
Abstract
Although multiple new agents for the management of diabetes have become available in the past decade, less than 50% of diabetics in the United States have Hgb A-1-C levels below 7.0% and far fewer at the newer more stringent targets of 6.0% to 6.5%. It has become increasingly clear that the course of Type 2 diabetes is marked by progressive loss of beta-cell function in the setting of relatively fixed insulin resistance. However, treatment algorithms are based on initial monotherapy, usually with metformin, and only move to combination or add-on therapy when treatment has failed and disease has progressed. Few therapeutic agents address both insulin resistance and beta cell function, and no monotherapeutic agent fully addresses any physiologic defect. Metformin, a well-established therapy for diabetes is effective in reducing hepatic and to a lesser extent muscle insulin resistance primarily through AMP-kinase activation, but has only modest effects on long-term beta-cell function. Pioglitazone, an agent in the thiazolidinedione (TZD) class has mechanistically distinct effects on hepatic, muscle and adipocyte insulin resistance, primarily through PPAR-gamma activation, as well as having somewhat greater effects on beta-cell function and durability of glycemic control. The combination of the two agents, either as initial therapy, or as very rapid add-on therapy for the patient who does not achieve target glycemia soon after initiation of metformin is a mechanistically favorable and useful approach to early and durable glycemic control of many new-onset diabetic patients. The efficacy of both metformin and pioglitazone as monotherapy has been well-documented in numerous studies, and combination studies have demonstrated superiority in efficacy of combination therapy over monotherapy with either agent as well as superiority in durability of response over non-TZD based combinations such as sulfonylurea/metformin. Safety issues with metformin remain primarily tolerability based on GI side effects with the rare risk of lactic acidosis in patients with declining renal function. The safety of the TZD class, while well-documented, does carry the risks of volume expansion and resultant CHF, as well as weight gain, which while troublesome, uniquely does not impair glycemic control in these patients. A more recent concern has been raised regarding fracture risk and decreased bone density, and although the relative impact appears small it remains relevant. These risks may be somewhat balanced by more recent studies suggesting a favorable effect of pioglitazone on multiple metabolic risk factors for CVD such as lipids, C-reactive protein, and adipocytokines such as adiponectin. Recent mechanistic and outcome studies such as PROACTIVE and PERISCOPE which suggest there may also be modest benefit on plaque progression and CVD outcomes. Metformin has beneficial effects on metabolic CVD risk factors, such as triglycerides, insulin and PAI-1 and there is a persistent signal of favorable CV outcomes in metformin treated patients. This review will address the safety and efficacy of the agents as monotherapy as well as in combination, and explain the physiologic rationale for earlier or initial use of pioglitazone/metformin combination therapy for newly diagnosed diabetes as well as the long term potential benefit for ongoing management of the treated diabetic.
Keywords
Introduction
Type 2 diabetes, a chronic progressive disorder of glucose metabolism associated with significantly increased risk of cardiovascular morbidity and mortality, is rapidly becoming a major health issue globally with an estimated 5% of the world population affected in 2005. In the United States, 7% of the population has diabetes, with an equal number diagnosed with impaired glucose tolerance. The most rapid growth in prevalence is occurring in the 16-45 year age group, paralleling the increase in overweight/obesity. 1 The diagnosis of diabetes is preceded by progressive hyperglycemia for up to a decade or longer before clinical diagnosis is made, and both microvascular and macrovascular complications are not uncommon in this prediabetic or newly diagnosed population,2,3 suggesting that current guidelines for initiation of treatment may not recognize the physiologic state of the patient at diagnosis.
Type 2 diabetes is physiologically characterized by progressive beta-cell dysfunction in the setting of relatively fixed insulin resistance. 90% of type 2 diabetics are insulin resistant, but the degree of insulin resistance is nearly maximal by the time patients reach IGT. 4 Subtle changes in adipocyte function may worsen peripheral insulin resistance modestly causing further deterioration in glycemic control, but only in the setting of impaired or deficient beta-cell response. The degree of relative beta-cell dysfunction in early diabetes has long been appreciated, with absolute hyperinsulinemia common at diagnosis but still relative insulin deficiency in that blood glucose remains elevated. However, data from the UKPDS and more recently from the San Antonio Metabolism study 5 have suggested that absolute beta-cell function has declined 50% in early IGT and that at diagnosis, as much as 80% of beta-cell function may have been lost. This suggests a more advanced disease state than is clinically apparent from glycemia, making current treatment paradigms somewhat discordant from disease state. Additionally, UKPDS 16 offered the insight that loss of beta-cell function is an intrinsic and progressive part of the disease process of diabetes and was not therapeutically well-addressed over the course of the study with monotherapeutic metformin, sulfonylurea or insulin therapy.
Current treatment guidelines reflect the older understanding of the disease state, initiating disease management with metformin, an effective, safe and inexpensive therapy for insulin resistance, but an agent without significant beta-cell modulating effects. Drugs such as thiazolidinediones or incretin based therapies which do have effects on beta-cell function and a suggestion of durability of effect are currently relegated to second line or late add-on therapy. This often occurs after further deterioration of the beta-cell functionality, minimizing their clinical effectiveness. Pioglitazone, a thiazolidinedione (TZD) improves insulin sensitivity at liver, muscle and adipocyte primarily through PPAR-gamma activation and increased tissue fatty acid oxidation. 6 Metformin improves insulin sensitivity though activation of the AMP-kinase pathway. 7 Its actions are primarily at the liver with additional, but lesser effects on muscle, and with little adipocyte sensitization. This suggests a potential additive and synergistic effect on insulin resistance when these drugs are combined. 8 Pioglitazone, unlike metformin, has demonstrated physiologic effects on beta-cell function and theoretically may conserve beta-cell mass, resulting in durability of glycemic effect. This combination of reduced beta-cell work and enhanced beta-cell function although as yet unproven, is mechanistically superior to other combinations in addressing the dual defect present in early and ongoing diabetes. The purpose of this review is to examine the pharmacology of these two agents singly and in combination in the context of current understanding of the diabetic disease state and address the safety, efficacy and potential long-term benefits of combined pioglitazone/metformin therapy in treating diabetes and potentially upon diabetic cardiovascular complications.
Metformin and Pioglitazone: Pharmacology and Efficacy
Metformin, a biguanide agent acts primarily as an insulin sensitizer. Its primary clinical site of action is in the liver, improving hepatic insulin sensitivity and as a result, decreasing hepatic gluconeogenesis. Metformin may also increase both hepatic and splanchnic glucose utilization. Metformin also has significant effects on peripheral insulin sensitivity, primarily at muscle and modestly at adipocyte by phosphorylation and activation of AMP-activated protein kinase. 9 Therefore, reductions in blood sugar with metformin occur in the setting of reduced insulin levels and theoretically reduced beta-cell work. There appears to be little or no direct mechanistic effect of the drug, however on beta-cell function or apoptosis. Metformin is neglibly protein bound and is primarily renally cleared, proportionate to declines in creatinine clearance. Therefore dosage reduction or therapeutic restriction may be required in the aging or renally impaired patient.
Pioglitazone, a member of the thiazolidinedione class, is a potent peroxisome proliferator-activated receptor (PPAR)-gamma receptor agonist. PPAR-gamma is a ligand coactivated transcription factor involved in glucose and lipid metabolism. Pioglitazone also demonstrates modest PPAR-alpha activation, a similar transcription factor involved in lipid metabolism and fat oxidation. PPAR-gamma receptors are also richly expressed in the vasculature, the adipocyte and in macrophages and may play an important role in non-metabolic modulation of inflammation and atherogenesis. 6 The result of PPAR activation by thiazolidinediones is the expression of over 200 genes, approximately 1/3 of which are unique to a given agent. The lipid effects and cardiovascular and hepatic safety of pioglitazone appears to be due to its drug specific gene-activation profile. PPAR activation increases insulin sensitivity through several mechanisms distinct from that seen with metformin, although there is evidence that insulin sensitivity with pioglitazone may also be partially enhanced by AMP-kinase activation as well. PPAR active drugs increase intracellular fatty acid oxidation, reducing intracellular lipid and diacyl glycerol levels, improving insulin signaling. This effect may be enhanced by or due to an increase in circulating adiponectin, an adipocytokine which increases peripheral fat oxidation and decreases vascular inflammatory responses. 10 Adiponectin levels increase by approximately two-fold in response to PPAR-gamma activation, but it unclear how much of the improvement in insulin sensitivity is as a result of adiponectin action in humans. Pioglitazone significantly reduces hepatic gluconeogenesis to a degree similar to metformin, and improves muscle glucose uptake significantly as well. As myocytes do not express significant PPAR-gamma receptor activity, is is suggested that improvement in muscle insulin sensitivity is mediated by decreased intramyocellular lipid, a potential TZD mechanism. Hepatic insulin sensitivity and lipogenesis may further result from this improved peripheral postprandial glucose disposal as well. 11
Unique to the TZD class in the treatment of diabetes is the impact on adipocyte insulin sensitivity. 12 PPAR-gamma activation is an important modulator of fat cell function, and appears to have a direct impact on improving both visceral and subcutaneous fat cell insulin sensitivity. Effects on visceral fat may be mediated both by direct cellular PPAR effects, but also by PPAR induced reductions in macrophage-mediated inflammation, an essential modulator of visceral adipocyte function and sensitivity. 13 It has been proposed that sensitization of the subcutaneous adipocyte results in increased uptake of circulating free fatty acids and potential improvement in peripheral insulin sensitivity. 14 Enhanced visceral adipocyte insulin sensitivity also results in reduction of lipolysis and free fatty acid flux to liver potentially improving hepatic insulin sensitivity as well.
However while this decrease in circulating ffa may play a role, the reduction in intramyocellular and intra-hepatic fat seen with TZD therapy may have a more significant impact on both hyperglycemia and hyperlipidemia. 15
The attractiveness of combined or early aggressive use of oral therapy for type 2 diabetes rests on the presumed impact of treatment on beta-cell function. Terms such as beta-cell function, protection and preservation are used freely with varying definitions used by investigators. In this discussion it is important to remember several factors. Models such as HOMA and QUICKI that examine beta cell function based on insulin and glucose measurements measure the functioning of beta cells, but offer no insights as to the intrinsic “wellness” or longevity of beta cells. Sulfonylureas for example show improvements in HOMA-B beta cell function, but clinically lose effectiveness over time. A temporal component is needed to make modeled effects on function relevant for chronic disease management.
Function may be better assessed not by insulin output but by measures of beta-cell health, such as restoration of first phase insulin secretion, decreases in proinsulin/insulin ratios and restoration of normal oscillatory secretory patterns. These markers however do not provide any insights into beta cell longevity or clinical therapeutic efficacy. In the ADOPT trial, rosiglitazone showed greater durability of glycemic response than metformin yet did show an ongoing decline in beta cell function(2% vs. 3%). 16 The most important issue to consider in any discussion of beta-cell effects on therapy is that no human data exists and all anatomic correlates on beta-cell anatomy, mass and potential regeneration/decrease in apoptosis come from rodent models and therefore cannot be directly extrapolated to human physiology and more importantly therapeutics.
The attractiveness of pioglitazone therapeutically rests not only with its insulin sensitizing properties, but its apparent impact on beta cell function. Human studies have demonstrated favorable mechanistic effects of TZD therapy on restoring physiologic insulin secretory oscillations, 17 near-normalization of proinsulin/insulin secretion, 18 and restoration of first phase insulin secretion. 19 In rodents, pioglitazone has been shown to enhance islet cell mass and restore normal organelle structure and function. 20 The mechanism of potential beta-cell modulation is unclear but is likely substantially due to direct PPAR activation at the beta cell.21,22 The reduction of intra-beta cell lipid (i.e. lipotoxicity) plays an important role in enhanced beta-cell function and survival and is mediated by PPAR activation, although increased adiponectin may play a role as well. TNF-alpha and IL-6 also play a role in decreasing insulin autoregulation of the beta cell,23,24 thereby potentially decreasing beta cell function although the relative clinical contribution of this pathway is unknown.
Based on these mechanisms of drug action, there is little overlap between metformin and pioglitazone. the combination of the two drugs should demonstrate more potent insulin sensitization than either drug alone, with the additional benefit of beta cell “protection” and enhanced durability of drug effect. Most studies, however have examined pioglitazone added to existing metformin therapy, and little data exists on the therapeutic response when the two drugs are initiated simultaneously. Although standard clinical practice has remained step care with add-on therapy, there is a suggestion that there is a greater therapeutic response to pioglitazone when initiated with, not subsequent to metformin in naïve to treatment patients. 25
Homeostasis Model Assessment (HOMA) modeling validates the individual and combined actions of the two drugs on insulin resistance and beta cell function, though it better reflects changes in beta-cell performance than restoration of intrinsic normal function. The literature regarding HOMA-IR and HOMA-B for metformin and pioglitazone individually and in combination is best looked at in aggregate, as individual studies using HOMA modeling have shown widely disparate and contradictory effects on insulin sensitivity and beta cell function. For example, Pavo 26 failed to demonstrate any improvement in HOMA-IR with metformin in newly diagnosed diabetic patients despite similar glycemic efficacy to pioglitazone, a mechanistically inconsistent observation. However, in each study of combined therapy a consistent improvement in both HOMA-IR and HOMA-B were demonstrated when the two drugs were combined. Einhorn 27 and colleagues showed a 16% reduction in insulin resistance when pioglitazone was added to existing metformin therapy over a 16 week trial, compared to a 17% increase with placebo. Hanefeld et al 28 studied combined pioglitazone/metformin therapy v pioglitazone/glibenclamide over a much longer duration of 3.5 years. The pio/metformin group had an initial increase in insulin sensitivity of 42% which was sustained throughout the study, whereas the metformin/SU group had a 32% decline over time and the difference was significant 6 months after initiation of therapy. This would suggest that this combination may afford durable effects on glycemic control through a sustained reduction in beta cell workload. Although improvements in beta cell function are consistent, this does not reflect long-term changes in beta cell health, plasticity and turnover, and studies directly addressing the physiologic status of the beta cell with pioglitazone/metformin combination therapy are lacking.
The therapeutic efficacy of pioglitazone as addon therapy to metformin in patients with inadequately controlled diabetes has been evaluated for periods up to 3.5 years. (Table 1) However, there is little data comparing the initiation of the combined drugs as initial therapy for newly diagnosed disease to sequential implementation after therapeutic inadequacy with metformin monotherapy, and the two conditions may reflect somewhat different states of beta-cell sufficiency and responsiveness to treatment. Einhorn and colleagues studied 328 patients with HgbA1c of greater than 8.0% to receive either 30 mg of pioglitazone or placebo added to their existing metformin therapy. Dose titration to 45 mg was permitted if glycemic control was unacceptable. At study end the difference between study groups was −0.83%. the open label phase extended 72 weeks with a sustained reduction of HgbA1c of −1.36%.
Combination trials of pioglitazone/metformin.
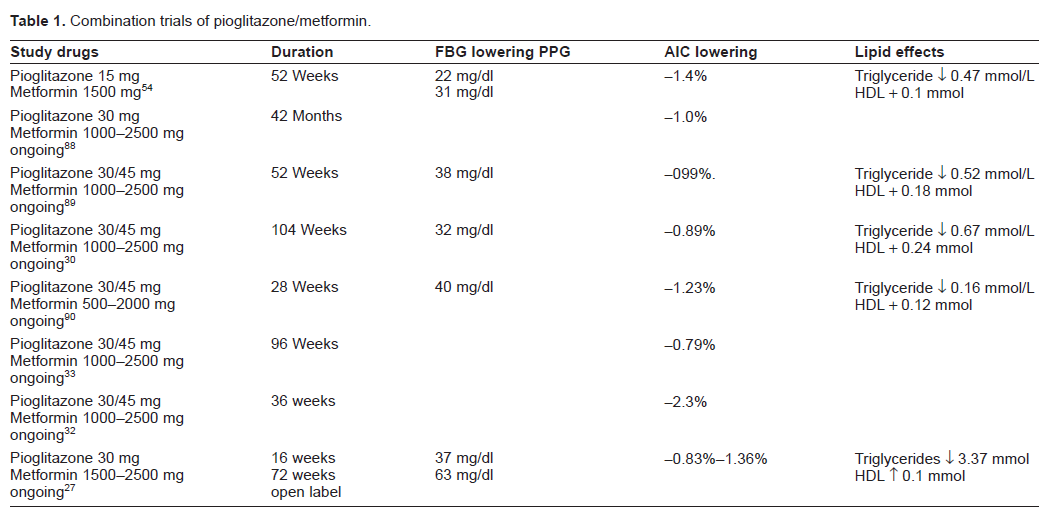
The effectiveness of combination therapy may be more clinically significant for long term management of diabetes when pioglitazone/ metformin is compared to sulfonylurea/metformin combinations. 29 Charbonnel et al 30 compared the addition of pioglitazone vs. glimepiride to patients failing metformin therapy. After 2 years, the A1c lowering was −0.89% in the pioglitazone group and −0.77% in the SU group, not statistically significant. However, among patients who completed 18 months of therapy, reduction of A1c from baseline was significantly lower in the pioglitazone/metformin group −1.07% vs. −076% in the sulfonylurea group, reflecting in some fashion the gradual rise in blood glucose seen in UKPDS after 12-18 months on sulfonylurea monotherapy. 31 Further evidence that pioglitazone may confer enhanced durability of glycemic control when added to metformin comes from 2 prospective long-term trials. Spannheimer 32 et al demonstrated that at 3 years A1c lowering with pioglitazone/metformin was −2.3% when compared to −1.8% in the glibenclamide/metformin group. Oerter 33 showed a non-significant difference in A1c of −0.79% in the pioglitazone treated group vs. −0.61% in the glibenclamide group, but among patients who responded to combination therapy who required no additional treatment for glycemic control, the difference was significant at 96 weeks −0.85% vs. −0.61%.
The dosages of these agents singly is slightly different from the fixed-dose combinations currently available in the United States. Pioglitazone as monotherapy may be titrated to a maximum dose of 45 mg. Although there is a statistically significant incremental improvement in glycemic control, the incidence of side effects, primarily weight and edema increases at this dose and should be used only after patients are close to but not yet at therapeutic target. The therapeutic dose of metformin ranges from 1000 to 2500 mg, with only modest improvements in efficacy at doses greater than 1700. The fixed dose combinations available in the United States reflect those observations with tablets containing 15 mg of pioglitazone combined with either 500 or 850 mg of metformin. Combinations of pioglitazone with higher doses of sustained release metformin remain in development.
Safety of Metformin/Pioglitazone
The safety of both metformin and pioglitazone have been exhaustively studied in the past decade, driven primarily by significant adverse events reported with troglitazone and to a less well documented extent with pioglitazone. The primary safety concern with metformin remains the rare occurrence of lactic acidosis in patients with renal or hepatic dysfunction and caution has been advised in patients with congestive heart failure. However Masoudi 34 et al have noted improved clinical outcomes in patients with CHF treated with metformin suggesting that the benefits of insulin sensitization outweigh the rare risk of lactic acidosis in this population. Tolerability of metformin is a greater issue than safety with up to 10% of patients experiencing gastrointestinal side effects sufficient to modify adherence with the medication.
The safety issues with pioglitazone are complex and in some cases poorly defined and even less well mechanistically understood. The fundamental issue in examining safety with TZD therapy is discerning class effect versus drug specific effect given the lack of complete overlap in gene activation between the four TZD drugs that have been well characterized. 35 The safety issues can be categorized as hepatic, volume overload (edema, CHF), cardiovascular and bone. Although the weight gain seen with TZD therapy has been listed as a safety/side effect issue, it reflects PPAR-gamma improvement in adipocyte function and lipogenesis, as well as potential fat redistribution subcutaneously. 36 Unlike weight gain seen with other diabetic therapies, this fat accrual is not associated with a decline in glycemic control. Additionally, weight gain often parallels the glycemic response, likely reflecting the degree of PPAR activation. 15 Both Charbonnel 37 and Kawai 38 have noted that the addition of metformin to pioglitazone attenuates the weight gain seen with pioglitazone alone, likely due to satiety and caloric intake effects, and the initiation of the two drugs simultaneously in combination may reduce clinical weight concerns. Volume expansion can be a cause of weight gain in some patients due to PPAR effects on sodium reabsorption and the development of edema. These studies suggest that rapid weight gain on the combination may therefore reflect significant volume expansion not fat accrual, and those patients need to be evaluated for that safety concern.
Volume expansion is a class effect of TZD therapy, mechanistically reflected by a combination of vasodilatation but a more significant sodium retention at the renal tubule induced by PPAR-gamma mediated insulin sensitization. This anti-natriuresis results from activation of Na+/K+ pump in the distal collecting tubule, and is enhanced in the presence of hyperinsulinemia due to exogenous insulin therapy and drugs such as non-steroidals that decrease natriuresis. The edema seen with TZD therapy reflects both this volume expansion and calcium channel blocker like vasodilatation, but is most commonly seen in patients with lower creatinine clearance and may reflect advanced endothelial dysfunction and extravascular extravasation of fluid. The incidence of edema ranges from 3% overall to 20% in insulin treated patients. 39 This edema, while effectively treated by drugs that block Na+/K+ exchange such as amiloride or spironolactone, responds less well to loop diuretics or hydrochlorothiazide. 40 The volume expansion linked to CHF, however, is responsive to these agents suggesting a somewhat different mechanism for edema and CHF. The CHF safety concerns will be reviewed later in this monograph.
Hepatic safety was a significant concern with troglitazone, prompting its removal from the market. Extensive post-marketing surveillance of hepatic safety with pioglitazone has showed no increase in hepatotoxicity, 41 and the use of pioglitazone in the treatment of NASH is currently under study with preliminary reports suggesting benefit. However, while the use of metformin in NASH would be safe, the use of combined pioglitazone/metformin in patients with relatively advanced hepatic dysfunction of any cause would be contraindicated. Hepatic function should be monitored once after initiation of therapy and then as clinically indicated, but no increased risk of hepatotoxicty has been observed with statin use. As pioglitazone is metabolized via CYP2C8/9 and CYP3A4, coadministration of drugs that inhibit these pathways such as gemfibrozil, a common hypolipidemic treatment should be minimized due to an increase in pioglitazone levels.
A more recent and potentially troubling long-term safety issue are recent reports of increased fracture risk and decreased bone density with both TZD drugs. 42 The ADOPT trial with rosiglitazone demonstrated a small but significant increase in leg and forearm fractures. 43 Pioglitazone post marketing analysis has also confirmed an increase in distal fractures in women of the hand, foot and humerus, somewhat different than the usual sites for post-menopausal or glucocortcoid induced fractures and sites high in cortical, not trabecular bone. Data from the ADOPT trial and subsequent metanalyses suggest an increase in relative fracture risk of 1.2-1.8. The effect on fracture is predominantly in women and appears to be associated with a rather rapid loss of bone density in the first 12 months of therapy, with a slower annual loss observed therafter. 44 Mechanisms for the decreased bone density are based on a decrease in bone formation but apparently no effects on bone resorption. PPAR-gamma stimulation of marrow mesenchymal cells into adipocytes rather than osteoblasts is a proposed mechanism for decreased bone density, 45 as increased marrow fat is observed in TZD treated patients, much as is seen in older adults. 46 However, additional studies have demonstrated decreased bone density on DEXA bone densitometry although the increased adiposity of marrow may falsely decrease DEXA readings. However, given the increased fracture rate seen, women at high risk for fracture or osteopenia should be treated with these drugs only when clinically preferable, and vitamin D status and calcium intake assessment should be an essential part of diabetes management when on pioglitazone treatment.
Cardiovascular Effects of Metformin and Pioglitazone
The cardiovascular (CV) effects of metformin and pioglitazone can be examined in four areas: impact on dyslipidemia, impact on atherosclerotic risk factors and plaque formation, impact on CV clinical outcomes and issues of cardiovascular safety. The bulk of the literature studies the CV effects of each drug individually, and few studies examine the additive effects of the two drugs when used in combination. The lipid and CV effects of metformin and pioglitazone monotherapy have been extensively discussed elsewhere 47 and this section will focus on potential synergistic impact of combined therapy. Metformin has been shown to have a modest but important impact on dyslipidemia. Mechanistically metformin reduces circulating free fatty acids (ffas) by 10%-20% and lowers triglycerides by 10%-15% (Kirpichnikov). The reduction in VLDL is due to decreased hepatic VLDL synthesis and a very small reduction in LDL cholesterol and a clinically insignificant increase in HDL is also seen. Of potential mechanistic import is the effect of metformin on reducing oxidative stress within the arterial wall. 48 This reduction in lipooxidation reduces oxidized LDL concentrations within plaque and may contribute to an enhanced beneficial CV effect.
The favorable lipid effects with pioglitazone are unique to this TZD and are not shared by rosiglitazone. Differential adipocyte gene activation by pioglitazone compared to rosiglitazone at the adipocyte might account for some of the observed effect. 49 A meta-analysis by van Wijk 50 as well as a randomized prospective trial (GLAI) by Goldberg 51 and colleagues have documented a rather substantial differential lipid impact between the two TZD drugs. Ginsberg postulates an increase in VLDL clearance with pioglitazone as a potential mechanism for the lipid lowering rather than a differential effect on lipid synthesis. 52 However, Al Majali 53 describes a primary impact of pioglitazone on hepatic lipase activity rather than on lipoprotein lipase, and differential effects of hepatic lipase could explain differences between rosiglitazone and pioglitazone on particle size and LDL particle number.
Pioglitazone is associated with a significant reduction in circulating ffa's and a reduction in triglycerides of 15%-20%. HDL increases are consistent but variable and are dependent upon baselines, with very modest increases in HDL when baseline is 40%-50% mg/dl but more robust increases of 10%-30% as levels decline below 35 mg/dl. LDL levels increase with both TZD agents, but the increased LDL seen with pioglitazone treatment is associated with an increase in LDL particle size and therefore a decrease in small dense LDL, a more atherogenic form of LDL. A decrease in LDL particle number and apoB is seen as well. 50
There are a number of studies looking at the additive effects of the two drugs when used in combination and few looking at lipid impact when the drugs are initiated jointly. 54 Charbonnel et al 30 compared the lipid effects of add on therapy of pioglitazone to either metformin or gliclazide and found both further reductions in triglycerides and ffas when pioglitazone was added to metformin and superiority of the pioglitazone/metformin combination to the gliclazide combination when the atherogenic index of plasma (AIP) was compared as well. Combination pioglitazone/metformin therapy should be expected to lower triglycerides approximately 10% more and increase HDL 5%-10% more than either agent alone. The magnitude of overall drug effect on lipids remains modest however when compared to glucose lowering and cannot readily explain any significant favorable effect in CV outcomes.
The effect of metformin and pioglitazone on vascular biology and adipocytokines is potentially far more relevant, but still remains only modestly evaluated at the clinical outcome level. Metformin significantly reduces levels of PAI-1, a cytokine associated with both hypercoagulability and plaque destabilization. 55 Levels of PAI-1 are significantly increased within the diabetic plaque and are increased by hyperinsulinemia, hyperglycemia and hypertriglyceridemia. It is not clear however that circulating levels of PAI-1 correlate with plaque PAI-1. Pioglitazone also reduces PAI-1 through similar effects on metabolic parameters, but also reduces PAI-1 by direct PPAR-gamma stimulation of both adipocyte and macrophage, primary sources of PAI-1 secretion. Combination therapy of pioglitazone/metformin is likely to have synergistic effects on hypercoagulability and plaque destabilization in vivo.
Although there is some anti-atherogenic overlap between metformin and pioglitazone, especially through impacts on PI3-kinase mediated mechanisms, the overall effects of pioglitazone on other components of plaque physiology are much greater than and mechanistically distinct from what is seen with metformin. PPAR-gamma activation of the adipocyte is associated with a reduction in proatherogenic and inflammatory cytokines TNF-alpha, IL-6 and resistin. 15 It was initially felt that TZD related declines in these cytokines may mediate the reduction in atherogenesis seen in multiple mechanistic animal models. However, circulating levels of these cytokines do not correlate well with clinical findings and it is becoming increasingly clear that local macrophage induced secretion of these cytokines as well as plaque destabilizing MMP-9 may actually better reflect event risk. Increased ffas appear to activate macrophages both at visceral fat and in the arterial wall, 56 increasing the local inflammatory response and increasing visceral fat cell insulin resistance. The combination of pioglitazone/metformin may therefore have additive effects at the plaque level in reducing inflammation, both by additive reduction in circulating ffa's, but also by direct PPAR-gamma reduction in macrophage activation. 57
The vasculoprotective cytokine adiponectin plays an important role in mediating vascular repair. However it has been shown that metformin has little effect on this cytokine 10 and levels are not substantially changed with combination therapy compared to pioglitazone alone.
It has been suggested in outcome studies that the beneficial CV outcomes seen with metformin and pioglitazone are merely reflective of improvements in glycemic and metabolic control, and do not relate to impact on vascular biology. However in non-diabetic animal models, pioglitazone has been shown to significant retard the development of plaque induced by hyperlipidemia and in an intriguing study by Collins et al significantly reduces angiotensin induced plaque, suggesting the importance of these non-metabolic effects of these drugs. 58 Recent unpublished data (APPROACH Trial) suggesting that rosiglitazone, which has somewhat unfavorable lipid impact, may demonstrate similar plaque effects as pioglitazone suggest that indeed a non-metabolic direct effect in plaque biology is likely. Additionally, a reduction in microalbumin, a marker of cardiac event risk is consistently seen with pioglitazone and is significantly greater than metformin monotherapy despite equivalent effects on glycemia further suggesting a direct vascular effect. 59
Cardiovascular Outcomes
It is difficult to definitively discuss CV outcomes from diabetes agents as the studies as currently published are not designed to examine the mechanistic impact of these drugs on vascular biology. Event driven trials or incident rates of events reflect plaque destabilization and atherothrombosis rather than atherogenesis, the primary CV target for metformin and pioglitazone. Outcome studies that do not run 5-10 years are therefore less likely to define benefit than shorter term studies. Additionally, the impact of PPAR-gamma activation on plaque integrity and stability and therefore event occurrence appears to differ between agents in the TZD class, as PPAR-gamma has both pro and anti atherogenic properties and differential gene activation may lead to a drug specific impact on both plaque and event rates. Metformin has long believed to have favorable CV effects, but this is primarily based on a very small non-randomized subset of obese diabetics in the UKPDS study. 60 This modest benefit disappeared when sulfonylureas are added. Selvin et al 61 conducted a meta-analysis of metformin therapy which suggested that a modest residual CV benefit occurs when metformin is used in diabetes. Inzucchi 62 has demonstrated that metformin may indeed confer modest benefit in the setting of acute MI as well.
There are few studies that directly clinically assess the anti-atherogenic properties of pioglitazone. One of thee first randomized trials was a study by Mazzone et al 63 which suggested a modest decrease/stabilization of CIMT with pioglitazone compared to glimepiride over an 18 month period. While short in duration and small in number, there was a trend towards fewer CV events in this study. This study was mechanistically supported by the PERISCOPE trial by Nissen 64 which through intra-coronary IVUS technique demonstrated stabilization of plaque progression with pioglitazone when compared to glimepiride over 18 months. This study did not demonstrate short-term reduction in events although lack of progression of plaque has been correlated with a reduced long-term CVevent rate. 65
The PROACTIVE trial by Dormandy et al 66 was designed to address the efficacy and safety of pioglitazone in patients with pre-existing CV disease and to date remains the only large long-term cardiovascular efficacy and safety trial with any TZD therapy. PROACTIVE failed to meet its primary endpoints but did document a 16% reduction in secondary endpoints of acute myocardial infarction, stroke and death. In a smaller subset of over 2400 patients who entered the trial with prior acute myocardial infarction, there was a non-statistically significant 28% reduction in recurrent MI and a 19% reduction in overall CV events. 78 The CV benefit seen was independent of any concomitant statin or angiotensin blocking therapy. In retrospect, this study had design flaws which impaired its ability to fully address any potential CV benefits of pioglitazone therapy. The study group was overly heterogeneous, with CV associated but mechanistically disparate diagnoses at entry, and by its event driven design ended prematurely at 36 months, far too short to address any anti-atherogenic effect of the drug. Statin drugs, a far more potent plaque-modifying class have shown in prior CV outcome trials either modest or no benefit at 36 months with significant effects often only demonstrated at 5 years.67,68
The controversial meta-analysis by Nissen 69 suggested that rosiglitazone may carry differential risk of increased CV event rate and led to an exhaustive analysis of TZD cardiovascular safety. The modest CV benefit and non-CHF CV safety profile of pioglitazone was confirmed by several metanalyses and retrospective analyses of prior pioglitazone treated patients. A meta-analysis by Lincoff et al 70 demonstrated a safety profile somewhat dissimilar from rosiglitazone and muraglitazar, but a trend towards fewer CV events overall in each study, again somewhat dissimilar from rosiglitazone and muraglitazar. Subsequent data from the large ACCORD, ADVANCE and VADT trials, all of which were rosiglitazone enriched or exclusively rosiglitazone treated patient populations demonstrated no increased ischemic CV risk with rosiglitazone therapy, but unlike PROACTIVE showed no evidence of any trend towards a reduction in events.71–73
The utility and safety of pioglitazone and metformin in the patient at risk for and with CHF has been well-studied and again clinically misinterpreted. CHF is a concern with TZD therapy with a consistent increase in both systolic and diastolic heart failure being reported (RR 1.7-2.5). 74 In contrast, the Kaiser Permanente database showed no increase in hospitalizations for CHF among TZD users. 75 In a study of elderly Medicare users with class I and class II CHF, Masoudi 34 reported a decreased one year adjusted mortality rate after hospitalization when compared to a non-insulin sensitizing use group, although readmission for CHF was higher among TZD users.
The mechanism for development of CHF remains acute volume expansion in the setting of compromised LV function as these drugs confer no adverse and mechanistically potential favorable effects on the dysfunctional myocardium.76,77 For this reason, the safety of these drugs have not been studied in patients with class III and class IV CHF and should not be used. Safety in class I and class II CHF has been evaluated and pioglitazone may be used in these patients when clinically necessary with appropriate monitoring. In the PROactive trial, an older patient cohort at significant risk for the development of CHF, the incidence of moderate to severe CHF was increased from a baseline 4% to 6%. The one year follow-up showed no increase in death or myocardial infarction despite continuation of the drug in a majority of patients, again suggesting a reversible volume-driven causality. The study design also increased the risk of CHF, as 90% of patients were rapidly titrated to 45 mg of pioglitazone within 1-3 months with one-third of treated patients on concomitant insulin therapy, a potent volume expanding scenario. The combination of pioglitazone/metformin offers a unique mechanistic and clinical opportunity to both capture potential benefits of insulin sensitizing therapy in these high risk patients while minimizing CHF. If indeed the data that combined pioglitazone/metformin therapy is associated with little or no weight gain, then the patient on this regimen who is accruing weight at a rapid or progressive rate must be evaluated for volume expansion. This is directly in contrast with the clinical assumptions that weight gain is lifestyle driven fat accrual and adjustment of the TZD dosage needs to be considered. The volume expansion is far greater with 45 mg than lower doses, and unless clinically warranted should not be considered in patients with potential LV compromise.
Discussion
A review of pioglitazone/metformin as therapy in 2009 does not pose the question of the use as a therapeutic combination in a step-wise approach, as this has been well validated in the step care algorithms put forth on 2 occasions by the ADA/EASD.79,80 With the availability of combination tablets of pioglitazone/metformin, the clinical question is should this combined agent be used as initial therapy or as a single agent add-on to existing sulfonylurea or incretin based therapy at step 2, rather than as two single agents. The pathogenesis of Type 2 diabetes requires the presence of both significant insulin resistance as well as even greater beta-cell dysfunction, with both UKPDS as well as the San Antonio Metabolism study suggesting a loss of 50%-80% of beta-cell function at diagnosis. No single therapeutic agent effectively treats either or both mechanistic defects fully and therefore combinations of agents are required in the vast majority of patients over time. The initial ADA/EASD algorithm, built along a step-care approach failed to recognize that step care models are effective in intrinsically static diseases that may worsen, but not intrinsically progress such as hypertension or asthma. These models are less successful in disease states that demonstrate progressive dysfunction such as diabetes where the need for next step therapy may reflect either a poor mechanistic intervention in an individual patient or may simply reflect progressive beta cell dysfunction. Bagust and Beale 81 argue that current models of diabetes progression do not adequately predict therapeutic effectiveness as they are based on present assumptions that rates of beta cell dysfunction are linear and occur in an essentially homogenous patient population. Instead their models suggest the rate of beta-cell loss is highly heterogeneous and that the degree of beta cell function at diagnosis may be higher in some patients than others. Given the lack of effective clinical markers other than early therapeutic success and absence of signs of long-term complications at diagnosis, initiation of combination therapy as either initial treatment or rapid add-on may more effectively address the heterogeneity of the patient population at diagnosis. The ADOPT trial was initially interpreted to show significant superiority of rosiglitazone vs. metformin and glyburide over 5 years of monotherapy. Careful reinterpretation of these results actually argues against monotherapy as treatment despite greater beta-cell impact of the TZD. The study definition of therapeutic failure as a fasting blood glucose of 180 mg/dl would never be used in the clinical setting, and therefore the number of patients at glycemic target even at shorter-term assessment is not likely to be satisfactory. Additionally, even with rosiglitazone, modeled beta cell function still declined at a significant rate, albeit less so. Although not part of this study, the ongoing loss of beta-cell function would suggest further slowing of rate might have been more possible had rosiglitazone and metformin been combined. Even if combination TZD/metformin had no additional direct beta cell impact, the further reduction of insulin resistance with these 2 drugs could enhance durability of glycemic control in the setting of slowed beta-cell loss and additional improvement in insulin resistance. Future studies comparing incretin/metformin to thiazolidinedione/metformin combinations may help elucidate the relative impact of beta cell focused vs. insulin sensitizing therapy on disease progression.
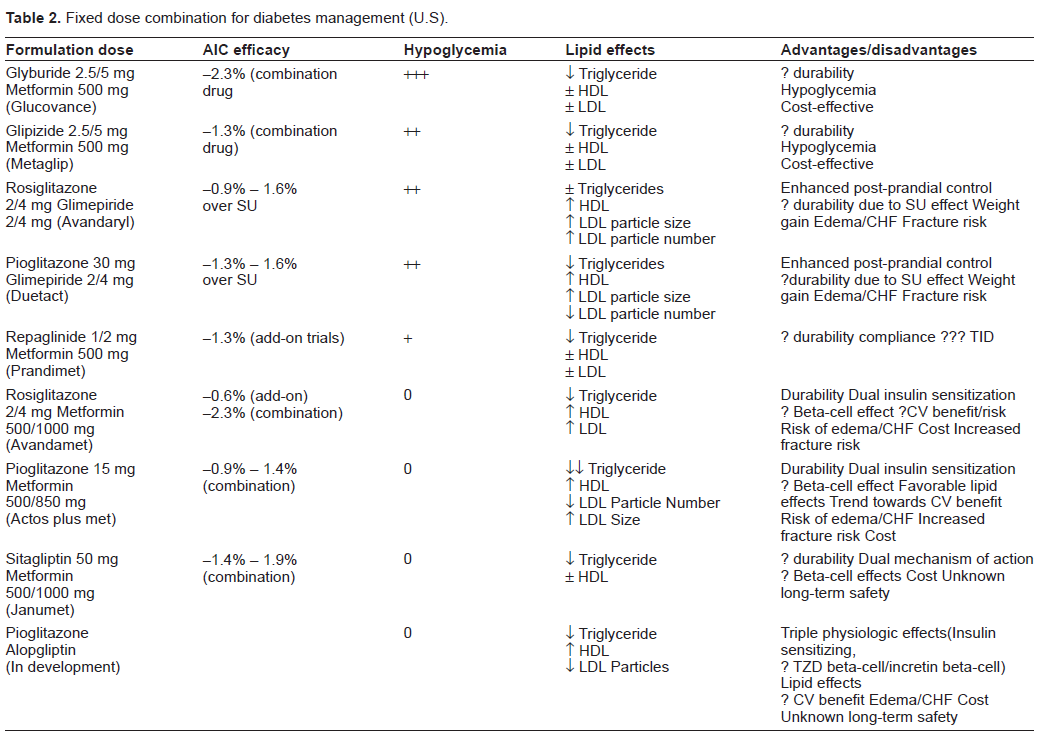
In the second iteration of the ADA/EASD guidelines, combinations were broken down into well-validated therapies vs. less well-validated therapies, with the combination of pioglitazone/metformin considered less-well validated, despite numerous studies suggesting superior efficacy and durability to the “well-validated” metformin-sulfonylurea therapy. 80 Rather than relying on consensus opinion, combination therapy should be looked at as well-validated mechanisms of disease vs. less-well validated mechanisms. Multiple combination agents are available for treatment of diabetes in the United States, but most studies looking at glycemic efficacy of combined therapy are based upon sequential use of the combined drugs rather than initial combination therapy in drug naïve patients. (Table 2) Consideration should be clinically and mechanistically driven with combination therapy chosen based on individual need for more aggressive treatment of insulin resistance vs. need for more aggressive beta-cell and postprandial effect. Chalmers 82 has demonstrated that when started within 3 months of diagnosis, pioglitazone/metformin was associated with a rise in A-1-C of 0.1% per year over 3 years compared to 0.5%/yr in the gliclazide/repaglinide group. The Texas diabetes board which oversees the care of a heavily ethnic and more rapidly disease progressive population has mandated initiation of combination therapy for all patients with a Hgb-A-1-C of greater than 6.5, recognizing the need for aggressive and early control in a more difficult patient population and the need for rapid stabilization of the disease. These guidelines await outcome validation but offer a strong rationale for combination therapy in a high risk population.
Fixed dose combination for diabetes management (U.S).
The cost effectiveness of pioglitazone/metformin therapy has always been an issue in the United States, although generically available pioglitazone will be available in 2011-12. Neeser 83 examined the cost effectiveness of combination of pioglitazone/metformin therapy and found a modest increase in modeled life expectancy and an incremental cost-effectiveness ratio of 47636 euro per life year gained vs. sulfonylurea/metformin. Coyle 84 reported in a Canadian cohort an incremental cost per life year gained of 42000 CD of pioglitazone vs. sulfonylureas though no combination data was available. Conversely Watkins 85 showed significant cost superiority of exenatide vs. pioglitazone. In aggregate the data suggest only modest cost effectiveness of pioglitazone/metformin based regimens, unless subsequent study substantiates a lower rate of disease progression or more favorable long—term CV outcomes with these agents.
Pioglitazone/metformin combination therapy should continue to be looked at as two drugs from a safety perspective. Therapeutically the combination should be viewed as a single agent that significantly reduces both hepatic and peripheral insulin resistance through additive mechanisms and brings the enhanced beta-cell functionality of thiazolidinediones to the modest beta cell effects of metformin. The favorable impacts of this drug on dyslipidemia as well as the mechanistically attractive and potentially clinically favorable CV effects of both drugs may over the long-term provide additional benefits to the diabetic patient as well. Safety issues of CHF and decreased bone density should be monitored and assessed individually in the patient at risk for these complications. With the earlier age of diabetes onset and the needed push for earlier and more aggressive treatment of all diabetic patients, more long-term observations will be of great importance.
The other question that must be addressed is if these combined drugs behave differently when initiated simultaneously in newly diagnosed disease rather than in the common setting of therapeutic failure which is usually driven by a further decline in beta-cell function and plasticity. One caution in therapeutics for diabetes is extrapolation of physiologic mechanisms and effects into clinical outcomes. Despite well validated mechanistic effects of rosiglitazone on atherogenesis, the anticipated short-term CV outcome benefit has never been demonstrated. Despite numerous models of in vivo and in vitro beta-cell effects of pioglitazone, as well as diabetes prevention trials such as PIPOD 86 and ACT NOW (De Fronzo), potential disease modifying effects remain based on at best 2-5 year studies, and no long term data exists to document additive benefits of combination pioglitazone/metformin therapy on therapeutic durability. De Winter and colleagues 87 have developed pharmacodynamic models that avoid single point assessments of physiologic and therapeutic response and may become valuable in assessing potential long-term efficacy of combination therapy without lengthy clinical outcome trials. Nevertheless, with appropriate safety assessment the use of combination pioglitazone and metformin should be considered as a potential initial or early add-on therapy for management of diabetes, especially in the highly insulin-resistant patient or those newly diagnosed patients who are at higher risk for more rapidly progressive disease.
Conflicts of Interest Statement
Dr. Stolar has received speakers honorarium from Takeda, Amylin, Lilly and Novo-Nordisk and has served as an advisory board member for Takeda and Lilly.