
Abstract
Sapropterin has recently been approved to treat hyperphenylalaninaemia in patients over 4 year-old with tetrahydrobiopterin (BH4)-responsive phenylketonuria (PKU) and in children and adults with BH4 deficiency. 1 The effectiveness of this treatment in BH4-responsive PKU patients has already been demonstrated in randomized, double-blind trials; 2 moreover, Sapropterin appears well tolerated in PKU patients. It is thus the first non-dietary treatment for patients with PKU demonstrated capable of lowering blood phenylalanine levels, and as a result, it is a promising treatment option for BH4 responsive PKU patients. Yet there are still many open questions related to this treatment. One such question concerns how a positive responsiveness to BH4 is defined. Generally, a positive response is established when the baseline level of blood phenylalanine (Phe) decreases at least 30% after a BH4 load, but the practice of this particular loading test differs widely among different countries. The second question concerns the long-term usage, i.e. no long term tolerability data was available before. Finally, the issue regarding its usage in children less than 4 year-old and in maternal PKU patients remained to be addressed.
Structure and Mechanisms of Action
Sapropterin dihydrochloride (Kuvan®), hereafter referred as sapropterin, is a synthetic formulation of the active 6R-isomer of tetrahydrobiopterine (BH4), the natural cofactor for phenylalanine hydroxylase. Biopten® is another formulation of sapropterin, which is approved in Japan for the treatment of hyperphenylalaninaemia arising from either tetrahydrobiopterin deficiency or phenylalanine hydroxylase deficiency. BH4 is first prescribed for treating primary BH4 deficiencies. Sapropterin, like the exogenously prescribed BH4, is given as a replacement for endogenous BH4. However, the usefulness of this particular formulation was to be assessed in the PKU-related patient population, and BH4 had been found rather effective in reducing plasma phenylalanine levels. 3 Meanwhile, exogenous BH4 treatment had become the standard treatment for the BH4 responsive PKU patients; we will thus focus this review on this new development. A significant number of PKU patients responded positively to oral administration of BH4. This positive responsiveness was related to the presence of residual phenylalanine hydroxylase (PAH) activity. 4 Findings from an in vitro study using a series of 15 PAH mutants showed that 14/15 BH4 responsive PKU patients had >30% residual PAH activity. 5 This treatment restored enzyme activity in vivo, reduced blood phenylalanine concentration, and significantly increased dietary-protein tolerance. 4 The exact molecular mechanism for the exogenously administered BH4 in PKU patients is not fully elucidated, although several possible hypotheses have been put forward.5,6 These include: PAH mutants with a lower BH4 affinity that can be overcome through supplementation; misfolded PAH mutants that can be corrected by the chaperone effect of BH4 through the stabilization and the protection of the mutant proteins from proteolytic degradation.5,6
Metabolism and Pharmacokinetics
Studies in healthy volunteers have shown a rather comparable oral sapropterin dihydrochloride absorption when the tablet form of the medication is dissolved in water or orange juice and taken under fasted conditions. Oral absorption was found even better when the tablet was given with or after high-fat, high-calorie meals, with an average Cmax (maximum concentration) 40%–85% higher 4–5 hours after taking the medication. 7 It is thus recommended that sapropterin be administered with meals around the same hour every day. The absorption and the elimination of sapropterin was best described by a two-compartment pharmacokinetic model with first-order input and first-order output under the presence of a constant level of endogenous BH4. 8 Total bodyweight was the only significant covariate identified in this model. The average half-life of sapropterin was 6.69 (SD 2.29) hours and there was little evidence of accumulation, even at the highest dose used. These findings suggested that once a day administration of the drug is appropriate. 8 Pharmacokinetic studies further unveiled an extensive interindividual variability in BH4 handling based on values such as Cmax and AUC (area under the curve) obtained across different modes of administration and meal composition. Such variability can be due to a decreased BH4 absorption from the intestine due to age. 9 Despite this large interindividual variability in the absolute levels of BH4 metabolites reached after BH4 loading, very similar time to peak biopterin and pterin (blood and plasma) were found in all patients. As expected, BH4 and its metabolites level increases significantly with increasing BH4 dose. In some patients, a twice-daily administration was found more appropriate. However, no correlation exists between the BH4 blood (and plasma) level and the reduction in blood Phe. 10
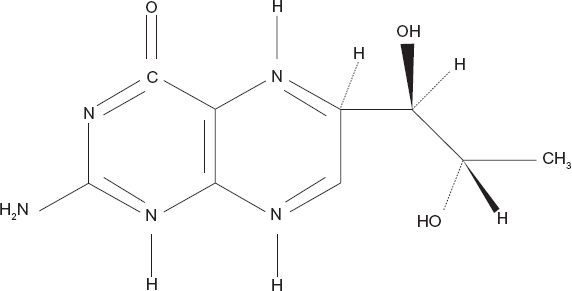
Chemical structure of sapropterin.
Potential Drug Interactions
So far, no report is available in human study regarding the interaction of sapropterin with other drugs. Still, it is recommended that sapropterin be used with caution when coadministered with drugs such as methotrexate. These drugs can inhibit dihydropteridine reductase, thus interfering with folate metabolism and eventually reducing effective BH4 level in cells. 7 Since BH4 is also a cofactor for nitric oxide synthase, sapropterin may induce vasodilation mediated by nitric oxide; its use in patients receiving drugs such as glyceryl trinitrate, isosorbide dinitrate, sodium nitroprusside, molsidomin, minoxidil and phosphodiesterase-5 inhibitors (e.g. sildenafil, vardenafil, tadalafil) should thus be carefully monitored. In a 10-year post-marketing survey of another formulation of BH4 used in the treatment of BH4 deficiency, three patients experienced convulsions, exacerbation of convulsions, irritability or overstimulation when the drug was given together with levodopa. 11 Caution should thus be taken in patients with diseases such as Parkinson disease.7,12
Clinical Studies
The first report of BH4 responsive PAH deficiency was published in 1999 by Kure et al 13 and this BH4 responsiveness was confirmed and related to an increase in PAH activity in 2002. 4 Then, the efficacy of oral sapropterin in patients with PKU was evaluated in a series of studies from North America and Europe.2,14–16 These studies were performed in three stages: first, a screening study; then a randomized, double-blind, multicentre trial for comparison with placebo and finally, an extension study.
Among all baseline characteristics measured, the only difference between groups was a higher proportion of males in the sapropterin group. 2 Treatment compliance was high; 72/88 (82%) patients took all doses of the study drug correctly throughout the 6 weeks of the study. The results showed that mean blood phenylalanine concentration at baseline was 842.7 (SD 299.6) μmol/L for the sapropterin group and 888.3 (323.1) μmol/L for controls. At 6 weeks, 18/41 (44%) patients given sapropterin (95% CI 28–60) and 4/47 (9%) controls (95% CI 2–20) had a blood phenylalanine reduction of 30% or more from baseline (p = 0.0002). Blood phenylalanine concentration was reduced by 50% or more in 13/41 (32%) patients who had received sapropterin (95% CI 18–48) and 1/47 (2%) controls (95% CI 0–11). At week 6, the mean change in blood phenylalanine from baseline for the sapropterin group was -235.9 (257.0) μmol/L, compared with 2.9 (239.5) μmol/L for controls (p < 0.0001). Blood phenylalanine levels at weeks 1, 2 and 4 (secondary endpoint) were also lower in sapropterin than placebo recipients (620 vs. 863 μmol/L, 639 vs. 863 μmol/L and 587 vs. 906 μmol/L, respectively (p < 0.0001). 1 11/47 (23%) patients in the sapropterin group and 8/41 (20%) patients in the control group experienced adverse events that might have been drug–related (p = 0.80). No patient withdrew from the study because of adverse events (see the safety section). Full PAH genotypes were available for 17 of the 19 patients who showed a 30% or more reduction in blood phenylalanine in response to sapropterin. In one patient, only a single mutation was identified and in the other a genotype was not available. If responsiveness to BH4 is thought to require at least one PAH mutation that allows for residual enzyme activity (non-null mutation), 17 there was no consistent relationship between specific mutations and BH4 responsiveness.
Safety
In clinical trials, Kuvan has been administered to 579 patients with PKU in doses ranging from 5 to 20 mg/kg/day for lengths of treatment ranging from 1 to 30 weeks. Patients were aged 4 to 49 years old. The patient population was nearly evenly distributed in gender and approximately 95% of patients were Caucasian. The most serious adverse reactions during Kuvan administration (regardless of relationship to treatment) were gastritis, spinal cord injury, streptococcal infection, testicular carcinoma, and urinary tract infection. Mild to moderate neutropenia was noted during Kuvan administration in 24 of 579 patients (4%). No sapropterin recipient had clinically significant changes in ASAT or ALAT. 2 Hypophenylalaninemia has been noticed in more than 1% of the treated patients, but this is more the consequence of a too high dosage of sapropterin than a real adverse event related to the drug. The most common symptoms (≥4% of patients treated with Kuvan) across all studies (n = 579) were headache, diarrhea, abdominal pain, upper respiratory tract infection, pharyngolaryngeal pain, vomiting, and nausea (Table 1). The overall incidence of adverse reactions in patients receiving Kuvan was similar to that reported with patients receiving placebo. In the extension study, no medical interventions related to adverse events were required. 15 In the pediatric phenylalanine tolerance trial, 16 that included children with PKU aged 4–12 years, most adverse events were of mild severity and most were thought not to be related to the study drug. There is minimal or no reliable sapropterin tolerability data in children with PKU who are <4 years of age, 20 in pregnant women21,22 or for treatment extended beyond 22 weeks. Some patients treated up to 18 or 24 months have been reported with a constant effect of the drug without adverse events.23,24 One patient has been treated from birth until 25 months of age without adverse events. 25 The safety and efficacy of sapropterin in patients with renal of hepatic impairment of who are aged >65 years has not yet been established.7,11
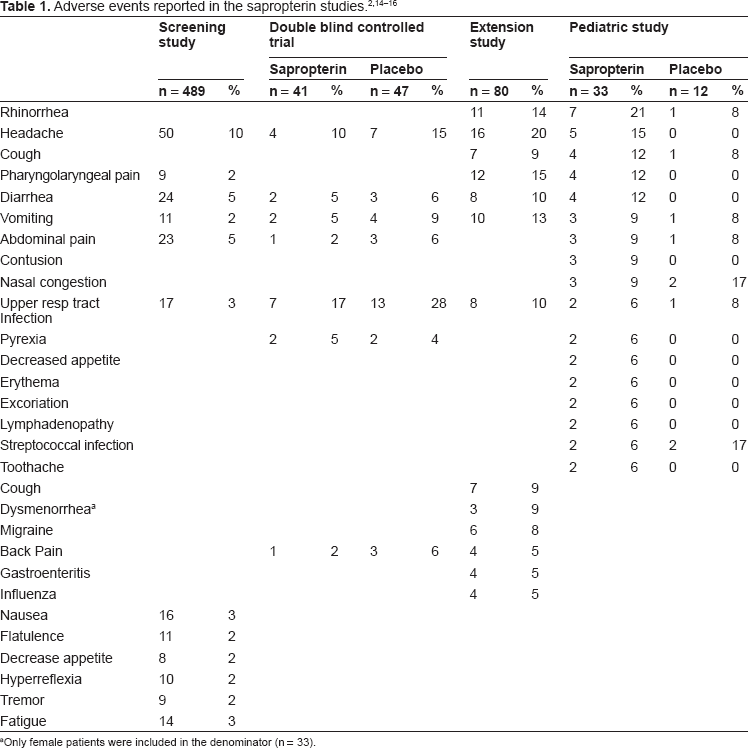
Only female patients were included in the denominator (n = 33).
It is worth noting that BH4 can induce some side effects which are not directly related to the drug itself. The nutritional status of the PKU patients treated by BH4 must be closely followed because, a metabolic control can be reached with BH4 associated to a vegan-like diet, and this can induce some micronutrients deficiencies. 26 Another side effect is linked to the feeling that patients can eat what they want because of the “magical drug” with a worsening of the metabolic control under BH4 (personal experience).
Efficacy
The efficacy of Kuvan has been demonstrated by 2 randomised placebo-controlled studies in patients with BH4 responsive PKU. The results of these studies demonstrate that Kuvan reduces blood phenylalanine levels and increases dietary phenylalanine tolerance.2,16 These data have been described in the clinical studies section. The long term efficacy of Kuvan has been demonstrated for patients with primary BH4 deficiencies 27 for up to 5 years; in PKU patients under continuous treatment of this 6R-BH4 preparation, reduced blood Phe levels were achieved without the incidence of adverse effects.23–25,28,29
Which Patients must be Treated?
Today, the main issue concerns not the question if BH4 can be efficient in treating PKU patients, but the question which patients can benefit from this treatment. Oral administration of BH4 (using the unregistered formulation) has led to clinically significant reduction in blood Phe level in about 80% of patients with mild hyperphenylalaninemia (HPA), about 50% of patients with mild PKU, and only about 10% of patients with classical PKU. A BH4 loading test is necessary to determine who should be treated. A decrease in blood Phe level of at least 30% is often used as a cut-off point to determine if BH4 treatment is required, although this is arbitrary.30,31
Sapropterin is suggested to be used for the treatment of HPA in patients with PKU who have been shown to be responsive to such treatment. Thus, all patients with PKU should undergo a sapropterin oral-response test before the initiation of treatment. 32 In USA, according to the FDA-approved algorithm, a measurement of blood Phe is followed by an initial daily dose of sapropterin at 10 mg/kg/day for 1 week; then, at the end of the 7th-day treatment, a repeat blood Phe measurement is taken. For patients whose blood Phe level is not lowed sufficiently, the dose can be increased to 20 mg/kg/day and their blood Phe level be followed for a total treatment period of up to 1 month. 33 In Europe, a recent expert commentary proposed an alternative test for identifying responders to BH4 therapy.32,34 This involved administration of a single dose of BH4, 20 mg/kg, followed by serial measurements of blood Phe during the following 24 h. This test considered a reduction in blood Phe of at least 30% as the primary determinant of BH4 responsiveness.32,33 Using this test (single 20 mg/kg administration with blood Phe monitoring over 24 h and with the 30% cut-off), the overall prevalence of BH4 responsiveness in patients with PKU was found to be 46%. 31 It should be noted, however, that this test of BH4 responsiveness is not consistent with the FDA-approved Prescribing Information for Kuvan, 11 but this test is used by the vast majority of the PKU centers in Europe. 35
In Europe, the BH4-loading test is also performed during the neonatal period. 20 If the blood Phe level in neonates is high enough, this test is performed. In case where a child is under strict dietary control, a Phe ‘challenge’ (50–100 mg/kg) must precede the BH4 administration. However, questions remain as to how to interpret these data without a preceding single Phe load. A number of different protocols have been practiced using various unregistered formulations of BH4 and sapropterin.14,30,33,36 These studies employed various diet regimes (normal or a Phe-restricted) and doses, and used various time periods to assess the effect on blood Phe (a 24 h test may detect slower responders more effectively than an 8 h test); the frequency of treatment (single or multiple doses) as well as the measurement of efficacy (blood Phe levels or the half-life of decreases in blood Phe) 32 differed in these studies as well. It should be noted that a 30% reduction in blood Phe is often considered as a clinically significant response to justify a treatment; however, it is important to note that this threshold is arbitrary and some medical professionals consider smaller reductions to be clinically significant. Clearly, a simple and universal loading test would facilitate the identification of responders to sapropterin. Such a test must be practical in its application and be sufficiently predictive for BH4 responsiveness while restraining the number of measurements needed.
Patient Preference
Treatment of patients with PKU should focus not only on ameliorating the metabolic control or the tolerance of Phe but also on applying a more holistic approach including the patient's subjective experience with the treatment, e.g. desired effects, side-effects, cultural acceptance of treatment and diet versus non-diet treatment should be applied. 37 We know that adolescents and young adults generally do not comply with the recommendations for the monitoring and the control of phenylalanine concentrations. Should phenylketonuria be proven dangerous in adults as it is in infants, maintenance of good dietary control beyond childhood will become increasingly important, and more acceptable modes of treatment than diet will need to be developed. 38 Sapropterin treatment, as it increases the Phe tolerance and decreases the burden of the diet, can even replace the dietary control in some fully responsive PKU patients (normalization of the Phe levels after the BH4 loading test). There have been great expectations and disappointments for this treatment among PKU patients. First, not all patients are responsive and thus it must be announced clearly when the BH4 loading-test is proposed to the patient and its family. Second, the extent of responsiveness will determine how the diet can be improved; for example, in patients with a 30% reduction in blood Phe level after the BH4 loading test, BH4 treatment will not modify that much the day to day diet while a patient with 50% (or more) decrease in Phe level, BH4 can completely change the dietetic management, resulting in a real improvement in the quality of life for the patients. Adherence to treatment is important; it lays the foundation for clinical effectiveness. As PKU patients do not feel the consequence of the relaxed diet during adulthood, it will be very important to study the long-term compliance to BH4 in PKU, mostly in adulthood because if the treatment is a novelty of today, it can be experienced as a constraint with time (as many other treatments in other conditions).
Studies about the modification of quality of life before and after BH4 are still lacking, and these studies are critical because BH4 is not the first efficient treatment of PKU. To be sure that BH4 is a real progress in PKU management; we must have the proof that this treatment improves the quality of life for PKU patients compared to the previous treatments.
Place in Therapy
Sapropterin is a synthetic formulation of the active isomer of tetrahydrobiopterin and is a new therapy for patients with PKU or tetrahydrobiopterin deficiency who are tetrahydobiopterin- responsive.39–41
In tetrahydrobiopterin deficiency, the mechanism of action of sapropterin is presumed to be the replacement of endogenous tetrahydrobiopterin. 3 No studies with the sapropterin formulation considered in this review have been conducted in patients with tetrahydrobiopterin deficiency. In an open-label trial in 16 patients with tetrahydrobiopterin deficiency, another sapropterin formulation (Biopten®) led to a marked global improvement in 87.5% of patients; all enrolled patients had blood phenylalanine levels maintained ≤181.6 μmol/L during the treatment period (mean 15.5 months). 7 The efficiency of BH4 in primary BH4 deficiencies is known for decades now, as Kuvan is the only pharmacologic presentation of BH4 in many countries it will probably be an “off-label” prescription until studies about the use of Kuvan in this particular indication will be published.
In PKU patients, tetrahydrobiopterin responsiveness is thought to be related to the presence of less active phenylalanine hydroxylase mutants that have the potential to become more active when exposed to high levels of its essential cofactor. In this indication, Kuvan has been authorized by the US and the European agencies in 2007 11 and 2009. 7 The regulations are slightly different in the two versions of the approval. In the US, Kuvan is only approved for BH4 responsive PAH deficiency (in patients responsive to such treatment) and it is to be used in conjunction with a Phe-restricted diet. There is no restriction in age in the indication section of the US version of the approval. The European Medicines Agency (EMA) authorized Kuvan in 2009, with a restriction to the PKU patients aged >4 years of age. EMA also authorized the use of Sapropterin in PAH deficiencies as well as primary BH4 deficiencies. In both versions, BH4 treatment is indicated in PKU patients who have been shown to be responsive (with the difficulties due to the lack of consensus about the definition of BH4 responsiveness and how to determine it).33,34
The second step is to determine who should be treated, as there is no consensus on this point too. Some guidelines recommend to treat patients whose Phe levels are above 400 μmol/1 42 and some others only in patients whose Phe levels are above 600 μmol/l. 19 The only published data on the outcome of HPA patient indicate that patients with Phe levels < 600 μmol/L are unlikely to be treated because their outcome (without treatment) are normal.43,44 As BH4 responsive PKU patients are mostly the mild hyperphenylalaninemic patients, this question is critical because some patients will be treated in some countries while some wouldn't be treated in some other countries.19,45 As the cost of the drug is high, it is very important to know if these patients are worthy to be treated or not.
The majority of patients who will benefit from this new treatment of PKU are the mild PKU patients who are responsive to the BH4 loading test. As the Phe-controlled diet itself is efficient enough as a treatment, the added benefit of BH4 is to improve the quality of life for the patients as much as a treatment. The difficulty will be to appreciate how much this new treatment improves the quality of life for these patients. Only a small number of patients have been reported to be able to stop supplementation with the amino acid mixture as a result of long-term BH4 treatment.23,46 In the study of Lambruschini, Phe tolerance (daily Phe intake allowing for blood Phe levels of 120–360 μmol/L) increased significantly (p = 0.004) in 9 patients with mild PKU and in 2 out of 4 patients with moderate PKU, during the long-term treatment with 5 mg BH4/kg bw per day. 46 Phe intake was increased by 200 mg/day. Mean Phe tolerance increased from 356 ± 172 mg/day to 1546 ± 192 mg/day. The Phe-free amino acid mixture could be completely removed from some patient's diet.
In a recent study, 63% of the patients with blood Phe levels > 450 mmol/L, showed a positive response to loading and were therefore suitable for long-term treatment. 47 They were treated with BH4 (10 mg/kg per day) over a period ranging from 6 months to 7 years. All the patients benefited from BH4 substitution, which allowed a substantial relaxation of the dietary restrictions. Before BH4 treatment, Phe tolerance was less than 700 mg/day in all patients but one, increasing to 2–3-fold on BH4 treatment. In these patients the amino acid mixture supplementation was stopped and the diet was a mixture of low-protein foods and natural proteins mostly from animal source. In these cases, the quality of life is very much improved and BH4 is a real change in the patient's life. In another study, increase in Phe tolerance was not sufficient to cover protein requirements from natural protein alone. 28
In the Lambruschini study, BH4 therapy was discontinued when Phe tolerance could not be increased by more than 400 mg/day and the amino acid mixture could not be completely removed. 46 Interestingly, this study showed that the nutritional status of PKU patients were improved under BH4 therapy compared to the low-Phe diet. 46 Despite identical intake of selenium, the selenium status improve with BH4 therapy, These data would suggest an increased selenium bioavailability of natural diet compared with that of the special formula. 46
To conclude, the benefit of Kuvan in PKU responsive patients must be evaluated on an individual basis, taking in account the level of responsiveness to BH4, the difficulty for diet compliance and the improvement of the quality of life that Kuvan bring to the patient. It is possible that Kuvan will be more adapted to older patients than to younger ones because the required metabolic control is less severe after adolescence, and these levels can easily be reached with Kuvan, rather than through the strict Phe control required for younger ages. This remains to be proven by adequate studies. As there are no studies on cognitive function in patients treated with sapropterin, 11 it will also be necessary to confirm that the controlled dietary relaxation with sapropterin treatment produces equally favorable cognitive outcomes to that seen with the dietary treatment alone. 1 Further research is also necessary to strengthen the assumption that the currently recommended blood phenylalanine levels are appropriate since no evidence has shown these levels to be harmful to the developing brain. 48 With all available evidence favoring the maintenance of a lowered phenylalanine blood level throughout life, adherence to treatment is a critical issue that can be improved with the sapropterin treatment alone with the loosening of a phenylalanine-restricted diet, although at an increased cost. Evidently, the consequent complexity in regimen could, of course, have the opposite effect. 48 Certainly, patient education and follow up is essential to ensure that the affected patients and their families understand that sapropterin treatment does not obviate the need for continued dietary control and monitoring.7,11
Hyperphenylalaninaemia in pregnancy is associated with fetal abnormalities, including mental deficiency, microcephaly and congenital heart defects.49,50 There are no (or very few) clinical data on the use of sapropterin in pregnancy,21,22 but in animal studies no direct or indirect maternal or fetal harmful effects were observed. 7 Tetrahydrobiopterin is considered a promising treatment in pregnant women. In EU, the physician-supervised dietary control of phenylalanine intake before and throughout pregnancy as the first line of treatment, with sapropterin treatment considered only when strict dietary management fails to adequately lower blood phenylalanine levels 7 (in the summary of product characteristics). A post marketing registry about maternal PKU (and children aged less than 4 years) has been asked by the European Medicines Agency to confirm the safety of Kuvan in these particular populations.
Conclusion
Oral Sapropterin effectively lowers the blood phenylalanine level in a proportion of patients with PKU. Sapropterin is well tolerated in patients with PKU, although longer-term tolerability data are required. Sapropterin is the first non-dietary treatment for patients with PKU that has been shown in randomized, double-blind trials to be effective in lowering blood phenylalanine level. Thus Sapropterin provides a new option for BH4 responsive PKU patients. 12
Conflict of Interest Statement
I declare that we receive consultant fees by Merck Serono.