
Abstract
Morphine or other strong opioids (fentanyl, oxycodone, hydromorphone, buprenorphine) are usually administered in patients with severe cancer and chronic non-malignant pain. However, when these analgesics are ineffective in terms of analgesia or induce intractable adverse effects, a switch to methadone might prove beneficial. Consequently methadone is used in opioid rotation (switch) when other opioids have failed. Methadone may be considered as the first strong opioid, especially in patients with neuropathic pain and renal failure. Still, methadone dosing is more difficult than dosing of other strong opioids due to unpredictable pharmacokinetics, numerous drug interactions and a possibility of QTc interval prolongation. Preferably, methadone should be prescribed by physicians experienced in cancer and chronic pain management. The knowledge on methadone cardiotoxicity among health care professionals is limited. The aim of this article is to outline methadone drug interactions and adverse effects with focus on the QTc interval prolongation. Several recommendations grounded in the literature review are provided to clinicians who use methadone in pain management.
Introduction
Methadone (Hoechst 10820) was synthesized in 1938 in Germany and it is available in the form of oral and rectal formulations as well as ampoules for parenteral administration. In clinical practice, methadone is administered mostly in patients with cancer pain who undergo opioid rotation (OR) when analgesia becomes ineffective and intractable adverse effects occur: neurotoxicity (drowsiness, confusion, hyperalgesia, myoclonus) and gastrointestinal symptoms (nausea and vomiting, constipation). 1 Due to lack of active metabolites methadone may be used in patients in pain and delirium. Methadone may also be the first strong opioid to be administered in patients who have been already treated with opioids for moderate pain (tramadol, codeine, dihydrocodeine) or in opioid-naive patients. Methadone may be safely administered in patients with renal impairment and or cancer-related neuropathic pain. Methadone is 10-fold less expensive than controlled release morphine, 25-fold cheaper than TF and it is particularly useful in patients requiring high opioid doses. Apart from pain management methadone is commonly used in the treatment of opiate dependence. 2
Methadone Interactions
Methadone is metabolized through P-450 enzymes, mainly CYP3A4 but to a lesser extent CYP2D6, CYP2B6 and CYP1A2. Methadone interacts significantly with drugs that cause hypoactivity or hyperactivity of these enzymes, especially CYP3A4. Differences in CYP3 A4 activity (30-fold in liver and 11-fold in gut), in CYP3A4 mRNA amount (50-fold) in the liver and CYP2D6 polymorphism also play an important role in large individual variations associated with methadone pharmacokinetics. Methadone drug interactions mediated via CYP2C9 and CYP2C19 enzymes alone seems to be not significant. 3
Antifungal azole drugs, SSRIs, macrolids and chinolones, diazepam, cimetidine, calcium channel blockers, desipramine, dihydroergotamine, grapefruit juice and single alcohol consumption inhibit metabolism, consequently causing a rise in methadone level and intensifying adverse effects. Among azole antifungals ketoconazole, fluconazole and itraconazole are potent CYP3A4 inhibitors and with methadone may lead to QTc prolongation or respiratory depression. From SSRIs group fluvoxamine, fluoxetine and paroxetine display very significant (CYP3A4 and CYP2D6 inhibition) while sertraline and citalopram seems to have a small potential for methadone interaction. An interaction between venlafaxine (substrate and mild CYP2D6 inhibitor) and methadone has not been studied so far; close monitoring is advised. Chinolones inhibit CYP3A4 and CYP1A2, macrolides are potent CYP3A4 inhibitors both prolong QTc interval; cotrimoxazole (sulfamethoxazole and trimethoprim) prolong QTc interval, sulfamethoxazole is CYP2C9 inhibitor; caution is advised in combining methadone with these agents. 4
Anticonvulsants, tuberculostatics, antiretrovirals, high corticosteroid doses, risperidone, fusidic acid, spironolactone, St. John's Wort, regular alcohol consumption (through inducing CYP3A4) and smoking cigarettes (CYP1A2 inducer) speed up methadone metabolism, reduce analgesia and may cause withdrawal. On the other hand a withdrawal from CYP3A4 inducers (carbamazepine, rifampicin and high corticosteroids doses) administration may lead to methadone toxicity. 5
Pharmacodynamic interaction between methadone and benzodiazepines may appear. Because of the possible pharmacokinetic interaction with diazepam (CYP3A4 inhibition), midazolam, alprazolam and triazolam (CYP3A4 substrates), drugs that do not undergo phase I metabolism may be preferred (buspirone, lorazepam, oxazepam, temazepam) if there is a need for methadone combination with benzodiazepines. 6
Caution and careful monitoring is recommended when combining methadone with tricyclic antidepressants (amitryptyline and trazodone) because it increases the risk of QTc interval prolongation. Methadone is CYP2D6 inhibitor and it may cause rise in drug levels metabolized by this enzyme e.g. SSRIs, tricyclics, venlafaxine, mianserine, neuroleptics (risperidone, haloperidol, chlorpromazine), β-blockers and opioids (dextromethorphan, tramadol, codeine and dihydrocodeine). Drugs that are CYP3A4 substrates may be affected by methadone administration and vice versa. Methadone therapy with monoamine oxidase (MAO) inhibitors should be avoided as it can produce serotonin syndrome. A combination of antiarrhythmics (quinidine and lidocaine are substrates and amiodarone CYP3A4 inhibitor, quinidine is a strong CYP2D6 inhibitor), which prolong QTc interval and may cause ventricular arrhythmia with methadone if possible should be also avoided. 4
Generally it is advisable to avoid agents metabolized through CYP3A4 especially CYP3A4 inhibitors and inducers, possibly limit CYP2D6 inhibitors and substrates during methadone therapy. Special attention should be paid on older patients who are particularly vulnerable to drug interactions due to coexisting chronic diseases requiring pharmacotherapy and age-related decline in P-450 activity 7
QTc Interval Prolongation
QTc interval prolongation is generally defined as over 450 ms, although in women it may be defined as over 470 ms and in men over 430 ms. A QTc prolongation over 500 ms is an accepted threshold for significant arrhythmia risk. 8 It is associated with a 4-fold increase in syncope or sudden death, presumably from torsades de pointes (TdP), in patients with congenital long QT syndrome. 9 QTc interval screening is the current standard for assessing drug safety.
The most common mechanism of drug-induced QTc prolongation and TdP is a blockade of the human cardiac ether à go-go-related gene (hERG) which encodes Ikr–-the delayed-rectifier potassium ion channel. Blockade of this cardiac ion channel prolongs the terminal portion of the cardiac action potential and causes delayed repolarization, which manifests as QTc interval prolongation on the surface ECG. Methadone is a potent inhibitor of the hERG channel, achieving 50% in vitro inhibitory concentration of Ikr at approximately 1 to 10 μM. 10 Apart from blockade of hERG channels, methadone may predispose to TdP by inducing bradycardia through calcium-channel antagonism and anticholinesterase properties. 11
In several studies ventricular arrhythmia was observed during methadone administration, especially in patients treated with high doses of the drug. Three patients treated with high oral dose of methadone (over 600 mg daily) were diagnosed with ventricular arrhythmia presumably evoked by drug interaction with CYP3 A4. Two patients had been earlier diagnosed with cardiac muscle damage. Authors of the study recommend careful observation of patients treated with high doses of methadone (over 600 mg daily) especially when it is administered together with other drugs interacting with CYP3A4. Similar precautions need to be taken with respect to patients with ventricular arrhythmia history. 12
Ventricular arrhythmia was observed in 17 patients treated for pain or addiction, with the mean daily doses of 400 mg. Among possible reasons, other drugs, cardiac diseases, drug interactions with methadone, hypo potassium in blood serum, and bradycardia are listed. 13 Another study found that QTc interval was prolonged in patients treated with intravenous methadone as compared to patients treated with intravenous morphine. 14
Cruciani et al reviewed 104 patients receiving oral methadone as treatment for chronic pain or addiction. The median daily dose was 110 mg (range 20–1200 mg) and the median time of methadone treatment was 12.5 months (range 1–144 months). QTc prolongation occurred in 33% of patients but it was not longer than 500 msec. Although methadone prolonged QT interval, there was little risk of serious prolongation. 15
Chug et al found that in the group of patients who died due to sudden cardiac death and used methadone for therapeutic reasons (blood level < 1 mg/L) cardiac abnormalities were found in 23% of patients in contrast to 60% (p = 0.002) of patients not treated with methadone. 16
Recommendations for Increasing the Safety of Methadone Use in pain Management
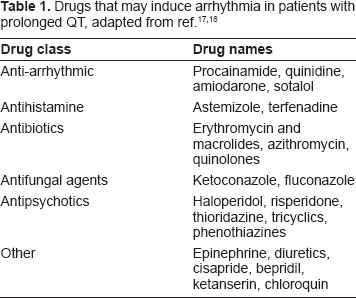
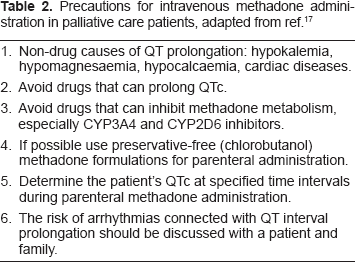
Several studies addressed the problem of increasing methadone treatment safety with regard to possible ventricular arrhythmia. Recommendations in this respect are based on recent reviews.17–20 Concomitant administration of drugs which may increase the risk of TdP should be avoided (Table 1). The risk of arrhythmia should be carefully assessed and discussed with the patient and family when starting parenteral treatment with methadone in patients with possible QT prolongation (Table 2). 21
Precautions for intravenous methadone administration in palliative care patients, adapted from ref. 17
Generally, it seems that the introduction of the ECG monitoring program may improve safety of methadone analgesic therapy although no formal studies on this matter have been carried out to date. The standard 12-lead ECG should be used as there is a risk that QTc prolongation might be overlooked when using single- or three-lead ECG. The QT interval is dependent on the heart rate and therefore it needs to be corrected. To this end, Bazett's formula can be used: QTc = QT interval in ms divided by the square root of the preceding RR interval in seconds. 22 ECG may be performed about 3–4 h after methadone ingestion because at this time methadone reaches peak plasma concentration. A manual or automated interpretation of QTc interval may be used. ECG may be performed at baseline (before starting oral or parenteral methadone treatment), after 4–7 days (when methadone plasma steady state is achieved) and 4–7 days after each dose increment. ECG may also be performed in the case of the change in patient's clinical condition such as occurrence of seizures or syncope. ECG should be also considered when other QT prolongation risk factors emerge such as electrolyte imbalance, drugs that may influence methadone metabolism (e.g. CYP3A4 inhibitors or discontinuation of CYP3A4 inducers). 23 The dose should not determine ECG as there is no consensus what dose or what dose increments are connected with higher risk or arrhythmia. Serum electrolytes level should be controlled on an individual basis.
Methadone dosing should take into account its plasma half life and duration of analgesia. Unfortunately they may be quite different; in spite of long and changeable plasma half life (over 20 h) analgesia persists for approximately 6–12 h. The regular dosing of oral methadone every 8 h seems to be the best possible approach. 24 The starting dose depends if the patient is opioid naive or opioid tolerant; in the former the dose 3 mg t.i.d. may be recommended, in the latter the dose depends on the amount of previous opioid consumption; when weak opioids failed the starting dose may be 5 mg t.i.d. With parenteral methadone the oral dose is halved and then usually administered in subcutaneous or intravenous infusion. The meticulous clinical evaluation of the individual patient in terms of pain, adverse effects, co morbidities and general condition is mandatory and adjusting methadone dose accordingly. 25
Before starting methadone therapy a detailed history on heart diseases should be taken. The patient and his/her family should be informed of a possible risk of QT prolongation and its clinical consequences. If QT interval exceeds 500 ms it is potentially dangerous even if no symptoms are observed. A change from methadone to another opioid (e.g. morphine, buprenorphine) which is safer with this respect seems to be the best approach. 26 Methadone dose reduction may be also considered with discontinuation of drugs that may prolong QT interval. 19 An independent panel developed cardiac safety recommendations for physicians prescribing methadone:
Disclosure: Clinicians should inform patients of arrhythmia risk when they prescribe methadone.
Clinical History: Clinicians should ask patients about any history of structural heart disease, arrhythmia or syncope.
Screening: Obtain a pre-treatment ECG for all patients to measure the QTc interval and a follow-up ECG within 30 days and annually. Additional ECG is recommended if the methadone dosage exceeds 100 mg per day or if patients have unexplained syncope or seizures.
Risk Stratification: If the QTc interval is greater than 450 ms but less than 500 ms, discuss potential risks and benefits with patients and monitor them more frequently. If the QTc interval exceeds 500 ms, consider discontinuing or reducing the methadone dose; eliminating contributing factors, such as drugs that promote hypokalemia; or using an alternative therapy.
Drug Interactions: Clinicians should be aware of interactions between methadone and other drugs that possess QT interval-prolonging properties or slow the elimination of methadone. 13
Cruciani recommends caution and ECG testing in patients who are or will be treated with drugs that are substrates of the CYP3A4/CYP2D6 and drugs that have the potential to block rapid rectifying channel currents or in patients who are medically frail and have other risk factors for QTc prolongation (e.g. hypokalemia). Patients started on methadone during hospitalization should get a baseline ECG test, which should be repeated after dose escalation and when drugs that can increase the risk of arrhythmia are added. The lowest methadone dose at which ECG should be performed was not clearly established. 21
Conclusions
Although methadone therapy may be associated with prolonged QTc interval, several precautions presented may decrease the risk of TdP. ECG monitoring and avoiding factors that increase the risk of QTc prolongation may help decrease the methadone cardiotoxicity. Before administering methadone to patients with a possible QTc prolongation, the risk of arrhythmia should be carefully assessed. In patients with significant QTc prolongation (over 500 ms) while on methadone the use of different opioid analgesics should be considered.
Disclosure
This manuscript has been read and approved by the author. This paper is unique and is not under consideration by any other publication and has not been published elsewhere. The author reports no conflicts of interest.