
Abstract
Arformoterol tartrate is a newly developed long-acting ssβ2-agonist with both acute and prolonged bronchodilator effects. It is formed of 2 isomers (R,R/R,R) which distinguishes it from the more commonly used racemic formoterol (R,R/S,S). The active isomer is the (R,R) and in vitro arformoterol may have more potent anti-inflammatory effects than formoterol. It can only be given by a nebulizer. There have been 5 randomized, blinded trials which have assessed the use of arformoterol in chronic obstructive pulmonary disease (COPD). Arformoterol has been demonstrated to improve lung function and symptoms but the subjects tested did have a high degree of airway reactivity. The medication was well tolerated with a low incidence of side effects but the trials may not have been of sufficient duration to assess this adequately. Arformoterol should be used with caution in subjects with underlying cardiac disease. The current main use of arformoterol is in those subjects with COPD who require a long acting β2-agonist but who cannot use a dry powder or metered dose inhaler preparation. Arformoterol may only need to be given once a day and can be combined with other inhaled medication particularly tiotropium for additional benefit. It potentially has a role in the management of acute exacerbations.
Introduction
Chronic obstructive pulmonary disease (COPD) is currently a major and increasing cause of mortality and morbidity and by 2020 it is estimated that it will be the third leading cause of death and the fifth leading cause of mortality worldwide.1,2 COPD is characterized by chronic inflammation that results in progressive airflow obstruction that is not fully reversible. The Global Initiative for Chronic Obstructive Lung Disease (GOLD) 3 classifies COPD into 4 groups based on lung function ranging from mild disease (stage I) to very severe (stage IV).
Current pharmacological treatment for COPD has not been shown to modify decline in lung function or reduce mortality. The current main aims in therapy are to reduce symptoms and exacerbations, improve exercise capacity and quality of life. 4 Bronchodilators are the main medication used to treat COPD and there are 4 categories: anticholinergics, methyxanthines, short-acting β2-agonists (SABA) and long-acting β2-agonists (LABA). Patients with moderate to severe (stages II-IV) are usually treated with a long-acting bronchodilator or combination.
Maintenance therapy with long-acting β2-agonists is more effective and convenient than short-acting β2-agonists 3 is well tolerated, improves lung function and health status and reduces exacerbations in COPD.3,5,6 LABAs such as salmeterol and formoterol promote bronchodilation for at least 12 hours and have been used extensively in the treatment of patients with COPD. Long-acting β2-agonists have primarily been formulated as metered dose inhalers (MDI) for dry powder inhalers (DPI). Some patients have difficulty using these inhalers, leading to poor compliance with treatment. 7 Arformoterol tartrate a formulation of the (R,R) isomer of formoterol, has been developed which is administered by nebulization. Arformoterol has been approved for the maintenance and treatment of bronchoconstriction in COPD.
Recent asthma literature has raised concerns about the long-term use of LABAs. 8 COPD patients also often suffer from multisystem problems disease, especially cardiovascular disease 9 and this may be affected by the use of LABAs.
Mechanism of Action, Metabolism and Pharmacokinetic Profile
β2-agonists act on the β2-adrenoreceptors of smooth muscles on the bronchi resulting in relaxation of the muscle and bronchodilation. Salmeterol is a partial agonist at the β2-adrenoreceptor with a maximal effect after 1 hour. 10 In contrast formoterol is a full agonist with a rapid onset of action with effective bronchodilation occurring 5 minutes after administration, similar to the effect of a short-acting β2-agonist. 11 The additional methoxy group on the side chain of formoterol may be responsible for the different action in comparison to salmeterol.12,13
Formoterol also has other airway effects in addition to bronchodilation. Formoterol decreases airway microvascular leakage through the β2-adrenoreceptor on the endothelial surface of post-capillary venules14,15 and sputum α-2 macroglobulin. 16 Neutrophils express β2-adrenoreceptors and LABAs have been shown to decrease bronchial neutrophils17,18 and the release of reactive oxygen species.19,20
The effects of formoterol are mediated through the activation of intracellular adenyl cyclase, which results in the formation of cyclic adenosine mono-phosphate (cAMP). The maximum plasma concentration of formoterol is reached within 5 minutes of inhalation. Urinary excretion demonstrated that absorption of formoterol in the lungs was linear and in COPD patients similar plasma concentrations at 10 minutes to 6 hours post inhalation occurred.21,22 Formoterol is metabolized in the liver by the cytochrome P450 enzyme system. The mean half-life in a small group of controls was 10 hours.11,22 There is no data available to guide the use of formoterol in older patients or those with hepatic or renal disease.
β2-agonists are comprised of a 50:50 mixture (racemates) of (R,R) and (S,S)-isomer (or enantiomer). 23 The bronchodilator effect is mediated by an interaction between the (R,R) isomer and the β2-adrenoreceptor. 24 The (S,S)-isomer may inhibit airway relaxation. The formoterol compound is composed of stereoisomers (i.e. the atoms in the molecules have different arrangements in space) around 2 chiral centers with 4 possible combinations (R,R), (R,S), (S,R) and (S,S). Formoterol is a (R,R/S,S) diasteriomer whilst arformoterol is an (R,R/R,R)-enantiomer. As the (R,R) is the active isomer, arfomorterol may have more potent pharmacologic effects than formoterol. However two studies have not been able to demonstrate any clear differences in bronchodilation between the 2 preparations.23,25
β2-agonists may worsen asthma by increasing airway inflammation 26 an effect that may be arising from the different isomers. The (R,R)-isomer is anti-inflammatory and the (S,S)-isomer is proinflammatory as demonstrated by albuterol; the (R,R)-isomer is anti-inflammatory while the (S,S)-isomer has an inflammatory effect on T cells. 27 (R,R)-formoterol reduces levels of granulocyte macrophage-colony stimulating factor (GM-CSF) in airway smooth muscle cells whilst the (S,S)-isomer had the opposite effect. 28 Steinke et al found that (R,R/R,R) formoterol decreased T cell mediated inflammation whilst (R,R/S,S) racemate formoterol had the opposite effect. 29 These 2 studies demonstrate at least in vitro that (R,R/R,R) formoterol may have useful anti-inflammatory effects.
Clinical Efficacy
There has been increasing interest in the use of formoterol for the treatment of COPD and this topic has been reviewed recently.30,31 Four recent randomized trials have demonstrated improved symptoms, lung function and decreased exacerbations with the use of formoterol.32–35
There have been 5 published studies that have assessed the clinical efficacy of arformoterol. These studies have been of good quality and have generally been randomized and double-blinded. The combined numbers in the trials now total approximately two and a half thousand subjects. These trials have all come from the same group of authors.
Two identical, randomized, double-blind, placebo controlled assessed the effect of arformoterol given over a 12 week period.36,37 Subjects were randomized to receive placebo, arformoterol (15 μg twice daily, 25 μg twice daily or 50 μg daily) or salmeterol MDI (42 μg twice daily). Subjects were followed up for 12 weeks and outcome measures were percent change in trough forced expiratory volume in 1 second (FEV1), percent change in FEV1 and peak percent change in FEV1 from pre-dose. A total of 1456 subjects completed the 2 trials and data was pooled from both trials. The results demonstrated an improvement in trough FEV1 for both salmeterol and arformoterol versus placebo. After 12 weeks 78%-87% of arformoterol subjects had a ≥ 10% increase in FEV1 compared with 56% in the salmeterol group and 44% of the placebo group. The median time to improvement in FEV1 (i.e. at least 10% change from pre-dose) was much more rapid with arformoterol (3-13 minutes) compared to salmeterol (142 minutes). The results showed that arformoterol was an effective bronchodilator in this cohort of subject; perhaps more so than salmeterol. It would have been helpful to also have an arm with racemic formoterol as well. Subjects all had a significant smoking history with a mean of >than 60 pack years and a mean FEV1 of 41% of predicted. The major criticism of this trial was the high proportion of subjects who had a significant bronchodilator (BD) effect. The article stated that patients had physician diagnosed nonasthmatic COPD but the mean airway reversibility of the group was 18.5% at the initiation of the trial. There is no detail as to how asthmatic subjects were excluded or whether the degree of initial airway reversibility affected outcomes.
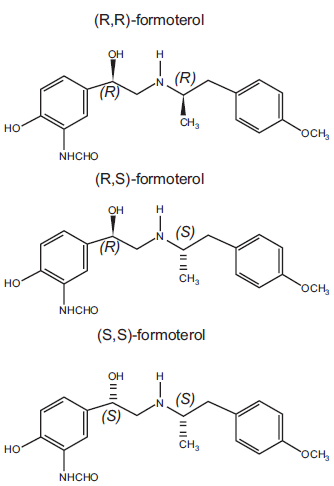
Shows the stereoisomers of arformoterol. Each isomer contains 2 chiral centers. (R,R), (R,S) and (S,S) isomers of formoterol are shown. Each isomer is joined to another isomer to make the final compound e.g. (R,R)(R,R)-formoterol is arformoterol.
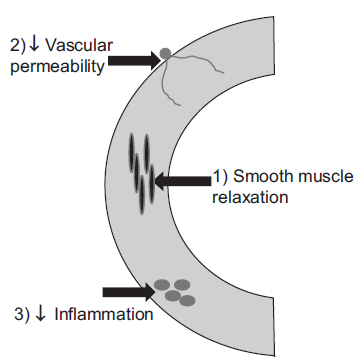
Shows the effect of arformoterol on bronchial wall. 1) Relaxation of smooth muscle mediated by higher levels of cAMP leading to reduced hyperinflation and improved respiratory muscle function. 2) Inhibition of vascular permeability. 3) Antiinflammatory effects (mediated by (R,R)-formoterol).
Kharidia et al 38 compared the effect of arformoterol to racemic formoterol in a small trial of 39 subjects with COPD (GOLD class 2-4, mean FEV1 of 1.4 L; 44% predicted). An open-label randomized three-way cross-over design was used with twice-daily treatments of nebulized arformoterol (15 μg) and formoterol (12 and 24 μg) for 14 days. The trial measured the blood levels of the two isomers of formoterol (i.e. R,R and S,S) which were compared with the % change in trough FEV1 from baseline to day 14. This trial found the degree of bronchodilator effect was proportional to the level of R,R isomer of formoterol in the blood and arformoterol produced a higher level of R,R isomer when compared with racemic formoterol. The trough increase in FEV1 was 19% with arformoterol (15 μg) and 16% with formoterol (12 μg) and 18% with higher dose formoterol (24 μg). Whether these findings have any functional significance in this small cohort was not clear.
A 12 month follow-up study assessed the effect of arformoterol compared with salmeterol in a cohort of 813 COPD subjects (GOLD class 2-4, mean FEV1 of 1.2 L; 39% predicted). 39 The subjects from this cohort were recruited from the large group of 1456 from the first 2 trials. A dose of arformoterol of 50 μg daily was compared with a dose of salmeterol 84 μg. The results demonstrated an improvement in trough FEV1 at 13 weeks which was sustained out to 52 weeks (6% for both treatments). There was no development of tolerance in this trial; arformoterol was no more effective than salmeterol though. As with the previous studies there was a marked baseline BD effect of 16% in both groups. The results of published trials are summarized in Table 1.
Published trials of efficacy of arformoterol in COPD.
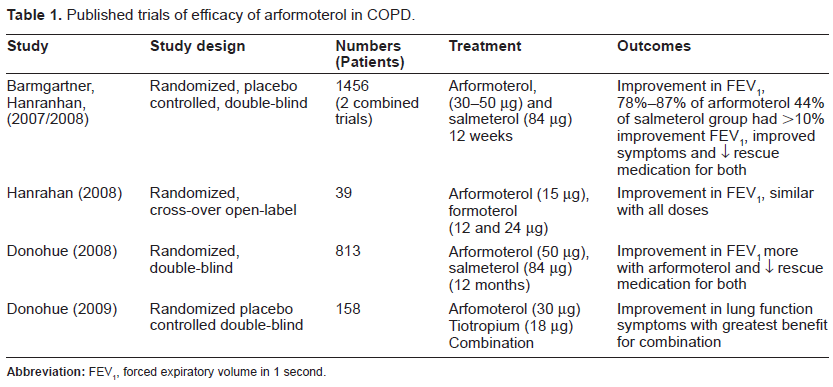
A recent study compared the effect of arformoterol, tiotropium and their combination in COPD patients. 40 This multi-center trial (34 sites) studied 235 patients who were randomized and blinded over a 2 week period. This trial demonstrated significant improvements in FEV1 for both arformoterol (0.10 L) and tiotropium (0.08 L) with maximal effects observed for the combination (0.22 L). Similar effects were demonstrated for improvements in other lung function parameters and clinical status. This trial demonstrated the benefits of combining anticholinergic and β2-agonists which has been demonstrated with other combinations previously. The study duration was brief and as with the previous trials it is not clear if initial airway reactivity affected the results.
Safety
β2-agonists have a variety of effects including tachycardia, hypotension, hypokalemia and hyperglycemia. 41 As a consequence there have been concerns about the use of long-acting β2-agonists particularly in the context of asthma. A recent Cochrane review found that formoterol increased the risk of non-fatal serious adverse events in asthma. 42 In COPD the TORCH trial of salmeterol found there was no increase in mortality over a 3 year period compared to placebo. 43
There have been 6 published studies which have described the use of arformoterol in COPD. These studies have demonstrated that arformoterol has generally been well tolerated with a low incidence of side effects. These studies had a high rate of bronchoreactivity as has been previously described in this review.
In two clinical trials comprising 1456 subjects over a 12 week period arformoterol was well tolerated at 3 different doses.36,37 The patients who received a dose of arformoterol of 15 μg bid and 25 μg bid there was no change in adverse events compared to placebo. In subjects who were taking 50 μg daily there was a 3% increase in mild side effects. There were no major adverse events reported.
A follow-up study was performed in this cohort to assess the risk of arrhythmias with the use of salmeterol and arformoterol. 44 This study found a high incidence of atrial tachycardias (42%) in this cohort prior to the initiation of β2-agonist use. Twenty four hour Holter monitoring was performed at week 0 (first day of dosing), 6 and 12. There was a total of 5226 Holter recordings in 1429 patients. The use of LABAs (both salmeterol and arformoterol) increased the risk of atrial arrhythmias by 2%-5% (not significant) with no effect on more serious cardiac manifestations. Whilst this study demonstrated safety this cohort has a high incidence of co-existent cardiac disease. The safety of LABAs as maintenance therapy in patients with known cardiac disease has still not clearly been established as the follow up data is only of short duration.
A study of 39 patients treated for 2 weeks frequent occurrence of minor respiratory side effects (−30%). 38 Tashkin et al studied 235 patients over a 2 week period 40 and reported no major incidence of side effects. As both these studies were only of brief duration it is hard to draw any firm conclusions.
The most definitive study of safety was performed by Donohue et al 39 who studied 813 patients over a 12 month period and compared the use of salmeterol with arformoterol. A major weakness of this study was the lack of control arm and as such it is difficult to interpret. There was on clear difference in side effects between the two β2-agonists. Twenty two % of subjects in the arformoterol group and 17% of subjects in the salmeterol group had to discontinue the trial due to side effects. A number of side effects are listed (e.g. infection, COPD) but without a placebo arm it is hard to interpret what they mean.
Place in Patient Therapy
Arformoterol can only be given by nebulizer and is currently approved by the Federal Drug Administration for the use of maintenance therapy in COPD. The patients who are most likely to use this medication are those who are unable/not motivated to use a dry powder inhalation or metered dose inhaler. Such potential groups may include those with poor dexterity, those who have poor inhalation technique and patients with reactions to propellants. The nebulized route may be indicated for patients who have ongoing symptoms despite DPI/MDI use and those with severe disease. 45
Fomoterol fumarate has been recently developed which can also be given by nebulizer. A study of 569 subjects over 12 months demonstrated safety and modest benefits in COPD subjects. 46 It is not clear if there is any difference between this medication and arformoterol.
Arformoterol may be given once a day (at a dose of 50 μg daily) and this may be easier for patients to manage. There has been recent interest in the use of ultra-long acting β2-agonists. 47 Whether this is a potential benefit has not been described in recent publications.
As arformoterol is comprised of the (R,R/R,R) isomers whilst formoterol is a (R,R/S,S) racemate it may have more potent effects, although this has not been definitively proven in the available literature. In vitro data suggests that the arformoterol may have a particularly efficacious anti-inflammatory effect but this action has not yet been tested in published trials. As such one potential important use of arformoterol may be in the treatment of exacerbations of COPD.
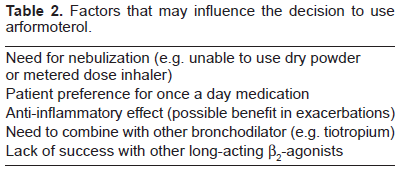
Patients with COPD may benefit from combined bronchodilator therapy. Bonasia et al described arformoterol as being compatible with 3 other nebulized medications; acetylcysteine, ipratoprium bromide and budesonide. 48 The effect on lung function was not assessed. Another study has demonstrated the benefit of combining tiotropium and arformoterol. 40 The combination of long acting agents to give once daily dosing may be beneficial. 47 Factors that may influence the decision to prescribe arformoterol are listed in Table 2.
Factors that may influence the decision to use arformoterol.
Conclusions
Arformoterol is a long-acting β2-agonist that can only be given by nebulizer and has been approved for maintenance therapy of COPD. It is comprised of the 2 active isomers of formoterol (R,R/R,R) and may potentially be more potent than racemic (R,R/S,S) formoterol at least in an in vitro setting. As arformoterol is a new drug the literature concerning its use is still fairly preliminary.
There have been 5 clinical trials that have assessed efficacy all of which have been randomized and blinded. The results have demonstrated that arformoterol was effective in improving lung function mainly FEV1 and symptoms. All of these trials have been performed by the same group and there was a high prevalence of baseline airway reactivity which may compromise the results. It was not clear whether arformoterol has any clear benefits over other LABAs.
Trials have demonstrated that arformoterol appears to be safe in the data available. However there was no placebo controlled trial with a follow-up longer than 12 weeks so this issue needs to be further clarified. Subjects with COPD do appear to have a high incidence of atrial arrhythmias and the safety of arformoterol in those with co-existent cardiac disease has not been established.
The main use of arformoterol is in those subjects who are unable to use DPI or MDI preparations. The use in combination with tiotropium is beneficial. One potentially important use may be in the treatment of acute exacerbations.
Disclosure
The author reports no conflict of interests.