
Abstract
Erectile dysfunction (ED) is a condition that affects approximately 18 million American men. Phosphodiesterase-5 inhibitors (PDE5i's) have revolutionized the treatment of erectile dysfunction by providing the first highly-effective oral medication. Vardenafil is one of 3 PDE5i's commercially available for the treatment of ED in the United States. It has demonstrated therapeutic efficacy in the management of uncomplicated ED as well as more refractory cases associated with diabetes and surgery for prostate cancer. The physiology, pharmacokinetics, pharmacodynamics, and primary literature evaluating vardenafil are reviewed.
Introduction
Erectile dysfunction (ED) is a condition that affects approximately 18 million American men. 1 The incidence appears to be increasing, although this is likely related to increased public awareness and self-reporting. The increased awareness that has taken place over the last decade is due in no small part to the discovery of the therapeutic efficacy of phosphodiesterase-5 inhibitors (PDE5i's) in treating ED as well as the marketing campaigns of the 3 formulations that are commercially-available in the United States. PDE5i's have revolutionized the treatment of erectile dysfunction. Whereas ED was traditionally a condition managed by specialists, the introduction of PDE5i's has resulted in management of ED in the primary care setting. PDE5i's provide arguably the most physiologic erection of the available treatments for ED. PDE5i's have traditionally been prescribed and studied as on-demand medications for the treatment of ED. However, with the recent exploration of once daily maintenance therapy as well as post-radical prostatectomy penile rehabilitation, there is potential for new ways to apply these medications to the management of ED.
Physiology of Penile Erection
In the flaccid state, there is very little blood flow to the corpora cavernosa. The hemodynamics of the penis in this setting are the result of baseline sympathetic tone. This sympathetic input maintains vasoconstriction of the cavernosal arteries as well as contraction of the cavernosal smooth muscles surrounding the lacunar spaces. The flaccid penis is smaller in this state, because this sympathetic tone minimizes cavernosal arterial inflow, corporal cavernosal volume, and ability of the corpora to trap blood. The small amount of blood that enters the corpora cavernosa exits through venules that pierce the tunica albuginea of the penile shaft. This blood then drains through the venous systems of the penis.
The physiologic process of penile erection involves both cavernosal filling and trapping of blood. Upon sexual stimulation, cholinergic end neurons of the parasympathetic neurons arising from spinal segments S2-4 produce acetylcholine which acts through the inositol triphosphate pathway to increase the conversion of l-arginine to nitric oxide (NO) by endothelial nitric oxide synthase (eNOS). This results in arteriolar dilation and increased cavernosal blood flow. Simultaneously, the nitrergic end neurons of parasympathetic nerves S2-4 located in the cavernosal tissue release NO. NO is produced by the cleavage of l-arginine by neuronal nitric oxide synthase (nNOS). Production of NO results in the conversion of GTP to cGMP by guanylate cyclase. cGMP interacts with protein Kinase G resulting in calcium shifts into the sarcoplasmic reticulum and relaxation of the carvernosal smooth muscles. The result of these processes is a 20 to 40-fold increase in cavernosal blood flow. The penis then enlarges in both length and girth until the tunica albuginea surrounding the corpora cavernosa reaches its maximum capacity for stretch. Once this occurs, the intracavernosal pressure increases. This increase in intracavernosal pressure compresses the venules against the underside of the tunica albuginea, preventing venous outflow of intracavernosal blood and providing the mechanism by which blood is trapped in the corpora cavernosa of the erect penis.
Mechanism of Phosphodiesterase-5 Inhibitors
Phospodiesterases (PDEs) are intracellular enzymes that regulate breakdown of cyclic nucleotides. 2 PDE5 is one of eleven mammalian PDE families. Inhibition of PDE5 prevents the breakdown of cGMP, which promotes calcium sequestration into the sarcoplasmic reticulum of cavernosal smooth muscle cells. This results in potentiated smooth muscle relaxation and cavernosal engorgement (Fig. 2). 3
Chemical structure of vardenafil.
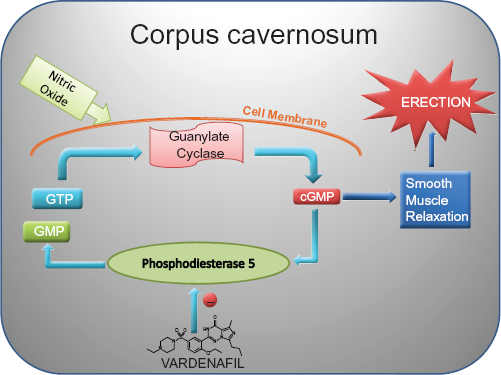
Mechanism of vardenafil.
Vardenafil (Levitra®) was the second PDE5i to receive FDA approval for the treatment of ED in the United States (Fig. 1). Vardenafil is the most potent of the commercially-available PDE5i's, although this has not been demonstrated to result in a clinical advantage over other PDE5i's. The IC50 is the in vitro concentratration at which 50% of phosphodiesterase 5 is inhibited. The IC50 for vardenfil is 0.1 to 0.7 nM. The IC50 of sildenafil is 3.9 nM. 4 The IC50 of tadalafil is 0.94 nM. 5 The maximal plasma concentration (Cmax) for vardenafil 20 mg 20.9 ng/ml vs. 327 and 378 ng/ml for sildenafil 100 mg and tadalafil 20 mg, respectively. The time to reach Cmax for vardenafil is similar to sildenafil at 0.7 to 0.9 hours and considerably shorter than that of tadalafil (2 hours). The half life of vardenafil is similar to sildenadfil at 4 to 5 hours, but shorter than the half life of tadalafil, which is 17.5 hours.5,6 As with sildenfail, consumptions of a high fat meal prior to taking vardenafil prolongs the time to reach Cmax. Unlike sildenafil, consumption of a high-fat meal does not alter is relative bioavailability. The delay in reaching Cmax has not been observed in low to moderate fat meals. 7 Tadalafil's absorption and bioavailability does not appear to be altered by high-fat meals. 8
With regard to selectivity, the affinity of vardenafil for PDE5 versus PDE6 is >15:1. This is higher than that of sildenafil (10:1) but lower than that of tadalafil (.700:1). Crossreactivity with PDE6 is responsible for the blurred vision that some patients may experience when taking PDE5i's. Indeed, comparative evaluation of side effects by patients taking once of the 3 PDE5i's has demonstrated increased blurred vision in patients taking sildenafil versus the other two PDE5i's. 9 Vardenafil's affinity for PDE5 vs. PDE11 is >300:1, which is less than that of Sildenafil (.700:1), but more than that of tadalafil (20 to 40:1). This may explain why there is a higher incidence of musculoskeletal pain in patients taking tadalafil. 9
Clinical Efficacy of Vardenafil
In 2001, Klotz et al performed a pharmacokinetic and pharmacodynamic study of vardenafil in 21 men with ED. The study was a prospective randomized, double-blind, placebo-controlled crossover trial. Outcomes were measured with a RigiScan. A Rigiscan is a device that consists of two cuffs worn at the base and tip of the penis. These cuffs measure radial penile rigidity at these two locations. This is then expressed as percentage of total rigidity (100%). The subjects in this trial wore the device 0.5 hour prior to dosing and then 2.5 hours after dosing. The subjects watched sexually explicit videos and RigiScan measurements were taken. The primary endpoint of the study was the length of time that penile rigidity was >60%. Vardenafil was evaluated at single doses of 10 and 20 mg. Compared to placebo, subjects receiving 10 mg demonstrated an increase in duration of >60% rigidity of 24.4 and 24.8 minutes at the base and tip of the penis, respectively. Subjects receiving 20 mg vardenafil demonstrated an increase in duration of 37.2 and 28.7 minutes at the base and tip, respectively. With regard to pharmacokinetics, vardenadil demonstrated a Tmax (time from administration to maximal plasma concentration) of 0.7 to 0.9 hours and a serum half life of 4.2 hours. 10 This study confirmed the therapeutic efficacy and specific pharmacokinetics of vardenafil.
Porst et al performed the first at home evaluation of vardenafil in 601 men. This was a multicenter, randomized, double-blind, placebo-controlled trial evaluating vardenafil at 5, 10, and 20 mg doses over a 12-week treatment period. Primary endpoints were answers to questions 3 (When you attempted intercourse, how often were you able to penetrate your partner?) and 4 (During intercourse, how often were you able to maintain your erection after you entered your partner?) of the International Index of Erectile Function (IIEF). The IIEF is a validated 15-item questionnaire designed to measure the degree of erectile dysfunction. Each question is answered on a 0–5 scale, with a score 5 indicating better function. All three doses of vardenafil demonstrated a statistically significant increase in positive responses to questions 3 and 4. Additionally, patients receiving vardenafil demonstrated statistically significant increases in all domain scores of the IIEF. Eighty percent of men receiving the 20 mg dose responded positively to the global assessment question (Has the treatment you have been taking for the last 4 weeks improved your erections?) compared to 30% for men receiving placebo. Treatment-emergent adverse events were dose-related and included headache (7%–15%), flushing (10%–11%), dyspepsia (1%–7%), and rhinitis (3%–7%). 11 This was the first study to report the efficacy of vardenafil in enabling men with ED to engage in successful sexual intercourse as determined utilizing a validated instrument.
In 2003, Hellstrom et al published a phase III, multi-center, randomized, double-blind, placebo-controlled, four-arm, parallel-group, fixed dose comparison study. Eight hundred and five patients were treated with of vardenafil 5 mg, 10 mg, 20 mg, or placebo for 26 weeks. Efficacy was determined through utilization of several metrics. Subjects were asked to answer IIEF questions 1–5 and 15 (IIEF-ED) after 12 weeks of treatment. They were also asked to answer the sexual encounter profile question 2 (SEP2) “Were you able to insert your penis into your partner's vagina?” as well as the sexual encounter profile question 3 (SEP3) “Did your erection last long enough for you to have successful intercourse?” Secondary outcomes included answers to the above questions at 26 weeks as well as a global assessment question. All vardenafil treatment arms demonstrated statistically significant improvements in primary outcomes. Mean EF domain score improved from 12.5 to 18.4, from 13.4 to 20.6, and from 12.8 to 21.4 from baseline to 12 week follow-up for vardenafil 5, 10, and 20 mg treatment groups, respectively (P < 0.0001 vs. placebo). The placebo arm did not demonstrate a significant change in EF domain score over the study period. The mean successful penetration rate improved from 42.8 to 65.5%, 45.4 to 75.5%, and 40.9 to 80.5% from baseline to 12 week follow-up in the vardenafil 5, 10, and 20 mg treatment groups (P < 0.0001 vs. placebo). The mean ability to maintain an erection for successful intercourse improved from 14.0 to 50.6%, 14.6 to 64.5%, and 14.7 to 64.5% in the vardenafil 5, 10, and 20 mg treatment groups, respectively (P < 0.0001). These statistically significant improvements were maintained at 26 week follow-up. 12 This study confirmed vardenafil's efficacy and safety in treating ED.
Erectile Dysfunction and Comorbid Conditions
The presence of ED has been suggested to be associated with an increased risk of future cardiac events. In two large scale analyses, the presence of ED was found to be a harbinger for future cardiac events.13,14 This is thought to be due to the common vascular pathology contributing to these two conditions. This has led to the investigation of the effect of cardiovascular risk factors, comorbid conditions, medications, and their relationship to the management of ED with PDE5i's.
ED develops in greater than 50% of patients within 10 years of being diagnosed with diabetes. In the Massachusetts Male Aging Study, the age-adjusted probability of developing ED was three times high in patients with diabetes compared to those without this condition. 15 In diabetic patients, ED is often associated with peripheral vascular disease and diabetic neuropathy.16,17 Reported success rates of PDE5i's in treating ED in diabetic patients have been lower than those reported evaluating their use in the general population. 18 Goldstein et al examined the efficacy of vardenafil in treating ED in diabetic patients in a phase III multi-center prospective randomized double-blind placebo-controlled trial published in 2003. In this trial 452 diabetic males were randomized to receive placebo, vardenafil 10 mg, or vardenafil 20 mg for 12 weeks. Primary outcomes were improvement in the IIEF-EF and answers to SEP2 and SEP3 questions. The mean improvement in the IIEF erectile function domain was 5.9 and 7.8 for vardenafil 10 and 20 mg (P = 0.03), respectively compared to 1.4 for placebo (P < 0.0001). The percentage of subjects self-reporting successful vaginal penetration was 36, 61, and 64% for placebo, vardenafil 10 mg, and 20 mg respectively (P < 0.0001 vs. placebo). The self-reported ability to maintain an erection until the end of intercourse was 23, 49, and 54% in the placebo, vardenafil 10 mg, and 20 mg groups, respectively (P < 0.0001). 19 This was the first study demonstrating the efficacy of vardenafil in treating diabetic males.
Subsequent studies have confirmed vardenafil's efficacy in treating ED in diabetic patients with success rates similar to those reported for sildenafil in treating this patient population.20,21 In 2006, Ziegler et al evaluated the efficacy of vardenafil in treating ED in men with type 1 diabetes mellitus. In this multicenter, double-blind, placebo-controlled trial, 302 PDE5i-naïve men were randomized to receive placebo or flexible dose vardenafil. Primary outcomes were answers to SEP2 and SEP3. Secondary outcomes were IIEF scores. Patients receiving vardenafil demonstrated significant improvements in SEP2 and SEP3 regardless of level of glycemic control (P < 0.0001). 20 The percentage of men responding positively to SEP2 and SEP3 was 71 and 50% after 12 weeks of treatment. These numbers are similar to that reported by Goldstein et al in their study on the use of vardenafil in diabetic patients, 19 but lower than those reported in the general population of men with ED. This seems to indicate that diabetic patients tend to have more refractory ED than patients without diabetes, but that this may not be a function of level of glycemic control.
The efficacy of vardenafil in the treatment of men with dyslipidemia was demonstrated by Miner et al in 2008. 22 In this multicenter, randomized, double-blind, placebo-controlled study of 712 men who had been on statin therapy for at least 3 months were given flexible dose vardenafil or placebo. Significant improvements in IIEF-EF, SEP2, and SEP3 were demonstrated. In a follow-up randomized, double-blind placebo- controlled, parallel group study, the same investigators evaluated the relationship between severity of dysplipidemia and efficacy of flexible dose vardenafil. Once again, outcomes included IIEF-EF, SEP2, and SEP3. In addition, a stopwatch-assessed duration of erection was performed. Subgroup analysis was performed based low density lipoprotein cholesterol (LDL-C) levels, total cholesterol to high density lipoprotein cholesterol ratio (TC/HDL-C), and the presence or absence of the metabolic syndrome. Once again, vardenafil treatment was associated with a significant improvement in all outcome measures regardless of subgrouping. Interestingly, patients with higher LDL-C experienced a greater increase in IIEF-EF despite similar baseline scores (P = 0.033). However, neither TC/HDL-C nor the presence of metabolic syndrome were associated with significant changes in IIEF-EF scores. Response to SEP2 did not differ significantly between subgroups. Response to SEP3 followed a similar pattern to the IIEF-EF score, with high LDL-C being associated with a significantly increased positive response rate (P = 0.019). The mean duration of erection sufficient for penetration was significantly longer in the patients of a TC/HDL-C greater than or equal to 3.5 (P = 0.028). 23 While the findings of this study fail to demonstrate a clear pattern of therapeutic efficacy among subgroups, all significant associations seem to be paradoxical. This may be explained by the fact that all patients in this study were on stable statin therapy. Thus, the lipoprotein levels used to stratify patients do not necessarily reflect baseline severity of dyslipidemia. Additionally, given the flexible-dose study design, patients with more severe dyslipidemia may have been receiving higher doses of vardenafil. Furthermore, no information was available regarding comorbid medical conditions as well as concomitant medications, all of which can have significant effects on erectile and sexual function.
Eardley et al performed a retrospective analysis of 13 randomized, double-blind, placebo-controlled trials investigating the use of vardenafil in patients with diabetes mellitus, hypertension, dyslipidemia, and/or the metabolic syndrome. Outcome measures were change in IIEF-EF score and answers to SEP2 and SEP3 questions. The investigators found significant improvement in all outcome measures regardless of underlying medical condition(s). Interestingly, the authors found that the level of glycemic control as well concomitant use of medications for the treatment of diabetes mellitus, hypertension, and dyslipidemia had no significant effect on efficacy of vardenafil. 24 Antihypertensive medications in particular have been demonstrated to adversely affect erectile function. 25 Given that sexual side effects can have a negative effect on patient compliance with these medications, the ability to minimize these effects can improve compliance and potentially prevent untoward cardiac events. Indeed, McLaughlin et al has demonstrated that prescribing sildenafil can improve patient compliance with antihypertensives, oral hypoglycemics, and antidepressants. 26
Sexual dysfunction, to include ED, is known to occur with significant frequency in patients with schizophrenia. 27 Whether ED in these patients is a consequence of symptoms of schizophrenia or antipsychotic medications is unclear. 28 In 2006, Gopalakrishnan et al performed a randomized, double-blind, placebo-controlled trial that demonstrated sildenafil to significantly improve erectile function in men with antipsychotic-induced ED. 29 Mitsonis et al performed a 12-week, open-label study of the efficacy of flexible-dose vardenafil in the treatment of ED in patients with schizophrenia. The IIEF was used to measure sexual function outcomes. A schizophrenia-specific Quality of Life Scale (QLS) 30 was administered to evaluate the effect of vardenafil on the patients’ overall quality of life. Vardenafil resulted in a statistically significant improvement in all IIEF domains as well as in the QLS when compared to baseline. 31 The strength of these results is weakened by the study's small size and lack of a control group. However, the significant improvement in overall quality of life as well as in all domains of the IIEF experienced by patients after being treated with vardenafil highlights the profound effect that PDE5i's can have on patients suffering from schizophrenia. Further large scale placebo-controlled studies are needed to confirm these findings.
Erectile dysfunction and lower urinary tract symptoms related to benign prostatic enlargement are both conditions that commonly affect the aging male patient. Concomittant management of these conditions has raised concern as PDE5i's and α-blockers can both result in hypotension. Simultaneous administration of vardenafil and α-blockers to healthy volunteers resulted in clinically significant decreases in blood pressure. Thus, the simultaneous use of alpha blockers and vardenafil was initially contraindicated. 32 Subsequent studies demonstrated that this effect was mitigated by separating the dosing of these two medications by at least 6 hours. Additionally, the use of the α1a receptor blocker tamsulosin further reduced the incidence of hypotension. 33 Thus, the contraindication on simultaneous administration was lifted by the FDA. It is now recommended that patients should be stable on α-blocker therapy before being started on the lowest vardenafil dose that is clinically effective. 34
Comparative Studies
In a prospective, randomized, double-blind, crossover study performed in 2006, investigators compared vardenafil and sildenafil in treating patients with diabetes mellitus, hypertension, and/or hyperlipidemia. A total of 931 men were included in the intent to treat population. The two drugs were assessed for patient preference, efficacy, and adverse events. With regard to preference, 683 (73.4%) of patients responded to the question. Vardenafil was preferred by 38.9% of patients, sildenafil by 34.5% of patients, and 26.6% of patients had no preference. This difference was not statistically significant. The IIEF-EF, SEP2, SEP3, and GAQ were used to evaluate efficacy, and responses to the treatment satisfaction scale (TSS). Vardenafil demonstrated statistical superiority in the included IIEF-EF, SEP2, SEP3, GAQ, and 12 of 19 TSS items. No significant differences were noted for the remaining 7 TSS items. Incidence of adverse events was low and similar between vardenadil and sildenafil. This was the first study to suggest that vardenafil may have increased therapeutic efficacy when compared to sildenafil. However, it should be noted that nominal significance does not necessarily translate into clinical significance. Indeed, no statistical difference in patient preference was demonstrated. 35 Further similarly-designed studies will be necessary in order to compare the efficacy of all 3 PDE5i's. Additionally, subgroup analysis with regard to medical comorbidities may help to identify specific therapeutic niches for each medication.
In 2009 Jannini et al reported on an open-label, randomized, multicenter crossover study comparing sildenafil 50 mg, sildenafil 100 mg, tadalafil 20 mg, and vardenafil 20 mg in the treatment of ED. 36 Of note, data from the crossover portion of this study were not presented in this publication. These data will likely be published in subsequent manuscripts. One hundred thirty-four men were randomized to one of the four study arms. Primary outcome was efficacy as determined by IIEF-ED scores after 8 weeks of treatment. Secondary outcomes were penile hemodynamic parameters as determined by penile duplex after intracavernosal injection of alprostadil. Of note, hemodynamic studies were not performed during the therapeutic window for the assigned PDE5i. No significant differences in primary outcomes were demonstrated between any of the 4 study groups. Sildenafil 50 and 100 mg were both associated with improvements in cavernosal peak systolic velocity when compared to baseline. Only patients receiving sildenafil 100 mg demonstrated a significant improvement in resistive index when compared to baseline. The clinical implications of these hemodynamic findings are not clear. Additionally, the findings of this study are weakned by the open label nature and a high attrition rate (25%).
Vardenafil in the Treatment of Postprostatectomy Erectile Dysfunction
ED can occur in over one third of patients undergoing radical prostatectomy for the treatment of prostate cancer. The cavernosal nerves course posterolateral to the prostate bilaterally before piercing the pelvic diaphragm and entering the corpora cavernosa. These nerves are responsible for releasing NO in response to sexual arousal leading to cavernosal engorgement as described above. The cavernosal nerves are vulnerable to injury during the posterolateral dissection performed during radical prostatectomy. Nerve-sparing techniques utilized in open, laparoscopic, and robotic-assisted prostatectomies are aimed at minimizing permanent ED. However, even patients who go on to experience a full recovery of erectile function tend to experience a variable period of severe ED following surgery. In these cases, the etiology of this transient ED is thought to be related to surgery-induced neuropraxia rather than complete transection.
In 2003, Brock et al published the first study examining the efficacy of vardenafil in treating postprostatectomy ED. This was a randomized, placebo-controlled, double-blind, fixed-dose, parallel group study examining the efficacy of vardenafil in restoring erectile function in men with postprostatectomy ED having undergone either bilateral or unilateral nerve-sparing radical retropubic prostatectomy. Efficacy was assessed using a GAQ. 65.2, 59.4, and 12.5% of patients receiving vardenafil 20 mg, 10 mg, and placebo reported improvement in erections, respectively. The strongest predictor of therapeutic efficacy was pretreatment ED rather than whether nerve sparing was unilateral or bilateral. 37 While this study clearly demonstrates improved erections in the patients having received vardenafil, findings are weakened by the lack of a validated instrument for assessing erectile function.
In recent years, several investigators have evaluated the role for penile rehabilitation in the treatment of postprostatectomy ED. This practice of penile rehabilitation is based on muscular rehabilitation programs that have proven beneficial in treating striated muscle denervation injuries. The regular oxygenation of the corpora cavernosa that occurs during sexual arousal as well as during nocturnal penile tumescence (NPT) may serve to maintain healthy corporal tissue. Corporeal oxygen tension has been demonstrated to increase from 25–40 mmHg in the flaccid state to 90–100 mmHg during erection. 38 This oxygen may be necessary for the efficient synthesis of NO. Furthermore, the results of several animal models have demonstrated that prolonged lack of cavernosal engorgement with its associated relative hypoxia may be associated with elevated levels of TGF-β resulting in corporeal fibrosis. 39 Thus, in theory, early intervention may prevent cavernosal smooth muscle atrophy and apoptosis as well as corporal fibrosis. This is thought to lead to a corporal veno-occlusive disorder (CVOD) where cavernosal arterial inflow is intact, but the emissary veins are never completely compressed against the tunica of the corpora cavernosa resulting in continuous venous leak.
Montorsi et al described the first prospective, randomized trial evaluating the therapeutic efficacy of restoring erections in the early postprostatectomy period. In this study 30 men having undergone nerve-sparing radical retropubic prostatectomy were randomized to receive intracavernosal alprostadil three times a week for twelve weeks or to be observed over the same time period. Patients were then evaluated six months after surgery with a detailed sexual history, penile Doppler examination, and RigiScan. Twelve of the 15 (80%) patients in the treatment arm completed the study. Of these patients, 8 of 12 (67%) reported recovery of spontaneous erections sufficient for vaginal penetration compared to 2 of 15 (20%) in the control arm (P < 0.01). Ten of the 12 (83%) patients in the treatment group, including all complete responders and 2 partial responders, had normal penile hemodynamics, while 2 of the partial responders demonstrated CVOD on Doppler examination. Within the control group, all 3 men with recovery of spontaneous erections and 2 of the failures demonstrated normal penile hemodynamics. However, 8 (67%) of the failures in this group demonstrated CVOD and 2 demonstrated arterial insufficiency. Thus, there was a 33% incidence of normal penile hemodynamics, a 14% incidence of arterial insufficiency, and a 53% incidence of CVOD in the control group. This study demonstrated both clinical and radiologic evidence of a potential benefit of early restoration of erections after prostatectomy. The striking difference in the incidence of CVOD between the treatment and control groups (17 vs. 53%, respectively) would seem to indicate that this is the penile vascular pathology prevented by early restoration of erections. 40 The impressive results of this study are tempered by its small numbers as well as the 20% attrition rate in the treatment group. To date, these results have not been replicated in a large prospective study.
The role for PDE5i's in the treatment of postprostatectomy ED has been well-established. However, their utilization in the setting of postprostatectomy penile rehab is more controversial. The main argument against their ability to restore spontaneous erections in these patients is that PDE5i's require the production of NO in order to have their effect. Thus, they would not be expected to be particularly effective in patients who have ED resulting from postsurgical cavernosal neuropraxia or injury. However, the results of several animal models as well as clinical studies have offered potential mechanisms for the efficacy of PDE5i's in this setting. In a study performed by Ferrini et al the administration of vardenafil to rats after cavernosal neurotomy reduced the incidence of smooth muscle loss and cavernosal fibrosis. This is thought to be due to an increase in intracellular cGMP in smooth muscle cells. 41 In another animal model study, administration of sildenafil to rats within 24 hours of stroke was associated with increased neurogenesis and decreased neurologic deficits. This study suggests that PDE5i's may possess neuroprotective properties. 42 Additionally, there is evidence PDE5i's can promote endothelial health as demonstrated by an increase in the number of circulating endothelial progenitor cells in humans as well as increasing cavernous endothelial cells in diabetic rats.43,44
Much of the initial interest regarding the use of PDE5i's in postprostatectomy penile rehabilitation was in response to a study by Padma-Nathan et al presented at the 2003 American Urological Association (AUA) Annual Meeting. In this study, 76 men with normal preoperative erectile function (defined as a combined score of 8 when answering SEP2 and SEP3 as well as normal NPT testing by RigiScan) having undergone radical retropubic prostatectomy with bilateral nerve-sparing were randomized to receive nightly sildenafil 50 mg (n = 23), sildenafil 100 mg (n = 28), or placebo (n = 25) starting 4 weeks postoperatively and continuing for 36 weeks. The patients were then reassessed 8 weeks after the treatment period (postop week 48) with SEP2, SEP3, and their response to the following question: “Over the past 4 weeks, have your erections been good enough for satisfactory sexual activity?” Fourteen of the fifty-one (27%) patients who received nightly sildenafil compared to 1 of 25 (4%) patients in the placebo group reported the return of spontaneous erectile function (P = 0.0156). 45 The authors propose that the sevenfold increase in the incidence of spontaneous erections when compared to the placebo group offers definitive evidence of the efficacy of nightly sildenafil. However, the rates of erectile function in both groups are far lower than those reported on prostate cancer outcomes studies. Thus, the applicability of these data is questionable.
In 2008, Montorsi et al reported on a large multicenter, prospective, randomized, double-blind, placebo-controlled, crossover trial evaluated the efficacy of nightly versus on-demand vardenafil in the treatment of postprostatectomy erectile dysfunction. In this study 668 men with normal preoperative erectile function scheduled to undergo bilateral nerve-sparing radical prostatectomy were randomized receive vardenafil 10 mg nightly with placebo on-demand, nightly placebo with flexible dose vardenafil on-demand, or placebo nightly and on-demand for 9 months. Following the initial 9 months, there was a 2 month washout period with placebo. Finally, patients entered a 2-month period open-label vardenafil on demand. This study was designed to both evaluate the efficacy of vardenafil on demand versus nightly administration in restoring function erections. Additionally, the washout period followed by an open label period was designed to determine whether early administration nightly or on-demand vardenafil could improve long term erectile function rates. Four hundred twenty-three men completed the study. As depicted graphically in Figure 3, at the end of the initial 9-month double-blind treatment period, the proportion of patients reporting an IIEF score of ≥22 was 24.8%, 32.0%, 48.2% in those receiving placebo, nightly vardenafil and vardenafil on demand, respectively (P < 0.0001 for vardenafil on demand vs. placebo). Additionally, the difference in patients reporting an IIEF score of ≥22 was statistically higher in the on-demand versus nightly vardenafil groups at several points during the double-blind period (P = 0.0065). No significant difference in the proportion of men reporting an IIEF Score of ≥22 was appreciated between the three groups at the end of the single-blind washout or open label on demand periods of the study. 46 Thus, this study provides powerful evidence against the efficacy of vardenafil (and other PDE5i's) in restoring spontaneous erections in men with initial postprostatectomy ED.
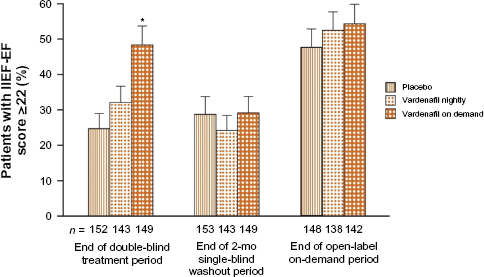
Percentage of patients with IIEF-EF score ≥22 at the end of double-blind, single-blind washout, and open label on demand periods. Reproduced with permission from Elsevier.
Conclusion
Over a decade after initial FDA approval, PDE5is remain the first line treatment for erectile dysfunction. This is due to excellent efficacy in the setting of relatively few adverse effects. Vardenafil has been associated with excellent success in treating ED in the setting of multiple medical and surgical comorbidities. The superior potency and selectivity for PDE5 when compared to the other two commercially available PDE5i's has not been demonstrated to translate into clinical superiority. However, further comparative studies are necessary.
Disclosure
This manuscript has been read and approved by all authors. This paper is unique and is not under consideration by any other publication and has not been published elsewhere. Dr. Dean has received a research grant from Pfizer Co. Dr. Rice and the peer reviewers of this paper report no conflicts of interest. The authors confirm that they have permission to reproduce any copyrighted material.