
Abstract
The HER-2/neu gene product is a 185 kDa Type I receptor tyrosine kinase which consists of an extracellular domain, transmembrane domain, kinase domain, and cytoplasmic tail. The initial discovery that amplification and subsequent overexpression of the HER-2/neu oncogene plays a pivotal role in the pathogenesis of 20%–25% of breast cancers has since led to significant clinical advances in the management of this subtype of breast cancer. The first approved HER2-targeted therapy, trastuzumab, is a humanized monoclonal antibody against the extracellular domain of HER2 and has demonstrated survival benefits in both the metastatic and adjuvant settings. Lapatinib, a small molecule tyrosine kinase inhibitor of both the epidermal growth factor receptor (EGFR) and HER2 is now also approved for advanced HER2-amplified breast cancer and is currently being evaluated in the adjuvant setting. Importantly, lapatinib has been shown to have activity in women with HER2-amplified breast cancer that is refractory to trastuzumab. In addition, it has been shown to extend survival in the front-line setting in combination with letrozole for estrogen receptor (ER) positive, HER2-positive breast cancer. Here we will review the biologic rationale and pre-clinical data that drove its initial clinical development as well as current clinical data and ongoing studies.
Introduction
Breast cancer is a leading cause of morbidity and mortality worldwide with over a million cases yearly. 1 Despite modern advances in adjuvant therapy for early-stage breast cancer, disease recurrence remains a significant issue. Given the poor prognosis associated with metastatic breast cancer, it is therefore critical to identify specific genetic alterations in the quest to develop more effective targeted therapies in this population. Recent data using microarray technology has increased our understanding of the molecular heterogeneity of breast cancer, and is giving insight into new therapeutic approaches.2–5
However, many years before the advanced technology that is available today, in 1987 Slamon et al observed that the HER-2/neu oncogene is amplified and overexpressed in 20%–25% of breast cancers. In addition, those women that had the alteration had a worse prognosis.6,7 Amplification of HER2 results in homo-and heterodimerization with other ErbB family members and propagation of cell proliferation, survival, and angiogenic pathways. 8 These observations provided support for pre-clinical studies that drove the development of trastuzumab, a humanized monoclonal antibody against the HER2 extracellular domain.9,10 Rapidly, these observations were translated to the clinic and have become the standard of care for women with metastatic and early-stage HER2-amplified breast cancer.11,12
Despite the clinical success of trastuzumab, still primary and acquired resistance remains an important clinical dilemma in HER2-amplified metastatic breast cancer. Lapatinib, a small molecule tyrosine kinase inhibitor against EGFR and HER2, has shown promise in this setting. In the pivotal Phase III study in advanced, HER2-amplified trastuzumab-treated breast cancer, the combination of capecitabine and lapatinib demonstrated an increased time-to-progression (TTP) and response rate (RR) compared with capecitabine alone. 13 In addition, for women with HER2-amplified breast cancer that has not been treated with trastuzumab (ie. front-line setting), lapatinib has been shown to improve outcomes for women in combination with letrozole 14 and paclitaxel. 15
Here we will review HER2 biology as well as proposed mechanisms of resistance to anti-HER2 therapies, pre-clinical data leading to the development of lapatinib, and contemporary trials of lapatinib in metastatic and early-stage breast cancer.
The ErbB/HER Family
The ErbB receptor family plays a key role in the regulation of cell proliferation, differentiation, division, and survival. 8 HER2 (human epidermal growth factor receptor 2; ErbB2) is one of four members in the ErbB/HER family of transmembrane glycoprotein receptors which also include the epidermal growth factor receptor (EGFR)/ErbB1/HER1, ErbB3/HER3 and ErbB4/HER4. Unlike in experimental models, 16 in human disease, HER2 gene amplification, rather than activating kinase domain mutations, is the primary mechanism for increased HER2 activity.6,7
Signaling through the ErbB//HER family is complex. 8 There are 11 known ligands that interact with various family members including epidermal growth factor (EGF), transforming growth factor (TGF) alpha, amphiregulin (AR) and epigen (EPG); betacellulin (BTC), heparin-binding EGF (HB-EGF), and epiregulin (EPR) and neuregulins (NRG-1, NRG-2). All of the HER-family receptors except for HER2 have a known ligand. In that sense, HER2 is an “orphan receptor”. In addition, HER3 has a non-functional kinase and relies on heterodimerization with other members, preferably HER2 for signal transduction. Ligand binding to other HER-family members induces auto-phosphorylation of the intracellular tyrosine kinase domain resulting in conformational changes and subsequent heterodimerization with HER2, which again has no known ligand of its own. Receptor dimerization initiates a signaling cascade beginning with Src-homology-2 (SH2) domain, which propagates along two main downstream effector pathways, the Ras-Raf-MAPK (Erk1/2) pathway regulating cell division and proliferation, and the PI3K-Akt-mTOR pathway regulating cell growth and survival. Upregulation of the PI3K/Akt pathway secondary to HER2/HER3 heterodimerization and activation plays a particularly crucial role in driving HER2-positive breast cancer progression.17,18
Trastuzumab: Mechanisms of Action
Based on in vitro and in vivo data, various mechanisms have been identified for the activity of trastuzumab, a humanized monoclonal antibody against the extracellular domain of HER2. These include downregulation of the ErbB2 receptor via endocytosis, 19 antibody-dependent cell cytotoxicity (ADCC), 20 increased PTEN activation via membrane localization, 21 G1 growth arrest induction, 22 and suppression of angiogenesis. 23 A detailed review was recently published. 24
Trastuzumab: Mechanisms of Resistance
Primary and acquired resistance to trastuzumab is frequently encountered in the clinic, with multiple postulated mechanisms. Cross-talk between HER2 and insulin-like growth factor-1 receptor (IGF-1R), evidenced by increased HER2 phosphorylation with IGF-1 stimulation in resistant cells but not in parental trastuzumab-sensitive SKBR3 breast cancer cells, is one potential mechanism. 25 Second, the presence of p95-HER2, a truncated form of the HER2 receptor which lacks the extracellular binding domain for trastuzumab, has been reported as contributing to trastuzumab resistance. 26 Third, trastuzumab resistance in HER2-overexpressing cell lines and primary tumors has been associated with deficiency of PTEN (phosphatase and tensin homologue deleted on chromosome 10), a tumor suppressor which mediates the PI3K/Akt pathway and which has been identified in almost 50% of breast cancers. 21 Similarly, a fourth mechanism of trastuzumab resistance relates to hyperactivation of the PI3K/Akt pathway, including activating mutations in the p110-alpha subunit of PI3K which has been reported in up to 25% of breast cancers.27,28 In one study, trastuzumab resistance associated with the PIK3CA mutations E545K and H1047R were identified in four breast cancer cell lines. 28 Fifth, Dokmanovic et al recently reported that Rac1, a Ras-like small GTPase, contributes to trastuzumab resistance by affecting trastuzumab-mediated endocytosis of the ErbB2 receptor. 29 Using trastuzumab-conditioned SKBR3 cell lines (Clone 3), Rac1 activity was found to be increased in GTPase activity pull-down assays and Western blot analysis compared with parental cells. Further, trastuzumab sensitivity and trastuzumab-mediated endocytic downregulation of ErbB2 was restored when used in combination with NSC23766, a novel Rac1-specific inhibitor.
Lapatinib: Mechanisms of Action
Lapatinib ditosylate (GW2016; GW572016; Tykerb®), a member of the quinazoline family with a 4-anilinoquinazoline core, is a reversible, small molecule tyrosine kinase dual inhibitor of EGFR and HER2. In contrast to trastuzumab which binds to the extracellular domain of HER2, lapatinib exerts its activity intracellularly by competing with ATP for the ATP-binding domain in the cytoplasmic tail of the tyrosine kinase receptor. Inhibition of tyrosine kinase phosphorylation is its major mechanism of action, which dampens and/or abrogates signal transduction along the PI3K/Akt and the ras/raf/MAPK pathways (Fig. 1). Compared with erlotinib and gefitinib (two isolated EGFR-specific tyrosine kinase inhibitors), lapatinib binds to an inactive-like conformation of EGFR and has comparatively slower inhibitor dissociation rates, with estimated Ki-app values of 3 nM and 13 nM against EGFR and ErbB2 respectively. 30 In EGFR-overexpressing HN5 cells, this correlated with prolonged downregulation of EGFR phosphorylation.
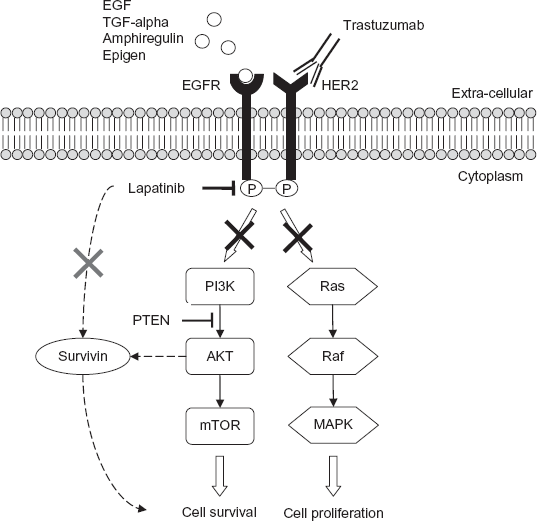
Mechanism of action of lapatinib. Intracellularly, the dual-targeted small molecule inhibitor lapatinib reversibly binds to the cytoplasmic ATP-binding sites of EGFR/HER1 and HER2 receptors, thereby blocking tyrosine kinase phosphorylation. This results in reduced signal transduction activity along two main effector pathways, PI3K/Akt/mTOR and Ras/Raf/MAPK, leading to deleterious effects on cell survival and proliferation, respectively. Downregulation of survivin, a member of the inhibitor of apoptosis family (IAP) of proteins, represents a postulated mechanism. In contrast, the monoclonal antibody trastuzumab exerts its activity by binding to the extracellular domain of HER2, as illustrated.
Unlike trastuzumab, the anti-tumor activity of lapatinib does not appear to depend on PTEN, a mediator of the PI3K-Akt pathway. 31 Rather, it is postulated that the anti-tumor effects of lapatinib may be related to survivin, a member of the inhibitor of apoptosis family (IAP) of proteins. 32 Using HER2-overexpressing cell lines, lapatinib resulted in significant downregulation of survivin protein with associated apoptosis. 33 Combining lapatinib with trastuzumab, or lapatinib plus fulvestrant, resulted in increased apoptosis and significant downregulation of downregulation of survivin.32,34
Recently, in vitro work using HER2-overexpressing breast cancer cell lines (SKBR3 and MCF7-HER2) and correlation with in vivo data using BT474 xenografts also indicated that lapatinib not only inhibited HER2 phosphorylation, but also decreased HER2 receptor ubiquitination and increased the accumulation of inactive HER2 receptors at the cell surface. 35 The combination of lapatinib plus trastuzumab was also found to potentiate ADCC-mediated cytotoxicity. Currently, clinical trials evaluating the combination of lapatinib plus trastuzumab in the metastatic and adjuvant settings are in progress, with promising early results.36,37
Early Pre-Clinical Studies of Lapatinib
One of the initial in vitro and in vivo studies utilizing lapatinib was reported by Rusnak et al in 2001. 38 In vitro inhibition of purified EGFR and ErbB2 kinases, and of cell growth assays of various human tumor-derived cell lines with EGFR or ErbB2 overexpression were performed. 50% inhibitory concentrations (IC50) values for enzyme inhibition were 10.8 nM for EGFR and 9.2 nM for ErbB2. In the breast cancer cell line BT474, characterized by ErbB2 overexpression and low levels of EGFR expression, 72 hr treatment with lapatinib demonstrated strong potency with IC50 values of 0.10 ± 0.03 μM, compared with a 30–40 fold difference of 3.0–4.0 μM in two breast cancer cell lines with low expression of both EGFR and ErbB2 (MCF-7 and T47D). Cell cycle flow cytometric analysis identified apoptosis in BT474 cells after 72 h of lapatinib exposure at 1 or 10 μM, as represented by an increased number of events with sub-2N DNA. In comparison, G1 growth arrest rather than apoptosis was primarily seen in the EGFR-overexpressing head and neck cancer cell line, HN5. On immunoprecipitation and Western blot analysis of the BT474 and HN5 cell lines, dose-responsive inhibition of EGFR and ErbB2 phosphorylation, as well as greater inhibition of Akt phosphorylation was found in BT474, corresponding to decreased PI3K/Akt signal transduction along the ErbB pathway. Finally, in vivo data with BT474 tumor xenograft models correlated with the in vitro findings, which demonstrated complete inhibition of tumor growth at an oral dose of 100 mg/kg given twice daily.
In 2002, Xia et al reported the effects of lapatinib on ErbB downstream signal transduction pathways. 39 In vitro studies using HN5 (EGFR overexpression) and S1, an ErbB2 transfected HB4a cell line sub-clone (characterized by high levels of phosphorylated ErbB2 protein), found that lapatinib exposure for 72 hr inhibited phosphorylated Erk1/2 in a dose-dependent manner, with complete inhibition at 5 μM. Consistent with the earlier report, lapatinib exposure for 24 hr in the presence of EGF stimulation resulted in significant inhibition of Erk1/2 and Akt phosphorylation in both BT474 and HN5 cell lines, at 1 μM and 5 μM respectively. In S1 cells, 72 hr exposure to lapatinib also resulted in significant apoptosis, with a 23-fold increase to 46% from 2% in vehicle-treated controls. In vivo studies with HN5 tumor xenografts using pre- and post-treatment tumor implant biopsies (to minimize inter-animal variability in baseline expression of activated EGFR and ErbB2) demonstrated inhibition of EGFR, Erk1/2, and Akt phosphorylation using a lapatinib dose of 30 mg/kg in post-treatment biopsies compared with pre-treatment. Overall, these study results are in keeping with those reported by Rusnak et al.
Lapatinib Sensitivity in Trastuzumab-Resistant Models
A key pre-clinical study assessing the use of lapatinib in the setting of trastuzumab resistance in HER2-positive breast cancer cell lines was reported by our laboratory in 2006. 40 Using a panel of 31 breast cancer cell lines, which included 3 trastuzumab-conditioned HER2-overexpressing cell lines, a dose-dependent inhibitory effect on cell growth in vitro was observed with lapatinib. However, a significant range of IC50s, up to a 1000-fold difference (0.010–108.6 μM), was seen between the individual cell lines. Importantly, cell lines with HER2 gene amplification and protein expression had marked lapatinib sensitivity with IC50s of less than 1 μM. Cell lines with high EGFR expression, however, had comparatively higher IC50s (4.7–78.6 μM). Immunoprecipitation and Western blotting demonstrated inhibition of HER2, Raf, Erk, and Akt phosphorylation in this subgroup with significant lapatinib response. Cell cycle analysis corroborated these findings with an increased apoptotic signal, as evidenced by a greater percentage of cells with sub-2N DNA (5% vs. 26% vs. 43%, for control vs. lapatinib at 0.1 μM and 0.5 μM). In long-term outgrowth assays (.9 months) to develop trastuzumab-conditioned HER2-overexpressing cell lines, in vitro resistance to trastuzumab was acquired while sensitivity to lapatinib was maintained. In vivo testing with BT474 xenografts showed consistent results, with significantly smaller tumor volumes in mice treated with 75 mg/kg of lapatinib twice daily for 77 days compared with vehicle-treated controls. Finally, synergism with lapatinib plus trastuzumab were also observed in four HER2-overexpressing cell lines, analyzed using the median effect/combination index (CI) isobologram method. This observation has gone on to be confirmed in human studies. 37
Similarly, in support of the data reported by Konecny et al, non-cross-resistance between lapatinib and trastuzumab was also reported in the HER2-overexpressing SKBR3 breast cancer cell line. 41 Consistent with previously reported data, inhibition of EGFR and HER2 signaling was observed in resistant cells with lapatinib use, as evidenced by decreased activation of downstream Akt, MAPK, and S6 kinases. Given the association between IGF-1 signaling and trastuzumab resistance, the authors also demonstrated that lapatinib use in trastuzumab-resistant cells resulted in reduced IGF-1R phosphorylation despite IGF-1 stimulation. Taken together, these two pre-clinical studies successfully highlighted the anti-tumor efficacy of lapatinib in the setting of trastuzumab resistance.
Lapatinib Dependence on EGFR vs. HER2
The relative contribution of its activity against EGFR in HER2-amplified breast cancer is unclear. Preclinical data suggest that HER2 inhibition is likely most important.40,41 To further investigate the role that EGFR plays in lapatinib efficacy, Zhang et al utilized an EGFR siRNA knockdown strategy in two HER2-overexpressing cell lines, BT474 and SKBR3. 42 They reported that EGFR depletion with siRNA knockdown did not affect lapatinib sensitivity when compared with controls, suggesting that HER2, rather than EGFR inhibition, is the primary mediator of lapatinib efficacy. Consistent with this data, a higher affinity of lapatinib for HER2 monomers over EGFR monomers has been reported. 35 Recently, a retrospective biomarker study encompassing two large randomized Phase 3 trials (EGF30001, paclitaxel +/- lapatinib in HER2-negative/unknown metastatic breast cancer; and EGF100151, capecitabine +/- lapatinib in HER2-positive metastatic breast cancer) found no correlation between lapatinib responsiveness and EGFR expression (using immunohistochemistry or mRNA levels), regardless of HER2 status. 43 Based on these results, the anti-tumor efficacy of lapatinib in HER2-positive breast cancer can most likely be attributed to inhibition of HER2, rather than EGFR.
In Vitro and in Vivo Mechanisms of Lapatinib Resistance
Despite the positive results from the Phase III trial which resulted in US FDA approval of lapatinib in the setting of HER2-overexpressing, trastuzumab-refractory metastatic breast cancer, clinical resistance to lapatinib is frequently observed. Unlike trastuzumab, co-expression of IGF-1R or presence of p95-HER2 does not appear to contribute to lapatinib resistance. In fact, Spector et al reported that IGF-1R co-expression appeared to predict for response to lapatinib. 44 Likewise, inhibition of signal transduction with lapatinib in truncated ErbB2 receptor (p95-HER2) BT474 transfected cells in vitro, 45 as well as anti-tumor effects in vivo using p95-HER2 derived breast cancer cell lines, have been reported. 26
One postulated mechanism underlying lapatinib resistance is increased estrogen receptor (ER) crosstalk and signaling.34,46 In one study, gene expression profiling was used to compare differences in baseline gene expression between lapatinib-conditioned BT474 cell lines with acquired resistance (rBT474) to lapatinib-sensitive parental cell lines. 34 57 genes were identified as differentially expressed and upregulated greater than 3-fold in rBT474 compared with parental cells. Pathway analysis revealed increased transcriptional activity and protein levels of ER-associated signaling genes, including FOXO3a and caveolin-1. Further, dual inhibition of ErbB2 and ER pathways using 500 nM of lapatinib and ER-specific siRNA knockdown, respectively, in rBT474 cells resulted in increased apoptosis compared with single pathway inhibition. In the second study, gene expression profiling showed that lapatinib upregulated the expression of ER and PR (progesterone receptor) in BT474 and T47D cell lines by 7–11 fold, which further supports the importance of crosstalk between the ErbB and hormone receptor pathways. 46 Additionally, differential gene expression and downregulation of Akt pathway transcripts (AKT1, MAPK9, HSPCA, IRAK1, CCND1) by 7–25 fold was observed in lapatinib-responsive (BT474, SKBR3) vs. lapatinib non-responsive cell lines (MDA-MB-468, T47D), characterized by high vs. low basal ErbB2 protein expression, respectively.
In a recent study, Trowe et al reported that 17 different ErbB2 mutations secondary to amino acid substitutions conferred resistance to lapatinib based on in vitro screening. 47 Using a randomly mutated ErbB2 expression library in Ba/F3 cells and structural computer modeling, direct steric interference and restriction of conformational flexibility were identified as contributors to lapatinib resistance, with the ErbB2 T798I mutation showing the highest frequency and strongest in vitro resistance. In addition, testing of a novel compound EXEL-7647, an EGFR/ErbB2/VEGFR inhibitor, revealed in vitro activity in almost all lapatinib resistance-associated mutations.
Hyperactivation of the PI3K pathway and PIK3CA mutations have been associated with trastuzumab resistance,27,28 and have also been reported to confer resistance to lapatinib. 48 Using a genome-wide, loss-of-function short hairpin RNA screening strategy in BT474 cell lines, lapatinib resistance was found to be associated with 2 dominant activating mutations in PIK3CA, E545K and H1047R. Furthermore, the novel compound NVP-BEZ235, a dual inhibitor of PI3 K/mTOR, was shown to reverse PI3 K-induced lapatinib resistance. Additionally, the authors also identified the tumor suppressor PTEN as a potential modulator of in vitro and in vivo lapatinib sensitivity.
Finally, Liu et al reported that overexpression of AXL, a membrane-bound tyrosine kinase receptor, also contributes to lapatinib resistance via crosstalk between HER, AXL, and ER receptor pathways. 49 Using lapatinib-conditioned BT474 cells, elevated levels of AXL, attributed to promoter hypo-methylation, were detected via Western blotting and mass spectrometry-based peptide sequencing. The addition of a multi-kinase inhibitor of AXL, MET, and VEGFR (GSK1363089; foretinib), siRNA to AXL, estrogen-deprived growth conditions, or the ER antagonist fulvestrant to lapatinib in vitro all resulted in decreased AXL expression and restoration of lapatinib sensitivity in these cells.
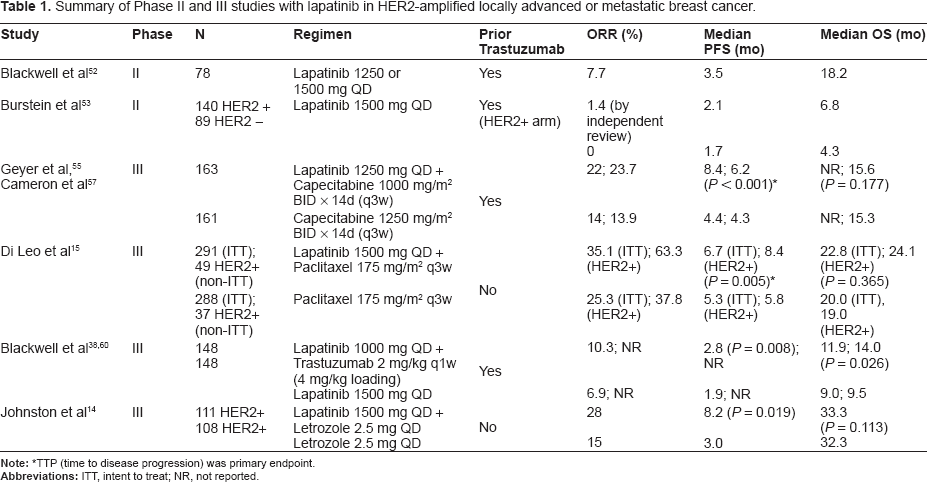
Clinical Development of Lapatinib (Table 1)
Summary of Phase II and III studies with lapatinib in HER2-amplified locally advanced or metastatic breast cancer.
One of the first proof-of-concept studies with lapatinib was performed in a Phase I study of 67 patients with heavily-pretreated metastatic solid tumors whom on biopsy had demonstrated expression of EGFR and/or HER2 by immunohistochemistry (IHC). 50 These patients had a Karnofsky performance status of ≥70% and a life expectancy of at least 12 weeks. The patients were randomly assigned to receive one of five doses of lapatinib, which was given daily for 21 days. The included doses were 500, 560, 900, 1200, and 1600 mg. This Phase I study included patients with breast, colorectal, head and neck, ovarian and lung primary malignancies. The most frequently reported adverse events were diarrhea (42%), rash (31%) and fatigue (10%). Furthermore, there were no drug-related reductions in left ventricular ejection fraction (LVEF).
Of the 59 assessable patients, four patients experienced partial responses. All four patients had breast cancer and HER2 over-expression (3+ by IHC) and with one exception, co-expression of EGFR. All of the four responders had previously been treated with trastuzumab, either alone or in combination with chemotherapy. The median duration of treatment for patients with partial response (PR) was 5.5 months. Stable disease (SD) was reported in 24 patients, of which 10 had breast cancer. The majority of patients who responded (PR, and SD > 6 months) had received 1200 mg daily of lapatinib. These data were encouraging and supported by the earlier pre-clinical studies of lapatinib in HER2-amplified models.
Given the apparent activity of lapatinib in the HER2-amplified breast cancer population, Blackwell et al evaluated the efficacy and safety of lapatinib in an open-labeled, single-group, multi-center, phase II study in HER2-overexpressing advanced or metastatic breast cancer patients. 51 These patients had progressed on trastuzumab therapy and were treated with a daily dose of 1500 mg of lapatinib, which was taken daily until disease progression or withdrawal from study. The primary endpoint was tumor response rate (complete response (CR) or PR). Secondary endpoints included clinical benefit rate (CR, PR, or SD $ 24 weeks), time-to-response, duration of response, progression-free survival (PFS), and OS.
A total of 78 women were enrolled in the study. At study entry, nearly all patients had stage IV disease with two or more metastatic sites (76%). In the ITT (intent-to-treat) population, the tumor response rate was 7.7% as assessed by the investigators and 5.1% as assessed by independent review. In addition, five patients (6%) had SD for ≥24 weeks. The clinical benefit rate was 14.1% by investigator review and 9.0% by independent review. The time to first tumor response ranged from 8 to 16 weeks, and the duration of response ranged from 9 to 42 weeks. The 4- and 6-month PFS rates were 41% and 21%, respectively. Median OS was 79 weeks, and the 4- and 6-month survival rates were 89% and 85%, respectively.
Lapatinib was well-tolerated in this study. Compliance was in excess of 90%. 90% of patients did experience one or more treatment-related adverse events. The most common treatment-related adverse events were rash (67%), diarrhea (46%), and nausea (31%). Grade 3 rash and diarrhea were reported in 4% and 9% of patients, respectively. One patient did develop a grade 2 drop in LVEF, which was attributed to the study drug.
An additional Phase II study evaluated lapatinib monotherapy in chemotherapy-refractory breast cancer patients who were both HER2-positive and negative. 52 A total of 229 women with refractory advanced or metastatic breast cancer were enrolled in two cohorts depending on their HER2 status. Cohort A (HER2-positive) consisted of 140 patients, and cohort B (HER2-negative) enrolled 89 patients. 97% of patients in the HER2-amplified arm had received prior trastuzumab. In addition, with the HER2-negative arm, the study aimed to explore the potential for dual inhibition of EGFR and HER2 in breast cancers that were not HER2-amplified. These patients had 3 or more metastatic sites and 73% had both visceral and non-visceral involvement. The most common metastatic sites were bone, liver, lymph nodes, and lung. Almost all patients had received three or more lines of chemotherapy prior to study enrollment. Patients received 1500 mg of lapatinib daily.
In the HER2-amplified cohort, the response rate by investigator assessment was 4.3% (three CR and three PR), compared with 1.4% (two PR) by independent review. In addition, 2 patients had SD for ≥24 weeks on independent review. Overall, 5.7% of patients derived clinical benefit. In contrast, no objective tumor responses were reported in the HER2-negative cohort. The median TTP and PFS were both 9.1 weeks in the HER2-positive and 7.5 weeks in the HER2-negative cohort. Consistent with other trials, the most common toxicities were diarrhea, nausea, and rash. Grade 4 adverse events occurred in 6% of patients (eg, gastrointestinal disorders, increased bilirubin, hypercalcemia, and renal failure). Only one patient (<1%) experienced a grade 3 decrease in LVEF, while eight others (3%) were asymptomatic (grade 1 or 2).
With the above data from pre-clinical and early clinical studies, a pivotal trial evaluating the benefit of adding lapatinib to capecitabine in metastatic breast cancer patients who had progressed on first-line therapy with trastuzumab was performed. The safety of lapatinib and capecitabine was previously shown in a Phase I study by Chu et al. 53 In the Phase I study, lapatinib was given at a dose of 1250 mg daily and capecitabine at a dose of 2000 mg per square meter of body-surface area daily on days 1 through 14 of a 21-day cycle. The adverse events of the combination were no different than either drug alone. With these results, a phase III randomized, open-labeled study comparing lapatinib plus capecitabine vs. capecitabine alone in women with progressive, HER2-positive, locally advanced or metastatic breast cancer was conducted. 13 Inclusion criteria included that women had to have received anthracyclines, taxane, and trastuzumab previously. A total of 324 patients were enrolled in the study, with 163 receiving combination therapy and 161 receiving monotherapy. The two groups were well-balanced, and most patients (96%) had metastatic disease. The median TTP was 8.4 months with combination therapy vs. 4.4 months with monotherapy, with a hazard ratio (HR) of 0.49 and P < 0.001. The overall response rates were 22% in the combination vs. 14% in the monotherapy groups, which did not reach statistical significance. Interestingly, central nervous system (CNS) as the first site of progression occurred in 4 patients in the combination group compared to 11 patients in the monotherapy group, although this difference was not statistically significant (P = 0.10). In a separate, multi-center phase II study evaluating the efficacy of lapatinib in women with progressive brain metastases following prior trastuzumab treatment for HER2-positive breast cancer, a modest 6% CNS objective response rate (of 242 patients) was demonstrated, highlighting the promising CNS anti-tumor activity of lapatinib in this setting. 54 In the phase III Geyer study above, common adverse events included diarrhea, hand-foot syndrome, nausea, vomiting, fatigue, and rash distinct from hand-foot syndrome in the combination group. 13% of patients in the combination group discontinued the medication compared to 12% in the mono-therapy group. While there were 4 asymptomatic cardiac events in the combination group, there were no symptomatic cardiac events, and lapatinib was not discontinued due to a decrease in LVEF.
An updated analysis of the Geyer study was published in 2008 to reflect the most recent efficacy and biomarker data. 55 At the closure of the trial, an additional 75 patients (a total of 399 patients) had been enrolled. 84 patients were still on study, 161 were alive, and 119 had died. The median TTP improved from 4.3 months in monotherapy arm to 6.2 months in the combination arm. Similar results were also seen for PFS with a HR for PFS of 0.59 for the combination arm relative to the monotherapy arm. The overall response rate was 24% in the combination group compared with 14% in the monotherapy group, with an odds ratio of 1.9 in favor of the combination group. Results of biomarker analysis suggested that HER2-positive status by FISH (fluorescent insitu hybridization) analysis provided a better discrimination for prediction of benefit from addition of lapatinib than immunohistochemistry (IHC). Furthermore, higher levels of circulating HER2 extracellular domain (ECD) were associated with a shorter PFS in the capecitabine-alone arm, the high ECD levels did not predict for poorer outcome in the combination therapy group, and perhaps patients with very high ECD levels may have an additional benefit from lapatinib. A large analysis of the potential predictive value of HER2 ECD in another lapatinib cohort did not show any clear clinical utility. 56
Randomized data of lapatinib in a previously untreated population was evaluated in the EGF 30001 study. 15 This trial evaluated the efficacy and tolerability of lapatinib and paclitaxel versus paclitaxel alone as first-line treatment of metastatic breast cancer in a HER2-negative or untested patient populations. The study was a randomized, multi-center, double blind trial, randomizing patients to lapatinib 1500 mg daily with paclitaxel (175 mg/m2 intravenously over 3 hours on day 1, every 3 weeks) or paclitaxel and placebo. The trial enrolled 580 patients. The overall response rate and clinical benefit rate were significantly higher in the lapatinib-paclitaxel arm versus paclitaxel-placebo group, with complete or partial responses seen in 35% of patients in the paclitaxel-lapatinib group compared to 25% on paclitaxel-placebo arm. There was however no statistically significant differences in terms of TTP, event-free survival (EFS), or OS. After centralized, blinded review of HER2 status, 86 patients (15%) were confirmed as being HER2-amplified. This group of patients had a significant improvement in TTP with the addition of lapatinib to paclitaxel versus paclitaxel alone (36.4 versus 25.1 weeks; HR = 0.53). The EFS was also significantly longer in the combination arm versus paclitaxel-placebo arm (35.1 vs. 21.9 weeks). Finally, the overall response rate (ORR) (63.3% vs. 37.8%, respectively; P = 0.023) and clinical benefit rate (CBR) (69.4% vs. 40.5%, respectively; P = 0.011) were significantly higher for the combination. As seen in other studies with lapatinib, there was no significant benefit seen in terms of ORR, CBR, TTP, EFS, or OS in the HER2-negative patients. Further biomarker evaluation of this latter group has been performed and suggests a relationship between steroid hormone receptor levels and response to lapatinib. 57
As mentioned above, pre-clinical data indicate that complete HER2 blockade with lapatinib and trastuzumab in HER2-positive breast cancer cells is synergistic. 40 A randomized phase III study evaluating the combination of trastuzumab and lapatinib versus lapatinib alone was initiated in women with prior trastuzumab treatment. 37 In this study, a total of 296 patients (148 per treatment arm) were randomly assigned. The two groups were well-balanced in regards to their disease characteristics. The majority (73%) had visceral disease, and both groups had received a median of three prior trastuzumab regimens for metastatic disease. The study showed a statistically significant improvement in PFS for the combination of lapatinib with trastuzumab compared to single-agent lapatinib with a HR of 0.73 (12 weeks with combination compared to 8.1 weeks with lapatinib alone). Furthermore, the percentage of patients whose disease was progression-free at 6 months doubled with the combination compared to the monotherapy arm (28% vs.13%, respectively; P = 0.003). The clinical benefit rate was 24.7% in the combination arm compared to 12.4% in the single-agent arm (P = 0.01). The data at the time of publication also showed a trend towards overall survival improvement in favor of the combination arm, with an OS of 51.6 weeks for combination compared to 39.0 weeks for the single-agent arm. The incidence of most adverse events was similar between the two arms, with only diarrhea being more frequent in the combination arm than the single-agent arm. Recently, the survival data was updated at the San Antonio Breast Cancer Symposium (SABCS) where the overall survival for the lapatinib-alone arm was 9.5 months compared to 14 months for the combination arm. 58 These data were statistically significant with a P-value of 0.026 and HR of 0.74.
Cross-talk between peptide growth factor signaling and steroid hormones have been implicated in resistance to endocrine therapy. 59 To test this hypothesis EGF 30008 was a randomized, double-blind, multi-center, phase III study of post-menopausal women with advanced or metastatic breast cancer who had not received any prior therapy for their disease. 1,286 patients with hormone receptor-positive metastatic breast cancer were randomized to receive letrozole plus lapatinib (n = 642) or letrozole plus placebo (n = 644). This included 219 patients with HER2-amplified breast cancer, while the remainder were HER2-negative. While there was no significant benefit from the addition of lapatinib to the HER2-negative patients, in those that were HER2-amplified, the median PFS was increased to 8.0 months for the letrozole-lapatinib group compared to 3.0 months in the letrozole alone group. The ORR also improved from 15% to 38% for the letrozole-lapatinib group. Again, a blinded retrospective biomarker study of the HER2-negative patients as in EGF 30001 suggests that those patients with lower ER expression may benefit from the addition of lapatinib. 60
Future Directions
The success of HER2-directed therapies in the adjuvant setting has decreased the incidence of HER2-amplified metastatic breast cancer. Still, there is a need for new approaches to treating HER2-driven breast cancer. Currently, there is a large adjuvant study evaluating lapatinib in the adjuvant setting for HER2-amplified breast cancer. The ALTTO (Adjuvant Lapatinib and/or Trastuzumab Treatment Optimization) trial randomizes women in the adjuvant setting to receive one of four biologic regimens after chemotherapy: 1) 1 year of trastuzumab vs. 2) 1 year of lapatinib vs. 3) 12 weeks of trastuzumab followed by a 6 week washout then 34 weeks of lapatinib or 4) 52 weeks of the combination of trastuzumab and lapatinib. This study will build on the data supporting lapatinib in advanced breast cancer and will evaluate the concept of “total HER2 blockade”. Other studies in early-stage breast cancer are focused on tissue acquisition in hopes of identifying biomarkers predictive of benefit to either trastuzumab or lapatinib. Still, no standard of care currently exists for patients with HER2-amplified breast cancer that are refractory to both trastuzumab and lapatinib. Based on pre-clinical data, inhibition of multiple signaling pathways using anti-HER2 based therapies plus novel agents appear promising. The role of AXL downregulation in this setting is intriguing but remains to be determined. Combined AXL inhibition with the multi-kinase AXL, MET, and VEGFR inhibitor foretinib (GSK1363089) is currently under evaluation in Phase II clinical trials, given that it was found to restore lapatinib and trastuzumab sensitivity in resistant cell lines with increased AXL expression. 49
A second strategy which may be useful in enhancing lapatinib efficacy involves combined inhibition of ErbB and mTOR pathways. Using semi-quantitative protein array technology, Vazquez-Martin et al reported that co-treatment of lapatinib-resistant MCF-7/HER2-Lap 10 cells with rapamycin, an mTOR inhibitor, lead to re-sensitization of the cells to lapatinib and suppression of hyperactivation of the serine-threonine kinase p70S6K1, an mTOR effector. 61 Trials testing this combination are currently underway.
As HER2-HER3 heterodimerization and activation appear to play a critical role in driving HER2-amplified breast cancer progression secondary to upregulation of the PI3K/Akt pathway, 62 interest has arisen with combined anti-HER2 and HER3 therapies. Presently, the combination of trastuzumab plus pertuzumab, another humanized monoclonal antibody against HER2 that prevents HER2-HER3 heterodimerization, is being evaluated in clinical trials of HER2-positive metastatic breast cancer.
Finally, novel compounds such as EXEL-7647, an EGFR/ErbB2/VEGFR inhibitor which has demonstrated in vitro activity against lapatinib resistance-associated mutations 47 as well as the PI3 K/mTOR inhibitor, NVP-BEZ235, 48 are promising candidates currently under investigation and may play potential roles in overcoming resistance to HER2-directed therapy.
Conclusions
Over the past decade, multiple studies conducted from bench to bedside of the EGFR/HER2 tyrosine kinase inhibitor lapatinib has led towards a greater biological understanding and established its role in HER2-positive breast cancer. Presently, its US FDA approved use is limited to HER2-overexpressing, metastatic breast cancer after refractoriness to an anthracycline, taxane, and trastuzumab. As clinical resistance to anti-HER2 therapies including lapatinib remain an issue, novel strategies to circumvent drug resistance including combinations of lapatinib plus trastuzumab, anti-estrogens, mTOR inhibitors, or HER3 inhibitors are under investigation. Results of ongoing clinical trials with these combined therapies are eagerly awaited, given their potential to revolutionalize treatment in HER2-overexpressing, trastuzumab-refractory metastatic breast cancer.
Disclosure
This manuscript has been read and approved by all authors. This paper is unique and is not under consideration by any other publication and has not been published elsewhere. The authors and peer reviewers of this paper report no conflicts of interest. The authors confirm that they have permission to reproduce any copyrighted material.
Footnotes
Acknowledgments
RYT is a Research Fellow of The Terry Fox Foundation (award #020017), Canada.