
Abstract
Paget's disease of bone (PDB) is a condition characterized by excessive and abnormal bone remodelling. Due to a high rate of bone remodelling, bisphosphonates, and especially pamidronate and the newer zolendronate, are indicated in the treatment of PDB. The presence of asymptomatic, but active PDB represents an indication for treatment aimed at preventing later complications. An additional indication for treatment is the involvement of skeletal segments that may give rise to severe complications. Pamidronate has a long history in the treatment of PDB. The more utilised regimen is 3 to 6 i.v. infusion of 60 mg of pamidronate at an infusion rate of 1 mg/min within 3-21 days. Zolendronate (5 mg once yearly) is the most powerful amino-bisphosphonate currently used. This primacy recognizes both the ability to inhibit the farnesyl-pyrophosphate synthetase and the higher affinity to hydroxyapatite crystals as a cause. Both pamidronate and zolendronate are effective in PDB, with an evidence-based superiority of the latter.
Introduction
Paget's disease of bone (PDB) is a condition fully described for the first time by Sir James Paget in 1877 characterised by excessive and abnormal bone remodelling. PDB is usually localized on one or several skeletal segments without significant clinical findings, but it may also be widespread and severe, leading to severe osseous deformity and pain.1,2
The disease seldom appears before the age of 40, but its prevalence tends to double each decade from the age of 50 onwards. Besides, 15% to 40% of people affected by PDB have a positive family history of the disease.3,4
Currently, the causes of PDB remain unclear, but growing evidence indicates both genetic and environmental influences. 5 Paget's osteoclasts seem to produce higher level of interleukin-6 receptors than normal osteoclasts and this appears to initiate an autocrine-paracrine loop enhancing osteoclast formation and increasing the osteoclast precursor pool. After this initial intensive wave of osteoclast activity, an osteoblastic response leads to an aberrant bone tissue resembling woven bone with increased vascularity and a pronounced connective tissue reaction. The combination of osteoclastic and osteoblastic activities account for marked elevation of osseous turnover rate. 6
In about 70% of the cases, PDB is asymptomatic. 2 Typically, the disease may be monostotic or polyostotic, in the latter case producing a richer clinical picture.7,8 Affected bones are involved right away with no new involvements during the evolution. PDB may virtually affect every bone in the skeleton, but the sites more often implicated are the pelvis and sacrum (>60%), the spine (50%), thigh bones and skull (40%), tibias, humeri and clavicles (20%). Hands, feet and facial bones are rarely affected.7,9
Pain is most often associated with bone deformities; besides, pagetic bone is brittle and may fracture even spontaneously. In long bones, deformities may induce secondary osteoarthritis, while in facial bones deformities may create difficulties for artificial dentures and tooth extraction. 2 Neurologic complications may result from skull involvement and the most frequent are hearing loss and cranial nerve palsies. Spine involvement may also cause radiculopathies. Due to the hyper-vascularisation of pagetic bone, skull involvement may divert blood from external carotid artery system at the expense of brain circle, accounting for tortuosity of the superficial branch of temporal artery.2,7
The most feared complication of PDB is malignant degeneration, which occurs in about 0.2% of the cases, although the overall risk of osteosarcoma in pagetic patients is 30 times greater than in general population. 10 Interestingly, the preferred localizations of malignant degeneration do not correspond to the preferential locations of the affected bones; in clinical practice, osteosarcoma has to be suspected in any long-standing disease with worsening bone pain, a sudden fracture or with the involvement of a new skeletal segment. In some cases, the detection of a new mass in soft tissue around the bone or a sudden, painful fracture would raise concern about malignancy. 11
In PDB biochemical measurement of bone turnover provides an objective assessment of both disease activity and the response to treatment. The main biologic characteristic is the elevation of total alkaline phosphatase (AP), that usually reflects the spreading of osseous involvement, especially in polyostotic forms of the disease.12,13 As far as the significant difference in the biologic markers is concerned, the importance of establishing biological variations in active disease rather than extrapolating it from unaffected people has been recently demonstrated. In particular, in normal subjects a change in AP of 15% is needed to exceed the critical difference, while in PDB patients a 30% difference is required. 14 In the evaluation of monostotic PDB, instead, bone AP seems to be the most sensitive biologic marker, even in those patients in which total AP results normal despite an active disease. 15
Bisphosphonates and Paget's Disease
Due to a high rate of bone remodelling, bisphosphonates, especially pamidronate and the newer zoledronic acid, are indicated in the treatment of PDB. The presence of asymptomatic, but active PDB (elevated AP), represents an indication for treatment aimed at preventing later complications. Other Authors do not confirm such use because the possibility of deformity still exists when disease activity is suppressed. 16 An additional indication for treatment is the involvement of skeletal segments that may give rise to severe complications. These are weight-bearing bones near major joints and the skull; in this setting the treatment is warranted especially in younger patients. However, even in the elderly, the pharmacological treatment is justified when bones involved are close to joints (i.e. knees) or nerve roots. Treatment is also indicated in subjects with normal AP but with focal symptoms. 2
PDB was an untreatable condition until the mid 1970s, when calcitonin was registered for the treatment of the disease. However, both salmon and human calcitonin have demonstrated to be ineffective in reducing bone turnover in most cases; moreover, its parenteral administration is associated with unpleasant side effects. In the early 1980s the bisphosphonate etidronate was introduced, but this had to be used at sub-optimal doses because of the development of osteomalacic features. The current pivotal drugs for the treatment of PDB are second-generation bisphosphonates, which strongly inhibit bone resorption. The greater advantage of these drugs relies in prolonged remissions and in the healing of the resorption front.17,18 In many patients the complications of PDB require additional symptomatic treatment, including analgesics and selected orthopaedic and neurosurgical interventions.
In this concise review we focus on the treatment of PDB with pamidronate and zoledronic acid.
Pamidronate has a long history in the treatment of PDB, but in some countries it has been registered only for the treatment of malignant hypercalcemia and thus it is still used off label in pagetic patients. Pamidronate was initially used in oral formulation, but it resulted in being poorly tolerated.19,20 Thus several intravenous (i.v.) dosing regimens have been proposed.21–30 The more utilized regimen is 3 to 6 i.v. infusion of 60 mg of pamidronate (Aredia®) at an infusion rate of 1 mg/min within 3-21 days. This dosage seems to determine a reduction of the alkaline phosphatase of the 50%-80%, a clearly symptomatologic improvement19,20 and sometimes improvements in radiological and/or scintigraphic pictures too.21,31 Effectiveness lasts for long periods after a single cycle of therapy in relation to entity of abolition of the osseous turnover: the greater the abolition, especially if it is within the normal range, the longer the persistence of efficacy.23,25,29,30,32 Noteworthy, clinical improvement can also include the remission of neurological complications. 33
Following the administration of pamidronate 600 mg/day orally for an average period of 9.5 months, 80% of patients normalized their AP levels; of the 20% who did not, all had a very high initial AP level before treatment started. Of the 80% with normalized AP levels, 72% remained normalized despite the absence of any therapy during a follow-up of 2 years, 16% increased their AP levels towards pretreatment values, while in 12% AP levels increased to initial values. 34
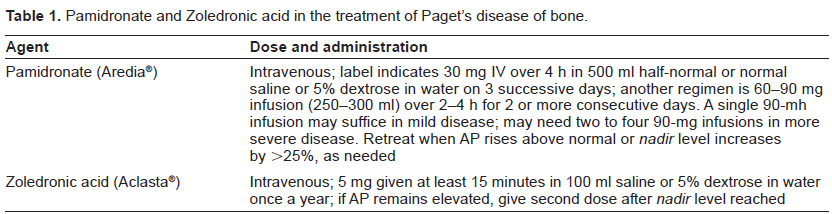
Pamidronate and Zoledronic acid in the treatment of Paget's disease of bone.
These various treatment modalities have produced a broad spectrum of results, including an improvement in spontaneous bone pain in 82% of the cases, an improvement in low back pain in 38%, an improvement in pain associated with secondary osteoarthritis of the hip and/or knee in 27% and an improvement in pain associated with deformity of the tibia or the femur in 52% of the cases. 35 With retreatment, cases of true acquired resistance are described. However, these may be considered rare and should be distinguished from apparent resistance that is observed in cases in which the resurgence of AP activity, before retreament, has not been high enough to allow a further full effect of the therapy. 36 In milder cases of PDB, a single course of therapy may bring a prolonged remission for up to 1 year. 28
In analogy with other i.v. amino-bisphosphonates, the therapy with pamidronate can be associated to an acute phase reaction (i.e. low grade fever and arthralgias) of the duration from 1 to 4 days, usually responsive to acetaminophen, especially after the first infusion, but also to uveitis.21,23,37 Prolonged pamidronate infusions may be responsible for small defects in bone mineralization of uncertain significance. 38
Zoledronic acid is the most effective aminobisphosphonate currently used. This primacy recognises both the ability to inhibit the farnesylpyrophosphate synthetase and the higher affinity to hydroxyapatite crystals as a cause. 39 These findings have justified a phase 3 trial of zoledronic acid versus risedronate in active pagetic patients. In this study the effectiveness of drugs was measured in terms of reduction of the excess of total AP: the excess is defined by the difference between the basal value of AP and the average values of the normality range. The subjects in which a reduction of at least 75% of AP was observed were considered responsive. The normalization of the enzyme, instead, was considered like a remission index. Zoledronic acid was employed to the dosage of a single infusion of 5 mg (in 15 minutes), while risedronate was used per os at a dosage of 30 mg/day for 2 months. At six months from the beginning of the study, the percentage of patients responsive to zoledronic acid was 96%, whereas it came down to 74.3% for risedronate. The percentage of remission was of 85% and 55% respectively. 40
As expected, zoledronic acid determined a much earlier biohumoral response, leading to a normalization of AP of about 90% versus 60% with risedronate. The most surprising aspect of this study was the long persistence of therapeutic effect of zolendronate so that 90% of responders remained so even after 2 years after a single administration, while patients treated with risedronate showed, in most cases, the tendency to recur within a year. 41 This study was documented for the first time as a marked improvement in the quality of life after treatment and it was significantly higher in patients treated with zoledronic acid compared with those treated with risedronate. This study has permitted the registration of zolendronate 5 mg (Aclasta®) for the treatment of PDB by the FDA and the EMEA.
The response to treatment should be based on the critical difference derived from a population with active PDB, while the concept of “remisson” is not completely clear. A relapse, in fact, may be defined as a post-treatment value outside the reference range, but in this way the true incidence of relapses may be underestimated. Because of the low-rate of bone turnover induced by treatment, it looks more appealing to calculate the least significant change to reach the critical difference from the normal population.
In addition to the well known side effects (flu-like syndrome and hypocalcemia for parenteral administration), which rarely require discontinuation of treatment, and the possible association with osteonecrosis of the jaw (ONJ), a possible increased risk of cardiac arrhythmias has recently been reported. 42
In conclusion, both pamidronate and zoledronic acid are effective in PDB, with an evidence-based superiority of the latter (Fig. 1).
Pamidronate chemical structure.
Zoledronic acid chemical structure.
Disclosures
The authors report no conflicts of interest.