
Abstract
Biological therapies have been a major advance in RA treatment. However, remission or response is not achieved in all patients. Therefore, new drugs seem necessary. Most recent trials have focused in the development of three different groups of molecules: those against commercialized targets but minimizing side effects or improving administration, others molecules against new targets, and a third group including small molecules. Some of them have been shown to be clinically efficacious and safe in RA patients, including: two new anti-TNFα therapies (golimumab and certolizumab pegol), three anti-CD (ocrelizumab, ofatumumab and a SMIP), subcutaneous abatacept, anti-IL17 therapy, tasocitinib and fostamatinib disodium. Therefore, a wide spectrum of new RA therapeutics are promising, but more studies are necessary to confirm these results.
Introduction
Rheumatoid arthritis (RA) treatment has experienced many important advances during the last decade, and this is associated with the appearance of biological therapies. The development of these drugs was possible thanks to the development of technologies that allowed identifying substances (cytokines) or key processes in the physiopathology of RA at the end of the 20th century.
The biological therapies nowadays approved for RA treatment are effective but they still are not able to induce remission in many patients. A wide spectrum of potential therapies is being developed in numerous clinical trials that have arisen immediately after advances in knowledge of the pathogenesis of the disease. Nowadays, there are more than one thousand trials on RA, most of them focused in evaluating new targets or better route and frequency of administration, and lower immunogenicity for commercialized drugs. The aim of this review is to evaluate the efficacy and safety of the newer therapies for patients with RA.
Most of the available biological drugs for the treatment of RA are monoclonal antibodies against cytokines or chemokines. The term cytokine is applied to any protein or small and not structured glycoprotein that serves as a chemical messenger between cells (lymphocytes) and participates in different processes: 1 cellular growth and differentiation, tissue repair and remodeling, regulation of the immune response (mainly innate). Although cytokines take part in the cellular growth and normal development, they play a very important role in the inflammatory and immune responses in RA. The inflammatory and immune cells, which are the principal but not the unique cytokines producing cells, are widely distributed in all organs and tissues of the body. Cytokines produce a biological effect by binding to high affinity specific receptors located at the exterior surface of the target cells. Multiple cytokines share the same biological response. The term chemokine (chemoattractive cytokine) refers to a super-family of at least 40 low weight proteins with 4 cystein residues which are able to recruit and to activate neutrophils, lymphocytes, monocytes/ macrophages, eosinophils and basophiles. 1 They are the principal system of signals by which the inflammatory and immune cells are attracted to organs and tissues. The principal promoters of chemokines synthesis are interlukin-1 (IL-1) and tumor necrosis factor-alpha (TNFα).
Monoclonal Antibodies
Monoclonal antibodies are made by identical immune cells that are all clones of a unique parent cell. Given almost any substance, it is possible to create monoclonal antibodies that specifically bind to that substance; they can then serve to detect or purify that substance. They act by means of the neutralization of a cytokine, blockade of the co-stimulatory molecules and inducing cytolysis, apoptosis or depletion of molecules in target cells. Early on, a major problem for the therapeutic use of them was that initial methods used to produce them yielded mouse, not human antibodies, and an immune response occurred when murine monoclonal antibodies were injected into humans and resulted in their rapid removal from the blood, systemic inflammatory effects, and the production of human anti-mouse antibodies (HAMA). In an effort to overcome this obstacle, fully human antibodies are being developed to avoid some of the side effects of humanized and chimerical antibodies.
New Molecules against Commercialized Targets Drugs
Anti-TNFα
The development of TNFα inhibitor therapy has revolutionized the treatment of RA. In both early and established RA, two-thirds of patients achieve meaningful clinical responses but one-third do not respond.2–4 Additionally, a number of patients initially responding develop acquired drug resistance or gradual drug failure, and some have to discontinue the biologic treatment due to adverse events. Retention rates with the first and second TNF antagonist are 53% and 47% at 36 months respectively. 5 In this regard, new TNF antagonists are welcome additions to the treatment of RA.
Golimumab
Golimumab (GLM) is a human, subcutaneous, monoclonal antibody specific for TNFα which binds to soluble and transmembrane forms of human TNFα. It has been approved recently for the treatment of RA.
Three phase III trials determined GLM efficacy. They included patients with different previous treatment: methotrexate (MTX) naive patients (GO-BEFORE), failure to MTX (GO-FORWARD) and inadequate response to anti-TNFα (GO-AFTER).
GO-FORWARD study evaluated monthly subcutaneous injections of GLM in active RA despite methotrexate therapy. 6 Results at week 14 demonstrated that combined therapy with GLM plus methotrexate (MTX) significantly reduced the signs and symptoms of RA and improved physical function after 24 weeks. Long-term results showed that the response rates were sustained after 52 weeks of treatment. 7 The safety profile appeared to be consistent with the other approved tumour necrosis factor inhibitors although it must be noted that there are no head-to-head studies so far.
GLM efficacy was also investigated in patients with active RA after treatment with anti-TNF (GO-AFTER study). Patients enrolled had previously been treated with adalimumab (48%), etanercept (48%) and infliximab (47%), and a total of 66%, 25% and 9% of them had received one, two or three anti-TNF, respectively. At week 14, ACR20 response was achieved by 35% patients on 50 mg GLM (P = 0.0006), and 38% patients on 100 mg golimumab (P = 0.0001) compared to 18% patients on placebo. 8 Therefore, GLM reduced the signs and symptoms of RA in patients who had previously had anti-TNF therapy. No significant differences were observed in serious adverse events after 24 weeks of treatment.
GO-BEFORE study demonstrated that efficacy of GLM plus MTX in MTX naïve patients as first-line therapy for early-onset RA is better than MTX alone in reducing RA signs and symptoms, with no unexpected safety concerns. However, there were no differences when both treatments were administrated in monotherapy. 9
For treatment of RA, the approved dosage of GLM is a 50 mg subcutaneous injection, given once a month. Less than 6% of patients included in all studies notified injection site reaction. Serious adverse events occurred 4%–10% of patients in placebo groups and 3%–7% in GLM groups. Nowadays, GLM exhibits a favorable safety profile, which is quite similar to the other commercialized anti-TNF-α, although long-term studies are needed to confirm these results.
Certolizumab pegol
Certolizumab pegol (CZP) is a humanized and the first pegilated TNF antagonist molecule. It means that antibody Fab fragment is conjugated to a polyethylene glycol (PEG), which increases the plasma half-life of the drug. The chemical structure of CZP is distinctly different from other anti-TNF monoclonal antibodies approved for use in RA. It does not have an Fc receptor and, therefore, does not activate complement or antibody dependent cytotoxicity and avoid apoptosis. It targets TNF-α with a different mechanism of action than widely used biologics. A new study has shown that CZP does not appear to be actively transferred across the placenta in the third trimester of pregnancy. 10 Three different phase III studies with CZP have evaluated its efficacy and safety in RA.
RAPID 1 and RAPID 2 studies included RA patients with active disease despite treatment with MTX. Their results showed that CZP plus MTX significantly improved signs and symptoms more frequently than MTX plus placebo, and clinical benefits were achieved rapidly, as early as one week of treatment. 11 Same results were observed for improving physical function and inhibiting radiographic progression. 12 There were no differences in clinical efficacy between the two CZP doses, suggesting that a 200 mg dose every two weeks is optimal for treatment.
The FAST4WARD study evaluated the efficacy and safety of certolizumab pegol 400 mg every four weeks as monotherapy in patients with active RA with no response to previous disease modifying antirheumatic drugs (DMARDs). CZP effectively reduced the signs and symptoms in these patients, and most adverse events observed were mild or moderate, with no deaths reported. 13
Safety profile was similar to other TNF antagonists. Based on published data, there seems to be no significant difference among the available anti-TNF therapies in terms of efficacy and safety.
CZP and GLM have shown promising efficacy benefits as first-line biologic therapy for patients with active disease despite treatment with MTX and/ or other TNF antagonists, or both. Another pegilated anti-TNF is being developed: pegsunercept.
Subcutaneous abatacept
Abatacept is a soluble fusion protein that consists of the extracellular domain of human cytotoxic T-lymphocyte-associated antigen 4 (CTLA-4) linked to the modified Fc portion of human immunoglobulin G1. It is the only agent currently approved to treat RA that targets the co-stimulatory signal required for full T-cell activation. Results of subcutaneous abatacept for the treatment of RA were presented in the EULAR Congress in 2010. ACR20 response after 16 weeks of treatment with 125 mg weekly of abatacept plus MTX and abatacept mono-therapy was achieved by 55% and 44% of patients, respectively. 14 The efficacy and safety results in RA patients of subcutaneous abatacept are consistent with the experience of intravenous administration.
Subcutaneous anti-IL6
IL-6 signaling can be inhibited by suppressors of cytokine signaling, such as antibodies directed against IL-6R. Tocilizumab is the only commercialized IL-6 antagonist for RA. It competitively inhibits the binding of soluble and membrane IL-6 to its receptor, which prevents IL-6 signal transduction to inflammatory mediators that summon B and T cells. Two new subcutaneous anti-IL6 monoclonal antibodies, including tocilizumab, have been developed and are being tested in trials.
Anti-CD20
The CD20 is a small molecule with small and big extracellular loops. Anti-CD20 molecules can reduce B cells by different mechanism of action: binding to the extracellular domain of antigen CD20, activating the complement and leading to cell lisis (CDC); union by means of the Fc of the antibody to the receptor adapted in the cytotoxic cells (ADCC); alteration of B cells stability; or stimulating apoptosis. Nowadays, the only anti-CD20 treatment approved for the RA treatment is rituximab. The efficacy of rituximab monotherapy in RA is limited, potentially in part because of reduced cell lysis via CDC in this setting. New anti-CD20 have been developed and their efficacy and safety profile are still being tested in different clinical trials.
Ocrelizumab
Ocrelizumab is a humanized anti-CD20 monoclonal antibody. It differs from rituximab in the positions of the determinant regions for the complement of the light and heavy chains. It was demonstrated to produce less CDC and more ADCC in vitro compared to rituximab; therefore, it is expected to produce less severe reaction to the infusion and less immunogenicity. The ACTION trial 15 was a combined phase I/II study which evaluated efficacy and safety of intravenous placebo plus MTX versus ocrelizumab (day 1 and 15 and 10–1,000 mg per each infusion) plus MTX in RA patients who had no response to previous MTX therapy. All doses evaluated were associated to clinical activity. Peripheral B cell depletion after infusion was rapid at all doses, with earlier repletion of B cells at doses of 10 mg and 50 mg. The incidence of serious adverse events and serious infections in the ocrelizumab plus MTX group was 17.9% and 2.0%, respectively, compared with 14.6% and 4.9%, respectively, in the placebo plus MTX group. Another phase III trial (SCRIPT) 16 evaluated the efficacy and safety of two doses of ocrelizumab (2 × 200 mg, 2 × 500 mg) versus placebo in patients with active RA despite treatment with at least one anti-TNF therapy. Both ocrelizumab doses had demonstrated to be clinically efficacious, but only the 500 mg dose decreased the radiological progression. Safety regarding adverse events and serious adverse events was similar in the three groups.
Ofatumumab
Ofatumumab is a human monoclonal antibody that targets an epitope encompassing the membrane-proximal small-loop on the CD20 molecule, while the binding location of rituximab and ocrelizumab is located in the large loop. 17 Ofatumumab efficacy and safety were investigated in a phase I/II trial which compared three doses of ofatumumab versus placebo in RA patients who did not respond to at least one DMARDs. ACR20 response rates were achieved significantly more frequently in all ofatumumab groups (40%, 49%, and 44% for the 300 mg, 700 mg, and 1,000 mg doses, respectively) than did patients with placebo (11%), (P < 0.001). Overall, a moderate or good response was reached by 70% of patients receiving ofatumumab. Serious adverse events were predominantly reported at the first infusion, and mostly had mild to moderate intensity. Rapid and sustained peripheral B cell depletion was observed in all doses groups. 18 Two phase three studies are being conducted to further measure the efficacy and safety of ofatumumab in RA patients who have had inadequate response to either methotrexate or TNFα antagonist therapy. Ofatumumab is also being developed for subcutaneous administration.
SMIP
Small molecular inmunopharmaceutical proteins are smaller molecules than the standard monoclonal antibodies, so they are expected to have better tissue penetration, efficiency and safety spectrum. Two CD20 SMIP against CD20 antigens of the B cells have been developed (TRU-015, SBI-087). Results of an open label of a phase 2b trial showed sustained efficacy and safety with continued retreatments of TRU-015 (a single 800 mg infusion at 24 weeks interval) in RA patients. 19 ACR 20, 50 and 70 response achieved rates after first retreatment were 70%, 40% and 23%, respectively. No subject experienced a serious adverse event on the day of infusion. SBI-087 is being developed for subcutaneous administration.
New Molecules against New Targets
Anti-IL15
IL-2, IL-4, IL-7, IL-9 and IL-21 share an identical receptor subunit with IL-15, and therefore, some functions of IL-15. There are no studies of these citokynes as therapeutic targets. Two monoclonal antibodies against IL-15 (one human and another one humanized) have been developed, with favorable results for only one of them (Humax-IL15).
Anti-IL17
Recently, besides the Th1 and Th2 CD4+ cells CD4, Th17 cells have been described. These produce not only IL-17, but also IL-21 and IL-22, and seem to be responsible for the autoimmune inflammation. Nevertheless, IL-17 is also produced by Natural Killer cells, T CD8+ lymphocytes and granulocytes. IL-17 plays an important role in adaptative immunity, differentiation and maturation of neutrophils, and increases the production of other citokynes (IL-1, IL-6 or TNFalpha) and regulates osteoclasts formation. The synovial tissue in AR patients produces biological active IL-17, in addition to IL-1, IL-6 and TNF, while in CN IL-17 is undetectable in peripheral blood. Therefore, IL-17 could be a novel cytokine target.
There are at least three new monoclonal antibodies against IL-17: LY2439821 (humanized, intravenous), AIN457 (human, intravenous) and AMG817 (human, subcutaneous). An early phase clinical study 20 investigated the safety, tolerability and efficacy after the intravenous administration of three doses of LY2439821 (0.2, 0.6 and 2.0 mg/kg) compared with placebo in patients with RA who did not respond to at least one DMARD. ACR20 response was achieved by 74%, 70%, 90% and 57%, respectively. There was one reported serious adverse event, classified as unrelated to study drug, and no deaths, and LY was well tolerated. Therefore, the results of this study are promising for IL-17 as a new target in RA.
Anti-M-CSF
The monocyte/macrophage colony stimulating factor is part of a natural immune and inflammatory cascade, but it also has been identified as an inflammatory mediator in autoimmune diseases such as RA, leading to an increase of proteases and proinflammatories cytokines production which produces joint destruction. PD-0360324 is a novel human monoclonal antibody against M-CSF. A single intravenous infusion of escalating dose was administered to healthy volunteers, and it was well tolerated. 21
Anti-oncostatin
Oncostatin M (OSM) is a member of IL-6 family, presented in synovial membrane and blood of RA patients, that is thought to drive pro-inflammatory responses and to produce acute phase reactants, all associated to cartilage degradation. GSK315234 is a new intravenous monoclonal antibody against OSM and shows to be safe and well tolerated in healthy volunteers. 22
Monoclonal antibodies against other targets, such as IL-22, IL-12/IL-23 and RANKL, approved for the treatment of other inflammatory or rheumatic diseases, could be efficacious in RA patients, but specific studies are needed to prove it.
Small Molecules
Small molecules are those with a molecular weight inferior to 1 Kilodalton. These agents are available for oral administration, and they could have same efficacy than current biological therapies, with a minor risk of adverse events and less expensive. These molecules act on several receptors, routes of intracellular signaling and enzymes, important in the RA pathogenesis. Understanding the intracellular targets that regulate cytokines in RA can potentially lead to new therapeutic options. After stimulation of innate immunity or exposure to pro-inflammatory cytokines, a number of subsequent enzymes phosphorylations take place within the cell cytoplasm, and this process usually permits the migration of NF-κB to the nucleus, where it is activated and responsible for the regulation genes that contribute to inflammation, including TNF-a, IL-6, IL-8 and cyclooxygenase-2 (COX-2). A great number of trials are evaluating the efficacy and safety of small molecules against different target. They are usually classified as follow:
Cytokines and chemokines antagonists
Cellular surface markers inhibitors
Intracellular signal inhibitors
Cytokines and Chemokines Antagonists
IL-12/IL-23
Monoclonal antagonist against IL12/IL23 (ustekinumab) is efficacious for some inflammatory diseases (psoriasis) and is being tested for RA. A small molecule against this target (Apilimod mesylate) is being investigated in RA (a phase II trial) and Crohn disease.
CCR5 inhibitor
The presence of a nonfunctional receptor of the CCR-5 gene has been associated with a reduced incidence and severity of RA. Maraviroc is a CCR-5 antagonist. A phase II study 23 did not observe disease improvement in RA patients after 12 weeks of treatment with this drug, and maraviroc was safe and well tolerated in this study.
CXCL-10 inhibitor
CXCL10 is a chemokine that acts by binding to the cell surface receptor CXCR3, and promotes directed migration of activated T cells and monocytes. Both CXCL10 and CXCR3 are widely expressed in RA synovium; therefore they may play a role in disease pathogenesis. MDX-1100 is a fully human monoclonal antibody which neutralizes CXCL10. A phase II study 24 evaluated the efficacy and safety of repeated doses of MDX-1100 in RA patients on stable doses of MTX. Disease response (ACR20 54% in MDX-1100 group versus 17% in placebo group) was seen 85 days receiving intravenous 10 mg/kg of MDX-110 or placebo every other week. Results also observed good drug tolerance.
Intracellular Signal Inhibitors
Tirosin-kinase
JAK kinase inhibitor (Tasocitinib, CP-690,550) Cytokine receptors are formed by two chains composed by an extracelular and an intracelular portion, each one joins to a kinase-family member named JAK kinase, which is usually inactivated. In the absence of cytokines, both chains are separated, but the cytokinereceptor union produces JAK kinase phosphorilation. Following this process, transduction or transcription signals named STAT molecules get together and phosphorilate, so they can migrate to the nucleus and directly activate transcription.
JAK-3 plays an essential role for signal transduction of different interleukins (IL-2, IL-4, IL-7, IL-9, IL-15, and IL-21) necessary after their union to the receptor. Different studies have demonstrated that JAK-3–knockout mice have defects in T lymphocytes, B lymphocytes, and natural killer (NK) cells, with no other defects reported. Therefore, the JAK3 kinase may serve as a useful target for RA.
Tasocitinib is an oral, selective, JAK antagonist. A phase II trial evaluated the safety and efficacy of this new drug in patients with active RA. 25 They received three different dosages (5 mg, 15 mg and 30 mg) of tasocitinib or placebo twice daily for six weeks. At the end of the study, the ACR20 response rates were 70.5%, 81.2%, 76.8%, and 29.2% respectively, (P < 0.001), and by week four, ACR50 and ACR70 response rates significantly improved in all treatment groups. The most common adverse events reported were headache and nausea. No opportunistic infections or deaths occurred. The incidences of adverse events in the 5 mg twice daily and placebo groups were similar, but there were dose-related increases in the number of patients reporting treatment-emergent AEs in the tasocitinib 15 mg and 30 mg twice daily groups. The infection rate in both groups was 30.4% (versus 26.2% in the placebo group).
New drugs against JAK-1 and JAK-2 are also being developed to treat patients with AR.
SyK (spleen tyrosine kinase) inhibitor (Fostamatinib disodium)
Spleen tyrosine kinase (Syk) is an important mediator of immunoreceptor signaling in different cells, including mast cells, macrophages, neutrophils, and B cells, and it is important in TNF–induced cytokine and metalloproteinase production. Increased levels of phosphorylated Syk are detected in RA synovial tissue as compared to tissue from patients with osteoarthritis. Fostamatinib disodium (FosD) is a prodrug that, following oral administration, is rapidly converted to R406, which is a potent inhibitor of Syk kinase.
A double-blinded, placebo-controlled trial26,27 evaluated the efficacy and safety of FosD in RA patients with active disease despite methotrexate therapy. At week 12, ACR20 response was achieved by 65% and 72% of 100 mg and 150 mg twice-daily groups, compared with 32% and 38% in the twice-daily doses of 50 mg and placebo respectively (P < 0.01). ACR50 and ACR70 response rates were also more frequent in these groups. During the 12-week study, there was a similar proportion of patients who experienced at least one adverse event in the placebo group and the FosD 50 mg, 100 mg, and 150 mg groups. The two most common adverse events were diarrhea and neutropenia. Diarrhea occurred in 6 (13%), 5 (11%), 8 (16%), and 21 (45%) of the patients in the placebo and FosD 50 mg, 100 mg, and 150 mg groups respectively. Neutropenia occurred overall in 15% of the patients treated with FosD compared with none of the patients in the placebo group.
MAP (mitogen activated protein)-kinase
The MAP kinases are also key regulators of cytokine production and can be possible targets for the RA treatment. There are three different MAP-kinase families: extracellular signal regulated kinase-ERK, c-Jun N-terminal kinase-JNK and p38 kinase. All of them are expressed in rheumatoid synovial tissue. Therefore, they are potential therapeutic targets for this disease.
P38-MAP kinase inhibitor
P38 MAP-kinase plays a key role in RA, including TNFα, IL1β and COX2 signaling regulation. More than 20 different p38 inhibitors have been tested in RA. 28 VX-702 was evaluated in two phase II trials including patients on monotherapy or combined with MTX, and modest response was noted with the group treated daily in both of them. Pamapimod is another p38α inhibitor. A phase II trial in RA patients failing metothrexate did not observe higher efficacy with three doses of pamapimod (25 mg, 50 mg and 150 mg twice daily) compared with placebo. Serious adverse events were reported in 4%–6% of pamapimod group and 2% of placebo group. Unfortunaltely, p38 inhibitors have limited efficacy and there was a number of trials that evaluated their efficacy and safety with unfavourable outcome.
JNK (janus tyrosine kinase)
Syk is expressed and activated in RA synovium and serves as a key regulator in TNFα-induced IL-6 and MMP-3 production in RA fibroblast-like synoviocytes. The mechanism of action for cytokine and MMP suppression probably involves the MAPK cascade, especially JNK. Of the JNK isoforms, JNK2 is particularly important in arthritis because it is the dominant isoform expressed in synoviocytes. SP600125 is a selective JNK inhibitor and has demonstrated striking protection against bone and cartilage destruction 29 in synovial tissue samples obtained from patients with osteoarthritis and RA at the time of joint replacement.
Transcription factors inhibitors NF-κB (nuclear factor κB)
Activation of NF-κB is essential in regulating osteoclast formation. This process is enhanced by proinflammatory cytokines such as TNF-α and IL-6. Targeting NF-κB is an effective therapeutic strategy in many animal models of arthritis. Intraarticular administration of a NBD peptide has been associated to the inhibition of NF-κB regulatory activity. Another molecule, IKK-2 is essential for NF-κB signal regulation and an antagonist against it is being developed.
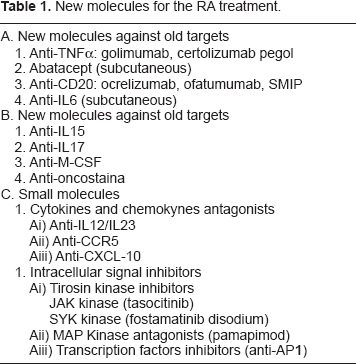
New molecules for the RA treatment.
NFAT (nuclear factor activation of T cells) AP-1 (activator protein)
Factor activator protein-1 (AP-1) regulates many genes that participate in RA. Its compounds, c-Jun and c-Fos, are frequent in RA synovium, and high levels of AP-1 are detected in RA synovial tissue compared to osteoarthritis. AP-1 decoy oligonucleotides suppress collagen-induced arthritis and inhibit IL-1, IL-6, TNF-a, matrix metalloproteinase (MMP)-3 and MMP-9 production by synovial tissue.
Conclusions
RA remains a major challenge. However, remission or response is not achieved in all patients. Therefore, new drugs seem necessary. This paper reviews newer therapeutics options that may offer an opportunity to these patients. Fortunately, the increasing knowledge of the mechanisms of the disease and the discovery of signaling pathways or molecules mediating the inflammatory process have lead to additional researches focusing on improving the available therapies or the development of new ones targeting different molecules.
Two new TNF inhibitors, golimumab and certolizumab pegol, in addition to demonstrating an acceptable safety and tolerability profile, have shown promising efficacy benefits as first-line biologic therapy for patients experiencing an inadequate response to MTX or TNF inhibitors. A number of anti-CD20 molecules (ofatumumab, ocrelizumab and SMIP) are under development or are already on the market. Data from a number of clinical studies suggest that they are safe and efficacious in RA.
Subcutaneous abatacept and anti-IL6 are under scrutiny, but available data suggests they could have similar results than intravenous administration. Safety and efficacy of new monoclonal antibodies against IL-12, IL-17, IL-20 and IL-23 are being tested in a large number of trials. Small molecules directed against intracellular signals involved in the transcription process are promising, mainly tasocitinib and fostamatinib disodium, have demonstrated a good efficacy and safety profile, and are promising treatments for RA. However, more studies are necessary.
Disclosures
This manuscript has been read and approved by all authors. This paper is unique and not under consideration by any other publication and has not been published elsewhere. The authors and peer reviewers report no conflicts of interest. The authors confirm that they have permission to reproduce any copyrighted material.
Dr. Federico Navarro Sarabia has received grants from Abbott, Bristol Myers Squibb, MSD, Pfizer, Schering Plough, Tedec Meiji, UCB, Wyeth.