism probably involving an idiosyncratic reaction or inhibition of the magnesium transporter in the intestine. 120 Esomeprazole may also lead to vitamin B12 deficiency, but the data are conflicting,25,121,122 and it is less likely that esomeprazole leads to atrophic gastritis. 38 Esomeprazole may influence the absorption of calcium carbonate, 123 and its effect on iron absorption is not clear.124,125
The safety of esomerpazole has been evaluated in the primary care setting of 11595 patients in England using prescription event monitoring. 126 Several adverse events were reported in the observational cohort study (diarrhea 3/1000, nausea and vomiting 2/1000, abdominal pain 3/1000, dyspepsia 4/1000, headache and migraine 2/1000, respiratory tract infection 3/1000, malaise and joint pain 1/1000). 126 The safety of esomeprazole has been evaluated in the short (8 weeks) and long term (up to one year), with similar rates of adverse events reported (diarrhea 6%, headache 7%, flatulence 3%, constipation 2%, dry mouth 1%, respiratory infection 4%, sinusitis 2%, pharyngitis 1%, dizziness 1%).9,45,62,64,67,96 In addition to these adverse events, other symptoms have been reported in longer follow up (urinary tract infection 3.7%, allergy 2.1%, bronchitis 3.6%, arthralgia 3%, hypertension 3%, insomnia 2.1%, dyslipidemia 2%, anxiety 2%, flu-like disorder 1%, myalgia 1% and fever 1.5%).9,45,62,64,67,96
The use of PPIs by pregnant women is not associated with increased risk of congenital malformation or birth defects,127–129 and esomeprazole is a class B drug. A meta-analysis of PPI use in the first trimester using the Mantel-Haenszel method to calculate relative risk and 95% confidence intervals revealed a relative risk of 1.18 (95% CI, 0.72–1.94) for major malformations after PPI exposure. Omeprazole had an overall malformation rate of 2.8%. 127
Gastric acid plays an important role in facilitating the absorption of calcium. 130 Long term or high dose PPI therapy increases the risk of hip fracture,131,132 but this risk is lower in patients without major risk factors for osteoporosis. 133 In a prospective study of 1211 postmenopausal women, omeprazole was associated with an increased risk of vertebral fractures (RR = 3.50, 95% CI 1.14–8.44). 134 Further studies are needed to assess the relationship between esomeprazole and osteoporosis.
Decreased gastric acidity increases gastric bacteria levels, and PPIs may increase the risk of developing Clostridium difficile diarrhea (C. difficile).135,136 Patients (n = 1187) that received PPIs and antibiotics for 9 months showed more C. difficile diarrhea (CDAD; adjusted OR 2.1, 95% CI 1.2–3.5), 137 but other studies did not show that effect.138,139 In a prospective study designed to evaluate the incidence of nosocomial CDAD and a case-control study to determine the risk factors for the disease. A total of 1703 episodes of CDAD were observed among 1719 patients at 12 hospitals, with an incidence rate of 22.5/1000 admissions. Exposure to PPIs was not significantly associated with development of CDAD. 139
Several studies assessed the association between PPI therapy and risk of developing community acquired pneumonia.140–142 The risk to benefit ratio favors using acid suppressive therapy for conditions in which efficacy has been demonstrated. 143 In a retrospective analysis of thirty one studies, there was no casual association between esomeprazole and increase the risk of community acquired pneumonia. 142
Long term PPIs therapy may stimulate the enterochromaffin-like (ECL) cell proliferation and increase the ECL mass even after discontinuation of therapy. This will lead to increase in the gastric acid production until there is a normalization of the ECL mass (2–3 months after stopping therapy).144,145 Withdrawal of PPI therapy in patients with reflux esophagitis may lead to worsening of there symptoms due to rebound acid hypersecration.146,147 In a randomized, double blind, placebo controlled trial of 120 healthy volunteers, withdrawal of PPI therapy after 8 weeks of treatment was associated with acid related symptoms comparable to placebo. 148 However, there was no strong evidence for a clinically relevant increased of acid production after withdrawal of PPI therapy in a systemic review of 8 studies due to heterogeneity in design, methods and outcome. 149 Further studies are required to assess the causality of symptoms due acid hypersecretion and withdrawal of esomeprazole therapy.
Conclusions
PPI therapy is more effective than other acid suppressive therapies. Esomeprazole is more effective for control of esophageal and gastric acid than other PPIs. However, it is not more effective clinically except in patients with severe esophagitis. Esomeprazole (S-omeprazole) is a single optical enantiomer proton-pump inhibitor (PPI) and the rational of developing this drug was its higher metabolic stability, which will lead to a higher bioavailability and increase in the area under the plasma concentration-time curve (AUC), which will provide more effective control of gastric acid secretions compared to other PPIs therapy. Esomeprazole is converted to the active metabolite (achiral sulphanomide) by the presence of the acidic environment through parietal cells and it will inhibit H+/K+-ATPase activity. The efficacy of esomeprazole in clinical practice compared to omprazole is unclear. However, in one study, esomerpazole was a slightly weaker inhibitor of CYP2C19 compared to omeprazole, which would favor the use of esomprazole although the potential for drug interaction in practice is similar between these two agents. This could be explain by the higher standard dose used for esomeprazole (40 mg) compared to omeprazole (20 mg) resulting in a higher plasma exposure level. 150
Esomeprazole can treat gastric acid disorders and help maintain remission, but the cost-effectiveness is unclear. Esomeprazole 40 mg daily is more effective for healing gastric ulcers in patients with NSAID therapy compared to ranitidine 150 mg twice daily at 8 weeks (91.5% vs. 74.2%, P < 0.05). 112 A meta-analysis of 11 studies, compared the efficacy of PPI therapy to ranitidine in treating patients with bleeding peptic ulcers. 151 Persistent or recurrent bleeding was lower in the PPI therapy group compared to the ranitidine group (6.7% vs. 13.4%, P = 0.09) and the need for surgical intervention was lower as well in the PPIs group (5.2 vs. 6.9, P = 0.09). Esomeprazole may interact with clopidogrel, but the data are conflicting.
Esomeprazole is generally well tolerated. PPI therapy is effective and safe during pregnancy, but the long-term effects on the gastric mucosa are unclear and may include achlorhydria and carcinoid tumor. PPI therapy can be chosen based on several factors, including doctor preference, patient tolerance, symptomatic response, and cost.
Disclosures
This manuscript has been read and approved by all authors. This paper is unique and is not under consideration by any other publication and has not been published elsewhere. The authors and peer reviewers of this paper report no conflicts of interest. The authors confirm that they have permission to reproduce any copyrighted material.