
Abstract
Bipolar disorder is a common and complex condition, starting early in life and continuing throughout the life cycle. Most people suffering from bipolar disorder manifest other problems as well, including metabolic disturbances, cardiovascular disease, anxiety disorders, substance use disorders, attention deficit hyperactivity disorder, and borderline personality disorder, among others. The treatment of bipolar disorder needs to be conceptualized within this context of early onset, chronic course, and significant co-morbidity. Because of its unique mode of action, its efficacy and its good tolerability profile, aripiprazole is well placed among the different treatment options to benefit the patient with bipolar disorder. This article will focus on aripiprazole's pharmacology, efficacy, effectiveness, and tolerability from a clinical perspective, while considering the complexities of bipolar disorder.
Introduction
Bipolar disorder is a common and complex condition, starting early in life and continuing throughout the life cycle. 1 A prevalence of bipolar spectrum conditions of approximately five percent in the general population has been reported in many different countries.2–4 Most people suffering from bipolar disorder manifest other problems over their lifespan, due to genetic vulnerability, psychosocial adversity, or the disruption of normal developmental pathways by the drastic mood and behavioral changes. These problems include metabolic disturbances, cardiovascular disease, anxiety disorders, substance use disorders, attention deficit hyperactivity disorder, and borderline personality disorder, among others.5–7 It is within this context of early onset, chronic course, and significant general medical and psychiatric co-morbidity that the treatment of bipolar disorder needs to be conceptualized.
Even though many different types of interventions are necessary to improve the functioning of patients with bipolar disorder, pharmacotherapy, to stabilize mood, reduce impulsivity, and improve cognition, is the mainstay of the treatment plan. Only 15 years ago, data supported just three medications as mood stabilizers, namely lithium, valproic acid, and carbamazepine. In 2008, many more medications have an established track record in treating at least one phase of the illness, while not worsening another, and/or maintaining improvement over extended periods of time. 8 The atypical antipsychotics, aripiprazole, olanzapine, quetiapine, risperidone, ziprasidone, and the anticonvulsant lamotrigine, have methodologically sound data showing their usefulness in the treatment of this illness. Others, such as clozapine, oxcarbazepine, typical antipsychotics, and antidepressants, are used as well. With the increase in choices among treatment options, comes increased responsibility on the clinician's part to match a particular treatment to the individual patient, taking into account factors such as age, general medical conditions and psychiatric co-morbidities.
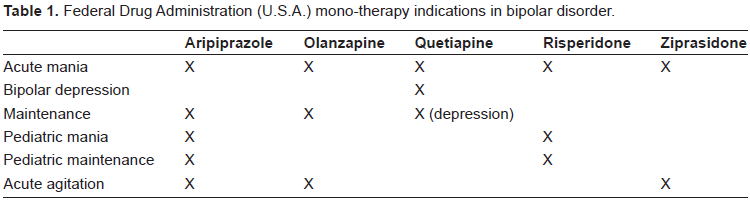
Aripiprazole, an atypical antipsychotic, has an extensive data base in bipolar disorder and is, currently, the medication with the most approved indications in bipolar disorder in the United States, according to the U.S. Food and Drug Administration (Table 1). Because of its unique mode of action, and its good efficacy and tolerability profile, Aripiprazole is well placed among the different treatment options to benefit the patient with bipolar disorder. This article will focus on Aripiprazole's pharmacology, efficacy, effectiveness, and tolerability from a clinical perspective, while considering the complexities of bipolar disorder.
Federal Drug Administration (U.S.A.) mono-therapy indications in bipolar disorder.
Pharmacology
Historically developed as treatments for schizophrenia, most atypical antipsychotics, including aripiprazole, have shown efficacy in certain phases of bipolar disorder. The effectiveness of current antipsychotics is believed to stem from their influence on dopaminergic neurotransmission. Dopamine, a key neurotransmitter in psychosis and schizophrenia, clearly plays a major role in depression and manic-depression/bipolar disorder, as well. 9 It is a major neurotransmitter in brain circuits influencing attention, motivation, perception, and mood. 10 While the first generation antipsychotics, like phenothiazines, are strong antagonists at certain dopamine receptors (i.e. D2), second generation (atypical) antipsychotics like risperidone, olanzapine, quetiapine and ziprasidone, continue this antagonism, while exhibiting additional mechanisms of action.
Aripiprazole, arguably the first of the third generation antipsychotics, is not a D2 receptor antagonist, but a D2 receptor partial agonist. 11 In theory, this has tremendous implications for the treatment of bipolar disorder and its frequent co-morbidities, such as attention deficit hyperactivity disorder (ADHD) and substance use disorders. Stimulating abnormally low and inhibiting abnormally high D2 activity, in prefrontal and mesolimbic brain pathways, may stabilize the dopaminergic system with concomitant improvement in attentional, motivational, affective and perceptual functioning. 12 Since dopaminergic neurotransmission in limbic areas may be low in depression and high in mania, partial D2 agonism may be related to mood stabilization. 9 Preliminary evidence also indicates improvement in disorders of attention and motivation such as Attention Deficit Hyperactivity Disorder (ADHD) and substance dependence.13,14 This same mechanism of action, however, has been implicated in the explanation of rare adverse events, such as worsening psychosis. 15
While partial D2 agonism sets aripiprazole aside from all the others, it shares other therapeutic mechanisms with the second generation antipsychotics, including partial agonism at serotonin 5HT1A and antagonism at 5HT2A receptors. These actions are more than likely related to this class of medications’ beneficial effects in mood disorders. 16 Many other receptors are influenced by aripiprazole, some of which may explain side effects: alpha-adrenergic and histaminergic antagonism may be responsible for autonomic and sedative properties.
Oral Aripiprazole has a bioavailability of 87% with peak serum concentrations after three to five hours. It is 99% protein bound. Aripiprazole is metabolized through cytochrome P450 3A4 and 2D6, with an active metabolite, dehydroaripiprazole. The average half-life of aripiprazole is approximately 70 hours and of dehydroaripiprazole 90 hours. 17 This half-life is significantly longer with certain drug-drug interactions: for example, two frequently used selective serotonin reuptake inhibitors, fluoxetine and paroxetine, and metoprolol, a beta-blocker, inhibit cytochrome 2D6 strongly and prolong aripiprazole elimination time. This also occurs in approximately eight percent of Caucasians and three percent of Asians and Africans who, for genetic reasons, lack this 2D6 cytochrome. 18 Even though it is not contraindicated to co-prescribe aripiprazole and fluoxetine, paroxetine or metoprolol, appropriate dosage adjustments are necessary in these situations.
A recent exploratory investigation in dose–-serum level correlations of aripiprazole reported some interesting findings. Even though serum levels between patients were highly variable, they did correlate significantly with dose. The concentration of the active metabolite dehydroaripiprazole was approximately 40 percent of the parent compound. Inhibitors of the metabolizing enzymes 3A4 and 2D6 changed the serum concentration by about 50 percent. Improvement was best seen with aripiprazole concentrations between 150 and 300 ng/ml, while side effects increased significantly with concentrations above 250 ng/ml. 19
Since aripiprazole, at least in the U.S.A, is indicated for the treatment of pediatric schizophrenia and pediatric bipolar disorder, it is important to investigate its pharmacokinetics in this patient population. Like in adults, aripiprazole has linear kinetics in youth, and shows comparable pharmacokinetic parameters. 20
Both in mood disorders and schizophrenia, doses of aripiprazole have ranged from 10 mg per day to 30 mg per day. It is available (in the U.S.) in oral doses of 2 mg, 5 mg, 10 mg, 15 mg, 20 mg and 30 mg. It is also available in oral suspension and in injectable form, to help acute agitation.
In summary, aripiprazole is a partial D2 agonist with significant serotonergic effects. It has good bio-availability, is highly protein bound, and is metabolized through 3A4 and 2D6 enzymes. It has lineair kinetics, while both aripiprazole and its active metabolite have a long half-life.
Efficacy and Effectiveness
Mania
The efficacy of aripiprazole in the acute manic or mixed phase of bipolar disorder was clearly established through two identical studies.21,22 These studies were double blind and placebo controlled, included large groups of hospitalized patients (>250 in each study), and were three weeks in duration. Patients suffered a manic or mixed phase relapse, with or without psychosis. Aripiprazole was started at 30 mg per day in these inpatients, although a reduction to 15 mg per day for tolerability reasons was allowed. The Young Mania Rating Scale (YMRS), the typical outcome measure in bipolar studies, showed a significantly greater improvement for aripiprazole, compared to placebo, in both studies. Categorical outcomes, i.e. response rates, defined as a 50 percent reduction in the YMRS, were much better with active medication as well: 53 percent versus 32 percent, and 42 percent versus 21 percent.
In reviewing double blind placebo controlled studies in acute mania, it appears that the efficacy of aripiprazole in reducing the YMRS is very similar to other atypical antipsychotics, even though head to head comparisons are not available.23,24 The same conclusion was formulated when other, more traditional, mood stabilizers were compared with the atypicals, including aripiprazole. 25
No head to head comparisons between new antipsychotics are available in acute mania, but a comparison between haloperidol and aripiprazole showed significantly more improvement and tolerability in patients taking the latter medication. Fifty percent of patients responded to aripiprazole after 12 weeks of treatment, while 28 percent improved with haloperidol. 26 Typical antipsychotics, like haloperidol, have indeed largely been replaced by the atypicals in the treatment of mania.
Since lithium is still considered the gold standard treatment and traditional mood stabilizer for bipolar I disorder, investigators compared aripiprazole to lithium and placebo in 480 hospitalized patients with an acute manic or mixed bipolar episode. They concluded that aripiprazole was as efficacious as lithium with a 47 percent response rate after three weeks of treatment. 27
The efficacy of aripiprazole in mania does not depend on a specific subtype of bipolar disorder since patients with more or less severe illness, with mixed or manic episodes, with or without psychotic features, or with a history of rapid or non-rapid cycling responded equally well. Men and women, and patients in different age groups, 18-40 and 41-55, showed no difference in their improvement. 28
Many patients with bipolar disorder require treatment with more than one mood stabilizer, due to efficacy or tolerability concerns. In fact, several guidelines for the treatment of severe mania recommend the combination of a traditional mood stabilizer with an atypical antipsychotic. In a large outpatient study (n = 384), aripiprazole, in combination with lithium or valproate, was more efficacious than placebo in reducing the YMRS, when manic patients did not respond adequately to therapeutic doses of lithium or valproate alone. 29
Pediatric mania
The clinically significant reduction in the YMRS, manifested during treatment with aripiprazole in adult bipolar disorder, was also seen in a large pediatric study: 296 patients between the ages of 10 and 17, with a diagnosis of bipolar I disorder manic or mixed episode with or without psychosis, were randomized to placebo, aripiprazole 10 mg, or aripiprazole 30 mg per day for four weeks. In the active medications groups, the YMRS dropped from an average of 30 to an average of 15. 30 Similar results have been reported in an open label study 31 and a retrospective chart review, 32 confirming the effectiveness of aripiprazole in young patients.
Bipolar depression
Most patients with bipolar disorder spend more time in depressive, rather than manic, episodes. Complicating this fact is the finding that bipolar depression does not respond well to current therapies, compared to manic episodes or unipolar depressive periods. 33 Clinically, bipolar depression remains a challenge and a major source of disability.
This challenge was highlighted in two recent studies of aripiprazole mono-therapy for non-psychotic bipolar depression: over eight weeks, more than 700 patients, in both studies combined, were randomized to placebo or aripiprazole (5 mg to 30 mg), while followed with the Montgomery Asberg Depression Rating Scale. Although Aripiprazole separated statistically from placebo during weeks one to six, it did not achieve statistical significance versus placebo at week eight in either study. 34
An open label study of 31 patients with bipolar depression indicated that aripiprazole produced a response in 42 percent and remission in 35 percent, after eight weeks of treatment. 35 Several studies have found the medication to be helpful as an adjunct to ongoing mood stabilizer and antidepressant treatment.36,37 For example, 30 outpatients with treatment-resistant bipolar depression, in the Systematic Treatment Enhancement Program for Bipolar Disorder, received adjunctive aripiprazole in a mean dose of 15 mg per day for approximately three months. Twenty-seven percent of patients responded, while 13 percent remitted. 36 While these numbers appear low, they are comparable to response and remission rates in community treatment of unipolar depressive disorders.38,39
Maintenance
For the large majority of patients afflicted with bipolar disorder, it is a life long illness with many ups and downs, remissions and relapses. Thus, long term treatment is of utmost importance. In this regard, aripiprazole has shown to be of benefit in bipolar maintenance. In a relapse prevention study, 161 patients were randomly assigned to aripiprazole or placebo for a 26 week, double blind phase, after stabilization (no significant depressive or manic symptoms) with open-label aripiprazole for at least six weeks. Patients on aripiprazole experienced significantly fewer relapses (25%) than placebo patients (43%). Time to relapse was longer in the aripiprazole group. Aripiprazole was superior to placebo in delaying the time to manic relapse, but not to depressive relapse. 40 These results were maintained in a 76 week extension of this study to a total of 100 weeks. 41
Pediatric maintenance
Since there is no evidence to believe that early onset bipolar disorder is a more benign or less chronic condition, long term treatment and maintenance in youth is important as well. Aripiprazole, 10 mg or 30 mg per day, maintained improvement in the YMRS scores over 26 weeks, after a four week acute treatment phase. One hundred and sixty-one patients, 10 to 17 years old, entered the 26 week continuation phase on active medication, compared to 76 patients on placebo. YMRS scores were significantly better at the end of 26 weeks in patients taking aripiprazole, while discontinuation rates were smaller and time to discontinuation longer in the aripiprazole groups. 42
Effectiveness in co-morbid conditions
Since bipolar disorder is a highly co-morbid condition, it is of great interest that aripiprazole has shown at least partial effectiveness in many of the commonly associated disorders. In this regard, it is striking that, in the above mentioned pediatric bipolar study, the 18-item ADHD rating scale dropped significantly compared to placebo during the four week mono-therapy aripiprazole treatment (-12.5 and -11.9 in aripiprazole groups; -3.7 in placebo group). ADHD is indeed a frequent co-occurring problem in pediatric bipolar disorder. Positive results in non-bipolar ADHD with aripiprazole have been published. 14 Other frequent issues in bipolar disorder include anxiety disorders, substance abuse, borderline personality disorder, and aggressive behavior. These problems have shown improvement with aripiprazole treatment as well.13,43,44 The double blind placebo controlled trial in borderline personality disorder showed improvements in depression, anxiety, anger, aggressiveness, paranoia, and global functioning. Aggressiveness, a frequent reason for referral to clinical care in youth with bipolar disorder, showed marked improvement in a community clinic study of aripiprazole and ziprasidone, with the Overt Aggression Scale as the primary outcome. 45 Over a period of two months, aggression scores declined by 63 percent. Preliminary evidence indicates aripiprazole's usefulness in addiction and anxiety problems, two frequent co-morbid concerns in bipolar disorder.46–48
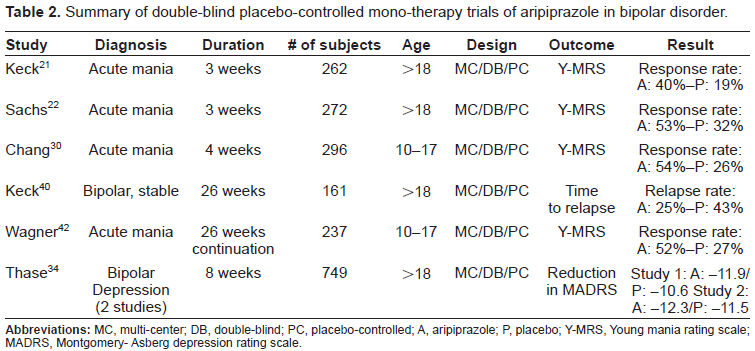
In summary, solid evidence indicates that aripiprazole is efficacious in the treatment of acute mania and in the maintenance treatment of bipolar disorder, in youth and adults. Table 2 presents the main studies. Some evidence indicates its usefulness in bipolar depression and in the co-morbid conditions of anxiety, substance use, and disruptive behavior disorders.
Summary of double-blind placebo-controlled mono-therapy trials of aripiprazole in bipolar disorder.
Safety and Tolerabilty
The safety of a particular medication needs to be judged within the context of the disease it treats. Therefore it is important to be cognizant of the complexities of bipolar disorder with early onset, chronic course, psychiatric co-morbidity, possible substance misuse, association with metabolic and cardiovascular disease, and possibly repeated non-adherence, when considering the side effect profile of aripiprazole. It is thus reassuring that systematic safety data for aripiprazole in bipolar disorder are available in pediatric (>10 years old) and adult patients, in acute and long-term studies.
Since aripiprazole belongs to the class of anti-psychotic medications, much of its side effects could be anticipated by considering the first and second generation antipsychotic adverse event profiles. However, significant differences exist that place aripiprazole apart from its many predecessors. In general terms, aripiprazole shows significantly fewer neurological side effects than the first generation antipsychotics, while not contributing much to metabolic disturbances, a significant liability of several second generation antipsychotic medications. Indeed, the second generation anti-psychotics, such as risperidone, olanzapine, and quetiapine, provide a relatively benign neurological profile, but present with concerns about negative metabolic effects. 49
In the adult acute mania treatment studies, the most common adverse events of aripiprazole were headache, nausea, somnolence, akathisia, agitation, constipation, vomiting, anxiety, and lightheadedness. Only akathisia, nausea, and constipation were more frequent than with placebo. Discontinuations during the three week acute trials, related to adverse events, were below ten percent. Most side effects abated after the first week.21,22 A similar side effect profile was apparent in the acute pediatric mania trial with somnolence, extrapyramidal events, fatigue, nausea, akathisia, blurry vision, salivary hypersecretion and dizziness, as the most common reported problems. 50 Overall, pediatric patients appear to show more sedation and parkinsonian side effects, and less akathisia. In the acute studies, 5 percent of adults and 27 percent of youth showed extra-pyramidal side effects, while 8 percent of adults showed sedation compared to 26 percent of youth. Akathisia was present in 13 percent of adults and 11 percent of pediatric patients.50,51
It is important to consider the study protocols in the interpretation of these adverse event frequencies: in general, titration was very fast, possibly increasing the risk for a variety of acutely emerging side effects. In a different treatment setting, with a slower titration frequency, tolerability may be significantly better.37,45,52
Aripiprazole's low affinity for alpha1 adrenergic, histaminergic, and muscarinic receptors may be the reason for the low rates of observed side effects, such as sedation, orthostasis, and gastro-intestinal problems. The incidence of akathisia, agitation, and anxiety, subjective states that are difficult to differentiate may be related to the D2 partial agonism of this medication. 53
While side effects in the acute phase, such as akathisia, sedation, or nausea, are transient or can be managed in the clinical setting, adverse events related to long term use of antipsychotics are potentially more serious and, at times, irreversible. Tardive dyskinesia (TD), weight gain, and metabolic changes are well known negative consequences of first and second generation antipsychotics. In general, it is believed that aripiprazole has less potential for these side effects.54,55 It is considered to have a lower risk profile for obesity and diabetes than many other second generation antipsychotics. 54 This may be the most important contribution of aripiprazole to the treatment of bipolar disorder, an illness associated with significant metabolic and cardiovascular morbidity.6,56,57
In the 26 week maintenance study of bipolar disorder with aripiprazole in adults, the only problems, more common than with placebo, were anxiety and nervousness. 40 Somnolence, extrapyramidal events, and fatigue continued to be the most common problems in the 30 week trial of pediatric mania. 42
In a 100 week bipolar maintenance treatment study, the following metabolic or cardiovascular side effects were seen: hypertension in 7.8% (placebo 3.6%) and weight gain in 6.5% (placebo 0%) of patients, while aripiprazole had no effect on QTc interval of the ECG, total cholesterol, LDL or HDL cholesterol, triglycerides, or glucose levels. 41 At the same time, other long term side effects, such as TD and hyperprolactinemia, appear less likely with aripiprazole as well.41,55
Despite its good overall safety profile, clinical monitoring of cardiovascular, metabolic, and neurological side effects is still indicated in patients treated with aripiprazole. Rare case reports of keto-acidosis, 58 elevation of triglycerides, 59 neuroleptic malignant syndrome, 60 and parkinsonism 61 have been published, although not necessarily in bipolar disorder.
In children and adolescents, systematic long term safety data are not yet available. In the author's experience in treating youth with aripiprazole, it appears that weight gain and parkinsonian side effects are more common than in adults. These side effects have been noticed more commonly in young patients with many psychotropic medications. 62
In summary, acute side effects of akathisia, nausea, and sedation (in youth) are relatively common, while aripiprazole's long term cardiovascular and metabolic profile is very favorable.
Patient Focused Perspective
While many treatment studies with atypical antipsychotics have focused on symptom control and maintenance in bipolar disorder, limited data are available on factors most important to patients: acceptability of the treatment, adherence to the therapeutic regimen, satisfaction with its effects, and above all, quality of life. Quality of life is seriously compromised in people suffering from this chronic mood disorder. 63 The depressive phase of the illness appears to be mostly responsible for this reduction, although hypo-manic or manic symptoms contribute to poor quality of life as well. 64 Patients’ functioning is further negatively influenced by medical and psychiatric co-morbidity. 65
No doubt, mood stabilizing medications enhance patients’ quality of life through reduction in disruptive behavior, depression, and suicide potential. But improved functioning through effective treatments can be offset by side effects. Medications’ adverse consequences can lead to poor adherence or general medical disturbances. 66 While it is generally believed that the newer, second generation, antipsychotic medications lead to better adherence and better quality of life, through better subjective tolerability, evidence for these assertions is sparse. 67 Also, there are no economical data available on the treatment of bipolar disorder with aripiprazole.
Even though no data on acceptability, satisfaction, and quality of life are available for aripiprazole in bipolar disorder, one would assume, based on the efficacy and tolerability data discussed in this paper, that these parameters would be favorable with aripiprazole compared to many other mood stabilizing medications. Preliminary data, albeit in schizophrenia, point in this direction. Weight and weight related quality of life were better with aripiprazole, compared to olanzapine, quetiapine and risperidone, in 555 patients with schizophrenia over 26 weeks. Physical functioning, self esteem, and sexual life were better in patients treated with aripiprazole. 68 Patients preferred aripiprazole more often compared to previous treatments. 69
In summary, much more research is needed to have a better patient focused perspective on aripiprazole.
Clinician Focused Perspective
Every time a new medication becomes available, clinicians need to go through a learning process, guided by limited data from randomized controlled studies. These studies are not representative of the treatment in community populations, however. Therefore, based on a vast experience with aripiprazole in a community outpatient clinic, some general guidelines are presented.
Dosing in most patients should be initiated lower and adjusted slower, compared to the published studies, to avoid subjective intolerability related to akathisia and gastro-intestinal distress. When these side effects do occur, temporarily lowering the dose appears to be the most effective remedy. Tolerability can be enhanced by initiating at night time in youth and in the morning in adults. Twice a day dosing may alleviate some side effects as well. When switching from most other antipsychotics with strong D2 antagonism, to aripiprazole, with D2 partial agonism, it is strongly recommended to cross-titrate very slowly and over an extended period of time, to avoid agitation or worsening of mania/psychosis. It is indeed possible that up-regulated D2 receptors would temporarily be stimulated through the partial dopamine agonism of aripiprazole, which has the highest affinity for this receptor among all antipsychotic medications. Drug drug interactions have been discussed. Neurological examination and metabolic screening continue to be necessary. While these guidelines are mostly applicable in mild to moderately ill outpatients, modifications with acutely ill inpatient populations are indicated. 70
In summary, as with many newer medications, aripiprazole's unique pharmacological profile requires a more in depth understanding on the part of the physician “to make this medication work” for their patients.
Conclusions
The first step in providing good care is to diagnose properly (International Society for Bipolar Disorders). 71 This is a challenge in bipolar disorder. Both under-diagnosis and over-diagnosis appear to be problems.72,73 Even though atypical antipsychotics are used in a variety of conditions (schizophrenia, mania, aggression, tics, augmentation in depression and some anxiety disorders, dementia), they should not be prescribed indiscriminately. Many antipsychotics have serious side effects that can reduce the quality of life, and possible life expectancy, of patients. A correct diagnosis, with its associated prognosis, helps in providing the patient with an empirically based cost-benefit analysis of the treatment.
Once a proper diagnosis is established, many factors need to be considered in selecting an appropriate treatment. Today, mood stabilizing medications are the core intervention for patients with bipolar disorder. Aripiprazole is one of these mood stabilizing options. The role of aripiprazole in bipolar disorder can be summarized as follows:
Efficacy, as mono-therapy, in acute adult and pediatric mania has been established.
In severe adult mania, combination treatment with lithium or valproate is safe and efficacious.
Maintenance efficacy, especially against manic relapse, in adult and pediatric bipolar disorder is present.
No strong evidence of efficacy in bipolar depression is present, but some data point to possible effectiveness in select patients.
Partial improvement in associated conditions of aggression, substance use, ADHD, and anxiety may be expected with aripiprazole.
One of the major contributions of aripiprazole to the therapeutic armamentarium for bipolar disorder is its relatively benign metabolic profile.
Disclosure
L. Bastiaens is on the speaker's bureau of Bristol-Myers Squibb, Eli Lilly, and Takeda, and has received research honoraria from Janssen, Forest and McNeil.