
Abstract
Anticonvulsant drugs continue to be the mainstay of epilepsy treatment but benefits of seizure control need to be balanced with the psychotropic potential of this class of compounds. The present paper is aimed at discussing positive and negative effects of anticonvulsant drugs on mood in patients with epilepsy. In general terms, the use in monotherapy, adopting slow titration schedules and low doses when possible, can significantly reduce the occurrence of treatment emergent adverse events. The mental state of the patient need to be taken into account in order to really optimize the anticonvulsant drug treatment.
Introduction
Anticonvulsant drugs have a number of mechanisms of action which are likely to be responsible for their anti-seizure activity but also for their effect on mood and behavior. Previous authors suggested that two categories of compounds could be identified on the basis of their predominant psychotropic profile, 1 namely sedating and activating drugs. The former are characterized by side effects like fatigue, cognitive slowing and weight gain and usually act on the gamma amino butyric acid (GABA) neurotransmission, while the latter have anxiogenic and antidepressant properties and usually attenuate glutamate-mediated excitatory neurotransmission (Table 1). Barbiturates, valproate, gabapentin, tiagabine and vigabatrin belong to the first group, while felbamate and lamotrigine to the second. According to this model, topiramate and levetiracetam possess a mixed profile with overall very mixed effects. However, the scenario is more complicated in patients with epilepsy than in the general population due to the presence of an underlying brain disorder. In fact, the psychotropic effect of anticonvulsant drugs can be related to direct and indirect mechanisms. The former represent the main properties of the drug and can be easily predicted using the theoretical framework previously described. The latter is due to the interaction between the drug and the epileptic process. In fact, some phenomena, such as forced normalization or post-ictal psychosis, may be pharmacologically driven but occur exclusively in patients with epilepsy and are not connected with a specific drug per se. 2
Positive and negative psychotropic properties of anticonvulsant drugs.
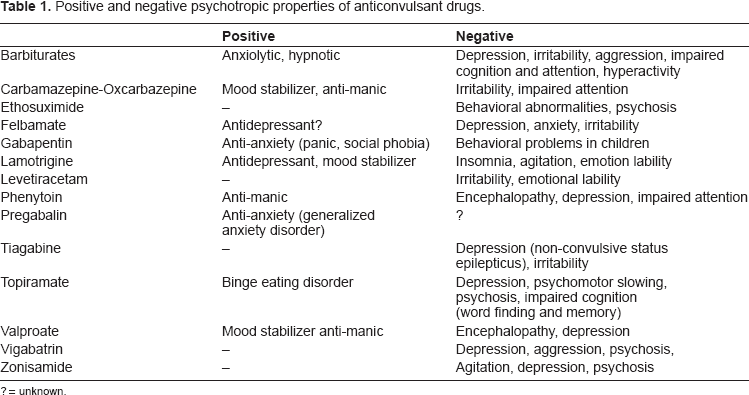
? = unknown.
Negative Effects of Anticonvulsant Drugs
It is now established that depression represents a frequent psychiatric comorbidity among patients with epilepsy 3 and may significantly affect quality of life, morbidity and mortality even more than seizures themselves. 4
Among potential neurobiological and psychosocial determinants of depression, anticonvulsant drugs play a considerable role. 2 The pathogenesis of treatment-emergent depressive symptoms is obviously multifactorial with some variables related to the drug (e.g. high dosages and rapid titration schedules, ability to reduce folate levels, potentiation of GABAergic neurotransmission) and others related to the underlying brain pathology (e.g. presence of hippocampal sclerosis, the forced normalization phenomenon). 2 These mechanisms are crucial in subjects with a past history of mood disorders, suggesting a biological susceptibility.
As far as old generation anticonvulsants are concerned, a number of studies suggested a link between depression and treatment with barbiturates (primidone or phenobarbital). An open study comparing primidone with carbamazepine showed that, over time, patients taking primidone present depressive symptoms more frequently than those taking carbamazepine. 5 Subsequently, other authors, using a double-blind crossover design, have replicated these findings using standardized clinical instruments. In this regard, it is important to point out that in children or in patients with mental retardation barbiturates may determine irritability, aggressiveness and hyperactivity. 5
Among new compounds, vigabatrin, tiagabine and topiramate, have been linked with depression as a treatment emergent adverse event. 5 Vigabatrin has been the most extensively studied, largely as a result of being the first of the new drugs to be introduced into clinical practice. It is an irreversible GABA transaminase inhibitor, determining an increase in GABA extracellular concentrations. 6 In some patients, the onset of depression was linked with a dramatic control of seizure frequency (probably a forced normalization phenomenon), while in others it was unrelated to that. However, in at least 50% of patients, treatment emergent depressive symptoms appeared to be more common in subjects with a past history of depression, 7 further confirming the importance of an underlying biological liability.
Topiramate is usually considered as having a mixed mechanism of action, but its GABAergic properties are probably prominent, and data coming from functional neuroimaging studies confirmed such a hypothesis. 8 Clinical studies have shown that depression is one of the main treatment emergent adverse events during topiramate therapy with a rapid titration schedule, a past psychiatric history and probably a more severe form of epilepsy being major risk factors. 9
In general terms, it is interesting to note that anticonvulsant drugs which seem to be frequently associated with depression as a treatment emergent adverse event, share a potentiation of the GABAergic inhibitory neurotransmission. 2 In psychiatric practice, it is well-known that long-term treatment with benzodiazepines may determine the occurrence of depressive symptoms, and withdrawal can aggravate a depressive illness. 10 This observation is not easy to explain but has been used as further evidence for a GABAergic hypothesis of depression.
Abnormalities in limbic structures represent another important variable in the pathogenesis of anticonvulsant drug-induced depressive symptoms. There is growing evidence in the psychiatric literature that depression might be linked to small hippocampal volumes. 11 Interestingly, this association has been described in patients with epilepsy but also in patients without epilepsy with a major depressive disorder. A number of studies from my group have pointed out the GABAergic potentiation is determinant in the development of depressive symptoms if this occurs in patients with hippocampal sclerosis.12,13 However, subsequent studies have suggested that functional abnormalities in the limbic systems may be even more determinant than structural ones, representing a major risk factor for the development of treatment emergent psychiatric adverse event per se.14,15 In fact, data from basic science observations showed that hyper-excitability of the hippocampus due to early insults can persist into adulthood even in structurally normal hippocampi. 16
Finally the forced normalization phenomenon needs to be acknowledged. This concept goes back to the publications of Heinrich Landolt, head of the Swiss Epilepsy Center in Zurich between 1955–1971. Landolt described EEG investigations of patients with epilepsy who had paroxysmal psychiatric disorders, describing a group of subjects with psychotic episodes and “forced normalization” of the EEG. 17 Subsequently, a number of cases of such a phenomenon have been documented to put the existence of such a phenomenon beyond doubt.2,18,19 Several psychopathological pictures have been linked to forced normalization but probably psychosis is the most frequent. 20 Wolf pointed out that several clinical pictures may evolve, not all psychotic, and noted that the development of psychotic symptoms was preceded by premonitory symptoms, especially insomnia, anxiety and social withdrawal. 21 He also noted an association with generalized idiopathic epilepsies and the prescription of ethosuximide, renovating the importance of both generalized seizures and suximide drugs in the development of these peculiar behavioral problems. 22
Positive Effects of Anticonvulsant Drugs
It is important to acknowledge that anticonvulsants are extensively used in psychiatric practice for a broad spectrum of psychiatric disorders. The primary application is in mood stabilization but interesting data are coming out also regarding anxiety disorders 23 and withdrawal syndromes. 24
As for the old generation of anticonvulsant drugs, carbamazepine demonstrated positive psychotropic properties since its introduction for the treatment of epilepsy.2,5,25 Over time, a number of controlled studies have been carried out evaluating the effects of carbamazepine in acute mania against placebo, lithium or antipsychotic drugs. These studies have shown that carbamazepine is equivalent to lithium in many cases, and, although the time course of the anti-manic effect seems to be a little slower than that reported with neuroleptics, it seems to be fairly equivalent to lithium. 26 This is relevant for those patients who are refractory to lithium and require an alternative, especially subjects with unstable forms of bipolar disorder with rapid fluctuations (rapid cyclers).
Valproate has been used in the treatment of acute mood episodes (both mania and depression) and in the maintenance therapy of bipolar disorder, although the strongest supporting evidence is for acute mania. 26 There is possibly an effect in behavioral problems associated with mood instability, aggressiveness, and impulsivity across a range of different clinical contexts (i.e. borderline personality disorder) but controlled studies are currently available mainly for bipolar disorders.
As far as new compounds are concerned, some of them (i.e. tiagabine, gabapentin) have failed to show any efficacy in primary psychiatric disorders while others (e.g. topiramate) might have adjunctive uses, such as the management of weight gain associated to atypical antipsychotics or in comorbid eating disorders.26,27 Data about oxcarbazepine are definitely less conclusive than those regarding carbamazepine. It seems to be less effective than lithium but as effective as carbamazepine in acute mania; 26 however, it has to be acknowledged that oxcarbazepine is probably better tolerated than carbamazepine.
Cumulative results of the studies on lamotrigine provided evidence that it is effective in the management of the depressed phase of bipolar disorder type II and in the long term maintenance treatment of patients with rapid cycling bipolar disorders. 26
Some new generation compounds (i.e. gabapentin and pregabalin) have demonstrated some efficacy in anxiety disorders. 23 For both drugs N-P/Q type channels represent the main molecular target, in particular the alpha-2-delta subunit, type 1 and type 2. Pregabalin is probably the most interesting molecule on this regard, with a number of controlled studies demonstrating that it is better than placebo in generalized anxiety disorder. 23
Available literature currently suggests an important role for anticonvulsant drugs in psychiatric disorders, but it would be misleading to transfer these findings directly from psychiatric patients to epilepsy patients. It would be clearly useful to have controlled data clearly demonstrating that anticonvulsant drugs have a positive influence on the psychic status of patients with epilepsy beyond their influence on seizure activity. However, there is still little scientific evidence for that. In fact, most of the studies are uncontrolled and based on quality of life measures rather than on a formal psychiatric evaluation. For example, the possibility of using the same compound as both an anticonvulsant and an antidepressant would be of great importance for a rational optimization of drug therapy in patients with uncontrolled epilepsy and comorbid psychiatric disorders. Further studies are urgently needed. Lamotrigine is the only drug whose positive psychotropic properties have been investigated in patients with epilepsy. A few controlled studies have shown a significant improvement in quality of life outcomes when lamotrigine is compared to carbamazepine or valproate but studies addressing the specific issue of depression are lacking. 5 Studies from our group reported that lamotrigine co-therapy was associated with a low prevalence of treatment emergent psychiatric adverse events with topiramate 9 or levetiracetam. 28 Therefore, all these studies taken together seem to suggest a possible positive role of lamotrigine in patients with uncontrolled epilepsy and depressive symptoms. In this issue of Clinical Medicine: Therapeutics, the article by Schiller and Krivoy reviews available literature about the antidepressant properties of lamotrigine in a special population of patients with epilepsy, namely elderly patients. 29 In clinical practice, patients presenting with epilepsy and comorbid psychiatric conditions should always have their anticonvulsant drugs reviewed in order to tailor the appropriate therapy according to the psychic status of the patient. The availability of a wide number of medications for epilepsy warrants the optimization of treatment according to the characteristics of the individual and the paper published in this issue represents a useful contribution, especially in the light of the current debate on risk of suicide and prescription of anticonvulsant drugs. 30
Disclosure
This manuscript has been read and approved by the author. This paper is unique and is not under consideration by any other publication and has not been published elsewhere. The author reports no conflicts of interest.
Footnotes
Acknowledgments
The author has not been paid for the present paper. In the past, he has received travel grants or consultancy fees, from various pharmaceutical companies including Novartis, Pfizer, UCB-Pharma, Janssen-Cilag–-involved in the manufacture of antiepileptic drugs.