
Abstract
Dexlansoprazole MR is a modified release formulation of the R-enantiomer of lansoprazole, which employs a novel Dual Delayed Release (DDR) technology. Pharmacokinetic studies have shown that the DDR technology provides a two peaks drug release, accuring 1–2 hours and 4–5 hours after dosing, leading to an extended duration of therapeutic plasma drug concentrations compared with conventional delayed release lansoprazole. Dexlansoprazole MR 30 and 60 mg provided superior intragastric pH control compared to that obtained with lansoprazole 15 mg and 30 mg once daily dosing. Dexlansoprazole can be taken without regard to food. The drug has been shown to be as efficacious as lansoprazole in healing, and superior to placebo in maintaining healing, of erosive esophagitis. Dexlansoprazole appears to be well tolerated with a comparable safety profile to lansoprazole. Overall, dexlansoprazole DR has an interesting pharmacokinetic profile and is effective and well tolerated in the healing and maintenance of erosive esophagitis and in the treatment of GERD. Nevertheless in the absence of head-to-head comparison there is no mean to recommend its use preferentially to other PPIs.
Keywords
Introduction
Gastro-esophageal reflux disease (GERD) is the abnormal reflux of gastric contents into the esophagus, leading to symptoms and/or esophageal damage. Esophageal symptoms of GERD include persistent heartburn, belching, hoarseness, sore throat, and changes in the voice. Extra esophageal symptoms may include cough, wheezing, shortness of breath, early satiety, hiccups, and non-cardiac chest pain. 1 If GERD is untreated or inadequately treated, the condition may predispose patients to serious complications, such as erosive esophagitis (EO), Barrett's esophagus and adenocarcinoma.2–4 Long-term treatment with a proton pump inhibitor (PPI) is recommended by the American College of Gastroenterology in patients with healed EO to maintain healing, control symptoms and preserve quality of life improvements achieved by initial treatment. 5 However, there is a consensus that about 30% of GERD patients failed to obtain complete healing and/or symptom resolution after a standard course of PPI therapy. 6
Proton pump inhibitors are potent inhibitors of gastric acid secretion because they irreversibly block the final common path of acid production, the activated proton pumps. 7 To be most effective, PPIs must be present in therapeutic concentration over 24 hours, thereby inhibiting over all the day newly activated proton pumps that turn over following initial PPI inactivation of H+/K+-ATPase. When they are given once daily, and because of their short half life (1 to 2 hours), they maximally inhibit approximately 70% of proton pumps and do not completely control acid secretion over 24 h. 8 Furthermore, pump turnover has a great inter-individual variability, and it is more difficult to inhibit gastric secretion in patients with a great proton pump turnover, compared with those whose pumps turn over more slowly. 9 Several approaches have been employed to extend the acid control of PPI. Increasing the dose of once daily PPI has been tested. The few studies that have evaluated this approach have shown marginal benefit.10,11 Twice-daily dosing has also been tested, as an option for patients who do not respond to a standard course of PPI therapy. However, increasing dosing frequency has been shown to reduce adherence to treatment regimens.12,13 Once-daily dosing is the preferred mode of administration, supporting the need for a once-daily PPI with an increased residence time in the systemic circulation, and a better pharmacokinetic/pharmacodynamic profile. 14
Dexlansoprazole MR (TAK-390MR, Takeda Global Research and Development Center, Inc., Deerfield, IL, USA) is a modified release formulation of dexlansoprazole, the R-enantiomer of lansoprazole, which employs a novel Dual Delayed Release (DDR) technology, formulated to extend the duration of acid suppression. Dexlansoprazole MR capsules contain a mixture of two types of granules, each providing a different pH-dependent dissolution profile. It provides a dual-peak PK profile, associated with 2 distinct releases of mediation.15,16
This article reviews the mechanism of action, the pharmacokinetic profile, the safety and efficacy and the place in therapy of dexlansoprazole in patients with EO and GERD.
Mechanism of Action
Dexlansoprazole MR is a novel modified-release formulation of dexlansoprazole, the R-enantiomer of lansoprazole. Lansoprazole and its enantiomers are equipotent in inhibiting H+, K+-ATPase proton pump in their activated form, in the gastric parietal cells. This enzyme inhibition blocks the final steep in acid production. 7
However, dexlansoprazole constitutes >80% of circulating drug following oral administration of lansoprazole. Moreover, its clearance is lower than that of lansoprazole. 17 Therefore, dexlansoprazole was selected for further clinical development.
Pharmacokinetic Profile
Dexlanzoprasole MR employs an innovative delivery system with dual delayed released technology. It is designed to provide an initial drug release in the proximal small intestine 1 to 2 hours after administration followed by another drug release at more distal regions of the small intestine several hours later.
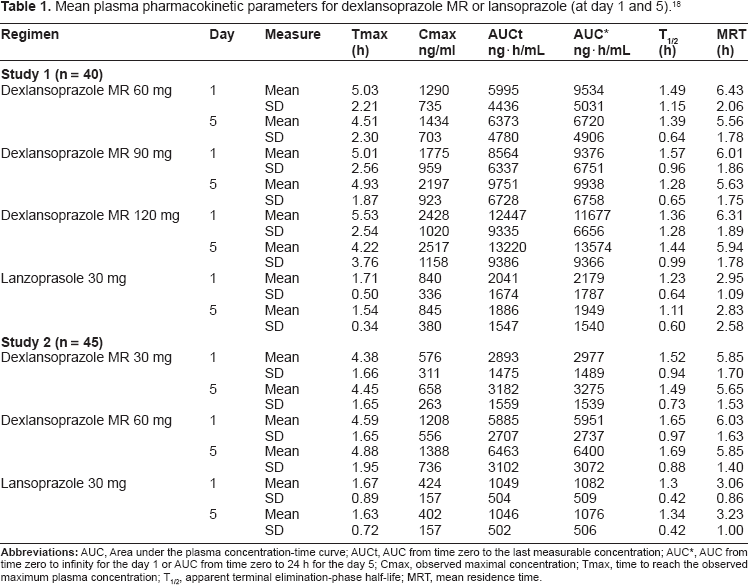
Two phase 1, randomized, open-label, multiple-dose, crossover studies have been conducted to evaluate the PK and PD of dexlansoprazole MR. 18 Healthy male and female subjects aged 18–55 years with a body mass index (BMI) ranging from 18 to 30 kg/m2 were eligible to participate. In study 1, subjects (n = 40 volunteers) received dexlansoprazole MR 60, 90, and 120 mg and lansoprazole 30 mg once daily for 5 days, in each of four periods according to the sequence to which they were randomly assigned. In study 2 (n = 45 volunteers), subjects received orally dexlansoprazole MR 30 mg and 60 mg and lansoprazole 15 mg once a day for 5 days in each of three periods according to the sequence to which they were randomly assigned. The doses used in the studies were those approved by the food and drugs administration in United States for various acid related disorders. In each study, dosing occurred at approximately 9 AM and participants were allowed to receive a breakfast one hour later, a lunch 4 hours later, a dinner 9 hours later and a snack 12 hours later. A washout of at least 5 days separated each treatment. The data of these two trials were pooled to assessed PK and PD parameters of dexlansoprazole MR and lansoprazole at day 1 and at steady-state (day 5). PD response was evaluated by the 24 hours continuous intragastric pH monitoring. The study's results showed that the plasma-concentration time profiles for dexlansoprazole at steady-state were characterized by two distinct peaks, the one occurring 1–2 hours after dosing and the second 4–5 hours after dosing. The Cmax and AUC of dexlansoprazole (30–120 mg once a day) increased in a dose proportional manner. At day 5, The AUC was approximately 3, 5 and 7 times higher with dexlansoprazole 60, 90 and 120 mg respectively, compared with lansoprazole 30 mg. Cmax was 1.5, 2.5 and 3 times higher with dexlansoprazole compared with lansoprazole 30 mg. Dual delayed release also prolongs the mean residence time (MRT: calculated as the average time the drug spend in the systemic circulation) of dexlansoprazole. MRT was approximately 3 h longer following administration of dexlansoprazole compared with that obtained after administration of lansoprazole. (Table 1)
Mean plasma pharmacokinetic parameters for dexlansoprazole MR or lansoprazole (at day 1 and 5). 18
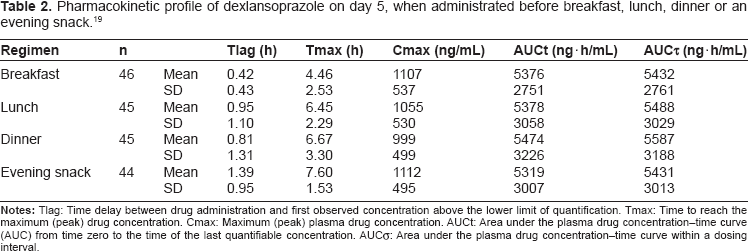
Lee et al 19 characterized the influence of time of the day on the steady-state pharmacokinetics of dexlansoprazole MR. A single dose, open-label, 4-ways crossover study was conducted in 48 healthy male and female volunteers, receiving dexlansoprazole MR 60 mg orally once daily for 5 days at one of the four different times of day: 30 min before i) breakfast (reference regimen), ii) lunch, iii) dinner or iv) an evening snack. The results of this study showed that absorption of dexlansoprazole was delayed approximately two-to threefold and, as a result, Tmax values occurred approximately 2–3 h later when dexlansoprazole MR was administered before lunch, dinner or an evening snack compared with administration before breakfast. However, there were no apparent differences in plasma mean dexlansoprazole Cmax or AUC values when dexlansoprazole MR was administered at different times of the day. Despite the delay in absorption, mean Cmax was 1055, 999 and 1112 ng/mL when dexlansoprazole MR was administered before lunch, dinner or an evening snack respectively compared with 1107 ng/mL after administration before breakfast; and AUC was 5378, 5474, and 5319 ng/h/mL when dexlansoprazole MR was administered before lunch, dinner or an evening snack, respectively, compared with 5376 ng/h/mL after administration before breakfast (Table 2). Moreover, Mean oral clearance was similar among regimens. These results indicating that bioavailability of Dexlansoprazole was not affected by the time of dosing in the day, before breakfast, lunch, dinner or an evening snack. Furthermore, the mean values of plasma half-life were similar with each regimen (1.27–1.44 h).
Pharmacokinetic profile of dexlansoprazole on day 5, when administrated before breakfast, lunch, dinner or an evening snack. 19
The pharmacokinetics of dexlansoprazole MR administered under fasting and various fed conditions (30 min before breakfast, or 5 or 30 min after breakfast) had been evaluated in an earlier phase 1, four-way crossover study in healthy subjects. 20 The values of AUC were 7999 and 6996 ng/h/mL when dexlansoprazole was administrated 30 min after a high fat breakfast or after a fasted state. Based on these results, it was concluded that dexlansoprazole MR can be administered without regard to meals or the timing of meals.
These results demonstrate that dexlansoprazole MR may offer a greater dosing flexibility for patients with acid-related disorders, which may improve compliance, an important and common issue for patients receiving PPI therapy for acid-related disorders.
Plasma protein binding of dexlansoprazole ranged from 96.1% to 98.8% in healthy subjects and was independent of concentration. The apparent volume of distribution after several doses in symptomatic GERD patients was 40.3 L. 21
Metabolism and excretion of [14C]TAK-390 have been evaluated by Grabowski et al 22 in six healthy male subjects. Subjects received a daily 60 mg nonradiolabeled TAK-390MR oral dose for 4 days, and a single oral dose of 60 mg [14C]TAK-390 suspension in aluminium hydroxide 200 mg/ magnesium hydroxide 200 mg/simethicone 20 mg, on day 5. Plasma, urine, and feces were collected for 7 days and analyzed for radioactivity and metabolite content. The results of this study showed that Dexlansoprazole is eliminated with a half-life of ~1–2 h in healthy subjects and in patients with symptomatic GERD. 50.7% of the initial dose was recovered in the urine and 47.6% in the feces. TAK-390 was metabolized by oxidation, reduction, and conjugation to at least 19 inactive metabolites. Oxidative metabolites are formed by the cytochrome P450 system, mainly through hydroxylation via CYP2C19 and oxidation via CYP3A4. The major and inactive metabolites characterized in plasma were 5-glucuronyloxy TAK-390 and 5-hydroxy TAK-390. Six metabolites of TAK-390 were characterized in urines accounting for an average of 85% of the urinary radioactivity. 5-glucuronyloxy TAK-390, 5-glucuronyloxy TAK-390 sulfide, 2-S-N-acetylcysteinyl benzimidazole, and 5-sulfonyloxy TAK-390 sulfide were the major metabolites. Six inactive metabolites were recovered in the feces. Apparent clearance (CL/F) in healthy subjects was 11.4–11.6 L/h, respectively, after 5 days of 30 or 60 mg/day administration.
Influence of CYP2C19 polymorphism on systemic dexlansoprazole exposure has been studied in Japanese male subjects. After volunteers received a single dose of dexlansoprazole MR 30 or 60 mg (n = 2–6 subjects/group), mean dexlansoprazole Cmax and AUC values were found to be to 2 times higher in intermediate compared to extensive metabolizers; in poor metabolizers, Cmax was approximately 4 times higher and mean AUC 12 times higher compared to extensive metabolizers. Despite no study was conducted in Caucasians and African Americans, dexlansoprazole exposure in these races may be affected by CYP2C19 phenotypes (Kapidex package insert, (Takeda Global Research and Development Center, Inc).
Necessity of dose adjustment in subjects with hepatic impairment has been studied by Lee et al 23 in a study where 12 patients with moderately impaired hepatic function received a single dose of dexlansoprazole MR 60 mg. Plasma exposure (AUC) of dexlansoprazole in the hepatic impairment group was 2 times greater compared to subjects with normal hepatic function. However, the authors did not consider the difference clinically relevant and did not suggest dose adjustment. This is in contradiction with the prescribing information for dexlansoprazole that recommends a maximum dose of 30 mg once daily for patients with moderate hepatic impairment. No study has been conducted in patients with severe hepatic impairment (Child-Pugh Class C).
Although the prescribing information for dexlansoprazole recommends no dose adjustment for patients with renal impairment, no study conducted in patients with renal failure has been identified in the literature.
In vitro data suggested that dexlansoprazole and lansoprazole have the potential to inhibit the activity of CYP3A and CYP2C19, and in the case of dexlansoprazole, the potential to induce human hepatic CYP1A. Vakily et al 15 studied the effects of dexlansoprazole on pharmacokinetics of diazepam, phenytoin, warfarin or theophylline in four separated randomized, double-blind, placebo-controlled, 2 ways crossover studies in healthy volunteers. Results of the four studies showed that concomitant administration of dexlansoprazole does not affect the elimination t1/2 and the AUC of the single dose coadministered drug and, therefore, it is unlikely that dexlansoprazole MR alters the pharmacokinetic profile of other drugs metabolized by CYP2C19, CYP2C9, CYP1A2 and perhaps CYP3A. Dose adjustments appear to be un-necessary in these cases of drug associations. However, further pharmacokinetic studies are needed to fully elucidate the effects of prolonged coadministration of dexlansoprazole with these or other medications.
The prescribing information for dexlansoprazole recommends against administration of dexlansoprazole with atazanavir, which absorption is pH dependent. Digoxin, iron salts, azole antifungals, and ampicillin esters also have pH-dependent absorption, but no pertinent study has been identified on the alteration of their pharmacokinetic by concomitant administration of dexlansoprazole.
Conflicting reports exist in the literature on the interactions of PPI and prodrugs activated by CYP2C19 or 2C9 dependent metabolism, like clopidogrel. 24 No literature data exist concerning the influence of dexlansoprazole on this metabolic prodrug activation. At this time, the prescribing information for clopidogrel recommends avoiding the combination of clopidogrel and agents that inhibit CYP2C19, unless clinically necessary. Additionally a new safety issue has been recently reported suggesting that in aspirin treated patients with first time myocardial infarction, treatment with proton pump inhibitors could be associated with an increased risk of adverse cardiovascular events. 25
Pharmacodynamic Profile
Dexlansoprazole MR was compared with two doses of lansoprazole, 15 mg and 30 mg once daily dosing in two studies reported by Vakily et al. 18 In the first study, the 24-h mean pH was statistically significantly higher after 5 days of dexlansoprazole DR 60, 90 or 120 mg dosing than that after 5 days of lansoprazole 30 mg dosing (P < 0.01). In study 2, dexlansoprazole MR 30 and 60 mg provided superior control of the intragastric pH compared with that obtained for lansoprazole 15 mg. The 24-h mean pH was statistically significantly higher after 5 days of dexlansoprazole MR 30 or 60 mg dosing than that after 5 days of lansoprazole 15 mg dosing (P < 0.01). Nevertheless, despite the modified released formulation the curves for mean pH exhibited the same patterns.
Lee et al 19 characterized the influence of time in the day of the dosing on the efficacy of dexlansoprazole MR. In a single dose, open-label, 4-ways crossover study, healthy volunteers received dexlansoprazole MR 60 mg orally once daily for 5 days at one of the four different times of day: 30 min before i) breakfast (reference regimen), ii) lunch, iii) dinner or iv) an evening snack. Continuous monitoring of intragastric pH performed in this study showed that the mean percentage of time with intragastric pH > 4 during the 24-h postdose interval on day 5 was 71%, 74%, 70% and 64% for the breakfast, lunch, dinner and snack regimens respectively. The difference between snack regimen and breakfast regimen was statistically significant (P < 0.05). Moreover, the mean intragastric pH during the 24-h period after administration of dexlansoprazole MR before lunch was higher than when the drug was administered before breakfast (4.83 vs. 4.63, respectively, P < 0.05). However, these differences were very small and not considered clinically meaningful. These results suggest that dexlansoprazole MR could be taken at any time during the day.
Clinical Studies
There are two steps in treating patients suffering from GERD, the first one being to heal the esophagitis and the second one to prevent recurrence and prevent symptoms.
Healing phase
The efficacy and safety profile of dexlansoprazole MR was assessed in two identical double-blind randomized controlled trials including a total of 4092 patients with erosive esophagitis (EO) who received either 60 mg or 90 mg of dexlansoprazole or 30 mg of lansoprazole once daily. 26 This study was aimed to assess week 8 healing and was designed as a non-inferiority trial followed by a second test for superiority versus lansoprazole.
Using life table analyzes dexlansoprazole healed 92% to 95% of patients in individual studies versus 86% to 92% for lansoprazole. The differences were not statistically different (P > 0.025). Dexlansoprazole was thus found to be non inferior, but not superior to lansoprazole. 26
For the more conservative crude rate analysis, both dexlansoprazole MR 60 mg (P = 0.004) and 90 mg (P = 0.001) provided significantly higher healing rates at week 8 than lansoprazole 30 mg in the first study, with therapeutic gains (difference in healing rates) of 6 and 7 percentage points respectively.
Dexlansoprazole MR 90 mg, but not 60 mg, also provided significant higher crude healing rate at week 8 than lansoprazole 30 mg in the second study with a therapeutic gain of 5 percentage points. In the first of the two studies, dexlansoprazole was shown to confer some kind of benefits over lansoprazole for the more severe patients ie, those with a Los Angeles grade C or D esophagitis (about 30% of patients in each treatment group), but this benefit was not observed in the second study. It is of interest that crude rate for healing at week 8 in the lansoprazole group in study 2 was exactly the same as that of dexlansoprazole MR 90 mg group in study 1 (84.6% and 85.8% for lansoprazole 30 mg and dexlansoprazole MR 90 mg respectively), questioning robustness of the statistical difference within groups in both studies.
The proportion of patients with at least one treatment-emergent adverse event was similar among all three treatment groups in the combined studies: 30.4%, 28.1%, and 27.8% in the dexlansoprazole MR 60 mg, 90 mg and lansoprazole 30 mg treatment groups respectively. The most common adverse event leading to premature discontinuation in dexlansoprazole MR and lansoprazole patients was diarrhea (0.5% and 0.2% respectively).
Maintenance phase
One study conducted by Howden and colleagues. 27 included 451 patients, with erosive esophagitis healed in either one of two dexlansoprazole MR healing trials, 26 in a double-blind trial. Patients were excluded from the healing trials if they were positive for Helicobacter pylori by serological assay, and were, therefore, ineligible for this maintenance trial. Patients were randomized to receive either dexlansoprazole MR 60 mg or 90 mg or placebo once daily. Endoscopy was performed at months 1, 3, and 6 or at the final visit to document the presence or absence of EO. Main outcome was the proportion of patients maintaining healing at months six and was analyzed using life table and crude rate methods. Secondary endpoints were percentages of nights and 24-hours day without heartburn based on daily diaries.
In this study the two doses of dexlansoprazole MR (60 mg and 90 mg) were both found to be superior to placebo for maintaining healing. Maintenance rates were 87% and 82% for the 60 and 90 mg doses, respectively whereas it was only 26% for placebo (life tables), and 60% and 65% versus 14% respectively (crude rate).
Both doses were found to be superior to placebo for the percentage of 24-hours heartburn-free days (60 mg, 96%; 90 mg 94%; placebo 19%) and nights (98%, 97%, and 50% respectively), but no difference was observed between both dexlansoprazole MR doses.
Adverse events like diarrhea, gastritis and abdominal pain occurred more frequently with dexlansoprazole MR than with placebo. This study demonstrates that dexlansoprazole MR is effective at maintaining healed erosive esophagitis and symptom relief but one of its major pitfalls is that the drug was compared to placebo and not to another PPI.
Another study published the same year by Metz and colleagues. 28 assessed in a randomized double-blind placebo-controlled trial the efficacy of dexlansoprazole MR 30 mg or 60 mg in maintaining healing of erosive esophagitis. In this study 445 patients with healed erosive esophagitis were randomized to receive either dexlansoprazole MR 30 mg or 60 mg per day or placebo. Maintenance rate where 75%, 83% and 27% respectively. Crude maintenance rates where 66% for both dexlansoprazole MR doses and 14% for placebo.
A prospective, randomized, double-blind, placebo-controlled, parallel-group study published in 2011 evaluated the efficacy of dexlansoprazole MR 30 mg in relieving nocturnal heartburn and GERD-related sleep disturbances, improving work productivity, and decreasing nocturnal symptom severity in patients with symptomatic GERD. 29 In this study 305 patients with frequent, moderate-to-very severe nocturnal heartburn and associated sleep disturbances were randomized 1:1 in a double-blind fashion to receive dexlansoprazole MR 30 mg or placebo once daily for 4 weeks. Patients with erosive esophagitis were to be excluded. The primary efficacy endpoint of the percentage of nights free of heartburn, as assessed by daily diary, was significantly greater in patients receiving dexlansoprazole MR 30 mg daily than in those receiving placebo (median of 73.1% vs. 35.7%; P < 0.001), even after adjusting for a wide range of potentially confounding factors. Therapeutic gain was maximal for patients with the most severe symptoms.
It is of concern that both studies were placebo and not active treatment controlled, and that they do not define the most appropriate dose to be used.
Safety
The safety profile of dexlansoprazole was reviewed in the paper that combined data from six randomized controlled trial and a 12-months safety study. 30 These studies included 4270 patients who received dexlansoprazole MR 30 mg (n = 455), 60 mg (n = 2311) or 90 mg (n = 1864); lansoprazole 30 mg (n = 1363) or placebo (n = 896). In these clinical trials safety was assessed as adverse events, vital signs, electrocardiograms, clinical laboratory results and gastric biopsies. Adverse events were summarized per 100 patient-months of exposure to account for imbalances in study drug exposure.
The number of patients with more than one treatment emergent adverse event per hundreds patient months was higher in placebo (24.5) and lansoprazole (21.1) than in any dexlansoprazole MR (15.6–18.8) group. From this paper it cannot be concluded that placebo had worst safety profile than dexlansoprazole or lansoprazole as most of the adverse events, that were found to be significantly more frequent in the placebo group, only reflect the absence of efficacy. But it's likely to conclude that dexlansoprazole MR and lansoprazole share the same safety profile. No specific signal was captured in terms of clinical laboratory values, EKG and gastric biopsies. As expected mean serum gastrin levels increased in all PPI dose-groups and were significantly higher than in the placebo group. Interestingly whereas gastrin levels increased during the first 3 months of receiving dexlansoprazole MR, it generally stabilized for the rest of study duration. Serum gastrin levels of patients who were randomized to placebo, in maintenance study, returned to baseline within the first month of the study regardless of which treatment they had received for the healing phase.
In the most recently published clinical trial that included 305 patients for a 4-weeks course of dexlansoprazole 30 mg MR, rates of AEs were similar among groups, the most frequently reported AE being upper respiratory tract infection, reported by 5% and 2% of the patients in the dexlansoprazole and placebo groups respectively.
Overall clinical trials that have been so far conducted with dexlansoprazole MR suggested that the safety profile is similar to that of all other PPIs already on the market.
Patient Preference
It is not possible to assess patient preference as published studies were only placebo-controlled trials. New head-to-head comparison, or real-life setting studies, will only allow for patient preference assessment.
Place in Therapy
It is quite difficult to best define Dexlansoprazole MR place in therapy as most of the studies were conducted versus placebo, and not versus an active comparator. Additionally when dexlansoprazole was compared with lansoprazole, daily dose was not the same. Indeed as dexlansoprazole MR is the R-isomer, the active one, of lansoprazole, studies have somehow assessed the efficacy of 60, 120 or 180 mg of lansoprazole compared either to placebo or 30 mg of lansoprazole. Thus available clinical results do not permit to rank usefulness of dexlansoprazole MR versus other PPI. It has to be kept in mind that none of the other PPIs available has clearly been shown to confer any advantage compared to the others. There is a theoretical advantage conferred by the modified release formulation, nevertheless it has not been yet convincingly converted into a clinical benefit for the patient. It is at least doubtful that the company marketing dexlansoprazole MR will engage in a complicated and costly development plan aimed at demonstrating superiority over the other PPIs.
The cost of a drug is of concern either for the patient or for a third party covering for drug fees. It is uneasy to discuss the cost of the drug as it might differ between countries where it has been, or will be released. But based on what has been shown in clinical studies authors’ opinion is that there is no incremental efficacy of dexlansoprazole MR likely to justify a price higher to that of lansoprazole generics.
The PK/PD properties, although being of theoretical interest, have not been converted into clinical benefit. There is no formal reason to explain this discrepancy between a more favorable PK/PD and a comparable efficacy profile compared with lansoprazole, but it has also been observed with potassium-competitive acid blockers that appeared very promising during phase one study and did not pass phase 2 studies. But, as all the existing PPIs have similar mechanisms of action, significant improvements in the current treatment profile may prove difficult to achieve, particularly with regard to onset of effect and duration of action. Additionally acid secretion might not be the only component of acid related disorders, explaining why improving acid control might not necessarily turns into improvement of clinical symptoms. Transient lower esophageal sphincter relaxations (TLESRs)–-frequent spontaneous relaxations of the LES–-are an important mechanism underlying GERD. 31
A new field of research has emerged aimed at developing effective drugs to reduce TLESRs, and it can be assumed that optimal control of GERD might only be achieved by a combination of drugs targeting the different component of the disease.
Conclusions
Dexlansoprazole MR appears to be well tolerated and effective in the healing of erosive esophagitis.
Nevertheless as most of the data were obtained from placebo-controlled trials it is not possible to draw definite conclusions about the place of dexlansoprazole among PPIs. It will remain the case until new head-to-head comparative studies will be conducted to determine whether the original formulation of dexlansoprazole translates into clinically meaningful benefits.
Authors’ opinion is that at this stage, dexlansoprazole 30 mg MR has not shown any added value compared to lansoprazole and must thus be considered as one additional PPI.
Disclosure
This manuscript has been read and approved by all authors. This paper is unique and is not under consideration by any other publication and has not been published elsewhere. The authors and peerre viewers of this paper report no conflicts of interest. The authors confirm that they have permission to reproduce any copyrighted material.