
Abstract
Background
In acromegaly expert surgery is curative in only about 60% of patients. Postoperative radiation therapy is associated with a high incidence of hypopituitarism and its effect on GH production is slow, so that adjuvant medical treatment becomes of importance in the management of many patients.
Objective
To delineate the role of lanreotide Autogel® in the treatment of acromegaly.
Methods
Search of Medline, Embase and Web of Science databases for clinical lanreotide studies in acromegaly.
Results
The weighted mean of serum GH normalization by Lanreotide Autogel®, based on 10 published clinical studies, was 58% in 370 patients. These patients were mostly switched from other somatostatin analogs. Serum IGF-I concentration normalized in 48% of these patients. Three small studies, with a total of 60 patients, compared the efficacy of octreotide LAR and that of lanreotide Autogel®. The highest dose of lanreotide appeared to be equivalent with 20 mg of octreotide LAR. Observed side effects were comparable with other somatostatin analogs, including octreotide LAR. Due to the lack of studies with previously, non-medically treated, patients no reliable data on tumor shrinkage is available.
Conclusion
Lanreotide Autogel®, a latecomer in the second generation of somatostatin analogs, has a therapeutic profile similarte octreotide LAR, which is now in clinical use for more than a decade. Preference for one of the drugs is dictated by the physician, patient and the cost of the drug.
Introduction
Growth hormone (GH), a polypeptide secreted by the pituitary gland has many effects, the most obvious being stimulation of growth in children. The childhood lack of GH causes dwarfism while excessive secretion results in gigantism. Growth hormone has profound metabolic effects by stimulating protein anabolism and lipolysis. Other effects include stimulation of bone turnover, leading to a net increase in bone volume, muscle growth, insulin antagonism, renal sodium retention and immuno-modulation. Most effects of GH are indirect and mediated via insulin-like growth factor-I (IGF-I). This peptide is synthesized and secreted as a result of GH-signaling, which acts locally in an autocrine or paracrine manner, or systematically as a hormone when secreted by the liver. 1 In mice, about 70% of the circulating IGF-I is derived from the liver. 2
Excessive secretion of GH leads to acromegaly, a disfiguring and debilitating condition causing severe co-morbidity and premature death.3–6
Clinical Features of Acromegaly
Acromegaly is a rare disease, caused by a GH-secreting adenoma of the pituitary gland. The incidence of acromegaly is about 3-4 per one million per year and the prevalence is 60-70 per one million, without geographical or sex differences.7–10 Clinical features of acromegaly include acral enlargement, prognatism, jaw malocclusion, arthropathy, carpal tunnel syndrome, hyperhydrosis, sleep apnea and visceromegaly.5,11 Acromegaly leads also to cardiomyopathy which involves the myocardium, conduction system and heart valves. Cardiac manifestations include arrhythmia, valvular regurgitation, concentric left ventricular hypertrophy and left ventricular systolic and diastolic dysfunction.11–13 The incidence of hypertension and of glucose intolerance is also increased. This is also true for the incidence of colon polyps and colon carcinoma.14,15 It is controversial however, whether the relative risk of cancer is increased in patients with acromegaly compared with that of the general population.16–18
Symptoms caused by the tumor include chronic headache, visual field defects and rarely cranial nerve palsies. Hypopituitarism is mostly associated with large tumors and the incidence is between 3%-10%. 19
Biochemical criteria of active disease and remission are the (mean) GH, glucose-suppressed GH and the IGF-I concentration. 20 GH assays differ in specificity, sensitivity and the used GH standard and therefore individual clinical endocrine laboratories should establish a normal range of gender- and age-related GH and IGF-I values, which should ideally be corrected for fat mass or a fat mass-derived parameter.21,22 Serum IGF-I reflects GH secretion rate and serum concentrations of IGF-I are elevated in all patients with active disease. 5 IGF-I concentrations decrease with advancing age. In addition, gender, sex hormone status, the use of an oral estrogen, thyroxine and body composition can all influence IGF-I concentrations. 23
Treatment of Acromegaly
Epidemiological studies have clearly demonstrated that controlling GH and IGF-I secretion is the most significant determinant of restoring the life expectancy in patients with acromegaly.24,25 As a consequence, the main goal of treatment of acromegaly is to achieve nadir GH levels below 1 μg/l after a glucose load, to normalize age- and gender matched IGF-I levels, to ablate or reduce tumor mass and prevent its recurrence, and finally to alleviate significant co-morbidities, especially cardiovascular, pulmonary and metabolic disturbances. 26 The currently available treatment modalities for acromegaly are selective transsphenoidal adenomectomy, radiotherapy, medical treatment, or combinations thereof.
Transsphenoidal surgery
This oldest treatment modality was developed a century ago by the Austrian neurosurgeon Schloffer. 27 It is usually performed via the transnasal, transsphenoidal route. In recent years most neurosurgeons have adopted the endoscope instead of the surgical microscope which has obvious advantages for the patient and leads to a better visualization of the operating field. Other variants of surgical techniques are neuronavigating and real-time intraoperative MRI scanning, aimed at visualization of tiny tumor remnants after resection of the adenoma.28,29 Surgical cure is highest in patients with a microadenoma (diameter less than 1 cm) varying from 80% to more than 90% in the hands of experienced neurosurgeons. However, complete tumor removal becomes more difficult with increasing tumor size and expansion into the neighboring delicate structures. Therefore, the cure rate of large macroadenoma drops to only 20 to 40% of cases.30–38 The obvious advantage of successful surgery is the rapid normalization of GH secretion and decrease in IGF-I levels, while the complication of (partial) hypopituitarism is mostly below 10%.37,38
Radiotherapy
Conventional radiotherapy is administered by a linear accelerator (4-8 MeV) with a total dose of 40-45 Gy, fractionated in at least 20 sessions. A rotational field, two opposing fields or a three-field technique are used. A mean GH decrease of about 50% is observed in the first two years after irradiation and after 5 years a 75% decline is reported.39–45 Whether the GH level normalizes post-irradiation depends mainly both on preirradiation serum GH concentration and the time interval between radiotherapy and the measurement of GH and IGF-1 levels. Post-irradiation remission rates are, however, largely affected by the extent of surgical debulking before radiotherapy. Other than the slow onset of GH control another drawback is the increasing incidence of hypopituitarism varying from 50%-85% after a follow-up of 10 years or longer.46,47
Radiosurgeryis the precise, stereotactic delivery of a single high radiation dose to a defined target with a steep dose gradient at the tumor margin.48–50 This form of radiotherapy uses a gamma knife with up to two hundred 60 Co sources, a Linac-based system or proton beams.51–53 The advantage of this form of radiation is that only one session is required. Otherwise there is no convincing evidence yet that radiosurgery is superior to conventional irradiation for GH control, time needed to reach clinically acceptable GH levels and incidence of hypopituitarism.47,54,55
Disadvantages of pituitary irradiation other than the development of hypopituitarism include the decreased quality of life (QoL), the development of secondary tumors, cerebrovascular disease and increased mortality. The decreased health-related quality of life (QoL) was described in acromegalic patients in long-term remission.56,57 A significant predictor of poor QoL was radiotherapy, but the pathophysiologic mechanism remains unclear. Increased mortality due to cerebrovascular disease was observed in two studies,58,59 but not in three others.60–62 The effect of radiotherapy on mortality is thus yet to be established. The likelihood of secondary tumor formation after pituitary irradiation is very low.46–63
Medical treatment
The three most important drugs used for medical treatment of acromegaly are dopamine agonists, somatostatin analogs and GH-receptor modulating chemicals.
Somatostatin analogs
Somatostatin was isolated in 1973 from the hypothalamus and subsequently synthesized. 64 The hormone is processed from a large pre-prohormone into two cyclic peptides, consisting of 14 or 28 amino acids (Fig. 1). The short form, SS14, is predominantly present in the brain, whereas SS28 is widely distributed in peripheral organs. Somatostatin acts as a neuromodulator and neurotransmitter in the brain and as a neurohormone in the regulation of GH and TSH secretion. In addition, somatostatin inhibits tumoral ACTH secretion in Cushing's disease. 65 Somatostatin also acts as a neurotransmitter in the extensive myo-enteric plexus, and as a hormone in a paracrine and autocrine fashion. Somatostatin exerts many inhibitory effects on gut and pancreatic hormones, including gastrin, insulin, glucagon, VIP, motilin and GIP. Other effects of somatostatin include the inhibition of gastric emptying, the secretion of pancreatic enzymes and bicarbonate, gastrointestinal blood flow and bile flow.64,66,67 Somatostatin acts via a G-protein-coupled receptor, of which 5 subtypes have been cloned and characterized. 68 After binding of somatostatin to its receptor, the activities of adenyl cyclase and of calcium channels are inhibited, whereas phosphotyrosine phosphatase activity and MAPK activity are stimulated. The first two processes are involved in the inhibition of secretory processes, and the latter two may play a role in cell proliferation, e.g. activation of the SST3 receptor may induce apoptosis.69,70 Analogs of somatostatin differ in binding properties to different receptor subtypes. 68 Many benign and malignant tumors express one or more somatostatin receptors. Receptor distribution and density and homogeneity of receptor expression within the tumor determine whether a particular analog can be effectively used therapeutically.70,71
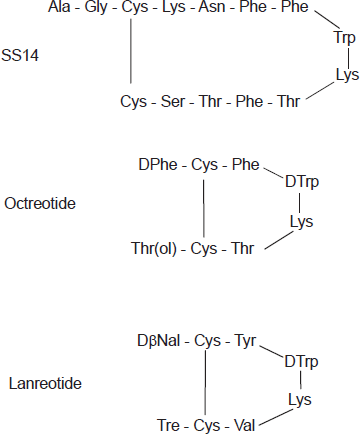
Amino-acid structure of somatostatin-14, octreotide and lanreotide.
GH-secreting pituitary adenomas predominantly express SST2 and SST5 receptors. The current clinically used analogs, octreotide and lanreotide inhibit GH secretion via the somatostatin receptor subtype 2. 73 The plasma half-life of these analogs is about 20 times longer than that of native somatostatin, which is less than 3 minutes. 68 Although the most important effect of somatostatin analogs is the inhibition of GH secretion by the adenoma leading to a subsequent decrease in circulating liver-derived IGF-I, part of the peripheral effects of these analogs is caused by the direct inhibition of IGF-I gene transcription after binding to the somatostatin receptor.74,75 The magnitude of this latter effect in various organs is not exactly known.
GH receptor antagonists
Pegvisomant is an engineered GH analog that antagonizes GH at the receptor site, and thus prevents endogenous GH activation of its receptor and subsequent downstream signaling. In short-term studies, the lowest dose (10 mg/day) normalized IGF-I in 38% of the patients and 20 mg normalized IGF-I in 82% of the patients.76,77 In a minority of the patients (2 out of 112 and 7 out of 229 patients, respectively) adenoma size increased during a relatively short treatment period.77,78 Careful documentation of tumor size before starting pegvisomant treatment and long-term monitoring is advisable. A small number of patients (2 out of 167 cases), developed abnormalities in liver function tests, necessitating the withdrawal of the drug, although increased liver enzyme levels, e.g. more than 3 times the upper level of normal was observed in 5.5% of 229 patients, which normalized spontaneously in 3.1% on continuing treatment.77,78 About 40% of the patients develop minor abnormalities in liver function tests on combined treatment with somatostatin analogs, not requiring stopping of drug, and which usually resolve spontaneously. 79
Dopamine agonists
Bromocriptine effectively reduces GH secretion in only a minority of patients with a GH-secreting adenoma. 80 Cabergoline, a more potent dopamine agonist with a prolonged duration of action normalizes GH in 35% and IGF-I in 44% of 46 patients with a purely GH-secreting adenoma. 81 The efficacy of cabergoline was somewhat better in tumors co-secreting prolactin, which occurs in about one-third of the patients. 82 Quinagolide, another dopamine agonist normalized IGF-I in 28% of patients. 83 Most endocrinologists presently use long-acting dopamine agonists as adjunct therapy in patients who fail to normalize GH secretion with somatostatin analog monotherapy. Combination therapy normalizes serum IGF-I concentrations in 30% to 40% of patients, irrespective of the prolactin concentration. 84 Side effects of cabergoline are rare although there has been recent concern about cardiac valve hypertrophy, as observed in patients with Parkinson's disease. Whereas the dose in Parkinson's disease is usually much higher than that used for endocrine indications, 85 patients with acromegaly generally require long-term medical treatment for GH control. Indeed, a recent large-scale retrospective study in patients with prolactinoma treated with different dopaminergic drugs for 8 years did not reveal an increased incidence of cardiac valvular abnormalities. 86
Pharmokinetics of Lanreotide
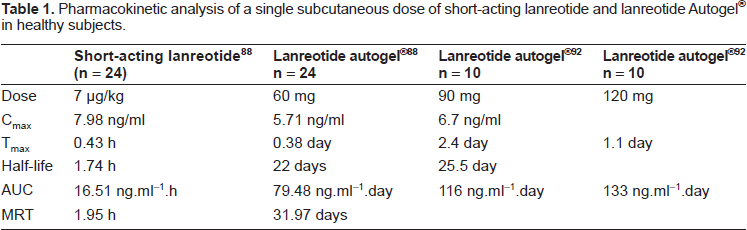
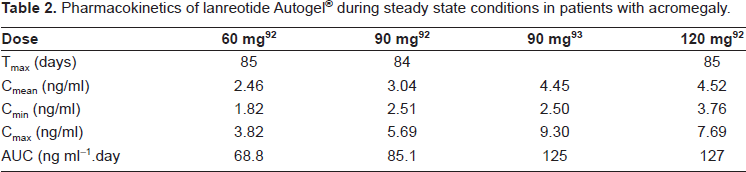
The first pharmaceutical available form of lanreotide (BIM 23014) was relatively short-acting, requiring multiple dosing, three times a day, or subcutaneous infusion. This was nevertheless a major advance in the treatment of many patients who had already undergone unsuccessful surgery and pituitary irradiation and for whom there were no other treatment options (Fig. 1). In healthy subjects, maximal serum concentrations of lanreotide were reached after 30 minutes and the serum half-life was 90 minutes, thus 30 times greater than that of native somatostatin87,88 Table 1. Subsequently, a long-acting form of lanreotide was developed by incorporating the drug into polyactide-polyglycolide microspheres, so that the half-life was considerably prolonged, and the injection interval could be extended to 7-14 days. 89 The lanreotide release pattern from the long-acting form is biphasic, i.e. an early release for two days from the drug adsorbed onto the surface of the microspheres, followed by a sustained release lasting for about one week, followed by an exponential decrease in the drug release thereafter. It was subsequently discovered that lanreotide had the unique property of self-aggregation under favorable conditions, leading to a stable structure of highly organized nanotubules.90,91 This formulation of the drug was named lanreotide Autogel® and has a long half-life after subcutaneous injection determined by pseudo-first order kinetics. Maximal serum concentrations are reached after 1-2 days (see Table 1) in healthy subjects and the serum half-life amounts to 25.5 days.88,92 In acromegalic patients maximal values are reached after 3.8-7.7 days under steady state conditions, depending on the dose administered (Table 2). Simulated steady state pharmacokinetic profiles of long-acting octreotide and lanreotide Autogel® differ significantly.92,93 During long-acting octreotide treatment serum concentrations of the drug are constant, whereas the characteristic first order kinetics of lanreotide Autogel® is superimposed on levels just before the next administration, as illustrated in Figure 2. 92 The pharmacokinetic differences therefore indicate that octreotide LAR can be better tailored to therapeutic levels, whereas serum levels of lanreotide must be (too) high for part of the interval between injections in order to be effective in the period before the next administration. The possible clinical consequence(s) of these different pharmacokinetic profiles are unknown.
Pharmacokinetic analysis of a single subcutaneous dose of short-acting lanreotide and lanreotide Autogel® in healthy subjects.
Pharmacokinetics of lanreotide Autogel® during steady state conditions in patients with acromegaly.
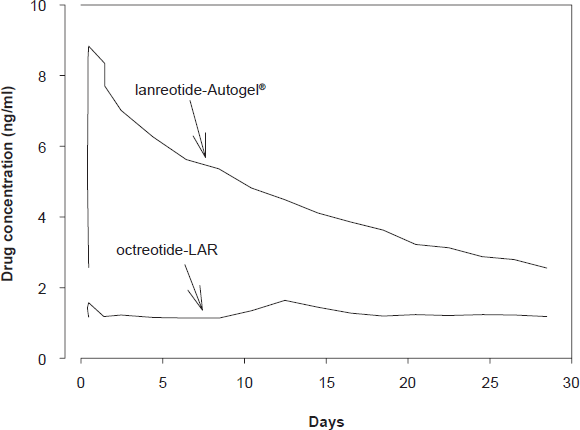
Pharmacokinetic profiles of Lanreotide Autogel® (90 mg) and octreotide LAR (20 mg) at steady state. The lines represent mean values of 10 simulated profiles. Data from Astruc et al. 2005.
Efficacy of Lanreotide
The first studies with lanreotide were performed using lanreotide Slow Release (lanreotide SR). In a recent meta-analysis of these mostly non-randomized studies was the overall better efficacy of octreotide LAR compared with lanreotide SR. 94
The first report in the English literature on lanreotide Autogel® was published in 2002. 95 Clinical efficacy studies are summarized in Table 3. Most of the patients who took part in these studies had undergone pituitary surgery, often with adjuvant irradiation and almost all patients were on octreotide or lanreotide SR treatment, while a minority also used dopaminergic drugs. The results of these studies should therefore be interpreted with caution, as a selection bias cannot be excluded. Normal GH, defined as a concentration below 2.5 μg/L in fasting single blood samples or as the mean of serial samples, was observed in 38% to 80% of cases, and normal age-related IGF-I in 39%-80% of patients. The calculated weighted mean in a total population of 370 patients was 58% for GH normalization and 48% for IGF-I normalization. The results mentioned above refer to measurements at the end of the study when dose titration of lanreotide Autogel® was fully effective. Indeed, most of the patients ended receiving the highest dose of 120 mg. These results do not differ from data obtained in patients on lanreotide SR (see above). Part of these studies compared the efficacy of octreotide LAR and lanreotide Autogel®. An important drawback of these studies is that except for one study, none were randomized. 96 An open label, uncontrolled single group assignment study on the effects of lanreotide Autogel® in 27 previously untreated patients with acromegaly was completed in December 2007, but not published yet (ClinicalTrials.gov, NCT00627796). Although the study is small it might contribute further data on IGF-I control and tumor size reduction.
Clinical studies with lanreotide Autogel® in acromegaly.
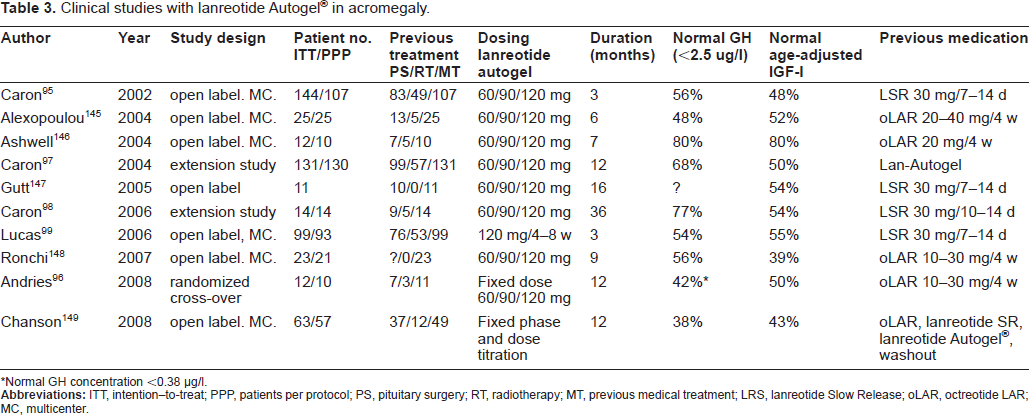
Normal GH concentration <0.38 μg/l.
In a 3-month study, GH was normalized in 48% of 107 patients during lanreotide SR and 56% during lanreotide Autogel® therapy, whereas a normal IGF-I was obtained in 45% and 48% of cases, respectively. 95 In an extension phase of this study to 12 months, the percentage of patients with normalized GH increased from 49% to 68% in 130 patients and 44% and 50% for IGF-I. 97 Fourteen patients of these studies were treated for 3 years with lanreotide Autogel®.
In this subgroup, the incidence of normal GH increased from 36% to 77% and that for IGF-I from 36% to 54%. 98 Finally, the Spanish multicenter study extended the Autogel® injection interval to 8 weeks in patients who were controlled by two–weekly injections with lanreotide SR. The overall GH control increased from 46% to 54%. 99
Studies comparing the efficacy between octreotide LAR and lanreotide Autogel® are displayed in Table 4. All studies were small and only the study by Andries was statistically properly designed. The studies suggest equal efficacy of both drugs in terms of normalization of GH, i.e. below a certain upper normal limit. The study by Andries demonstrated a better GH-suppressive effect of octreotide on absolute GH concentrations than lanreotide Autogel®, although the suppressive effect on IGF-I was similar. In another study there was no difference in the GH-suppressive effect in 7 patients in whom the 24-h GH secretion was precisely measured with a 10 min blood sampling protocol. 100 From the data presented above and despite limitations in design, it would appear that lanreotide Autogel® and octreotide LAR are equipotent in normalizing GH and IGF-I concentrations. 101 However, patients usually require the highest lanreotide dose while most patients on octreotide LAR had safe GH and normal IGF-I levels on the 20 mg dose. For clinical practice, the message should be that patients requiring 20 to 30 mg of octreotide LAR will likely need 120 mg lanreotide Autogel®, and those somatostatin-sensitive patients on octreotide LAR 10 mg mostly require 90 mg of the Autogel® formulation. Lanreotide Autogel® is registered under the trade name Somatuline Autogel® in the majority of the countries, as Somatuline Depot Injection in the U.S.A, and as Ipstyl Autogel® in a few European countries.
Efficacy of lanreotide Autogel® compared with octreotide LAR and lanreotide SR in acromegaly.
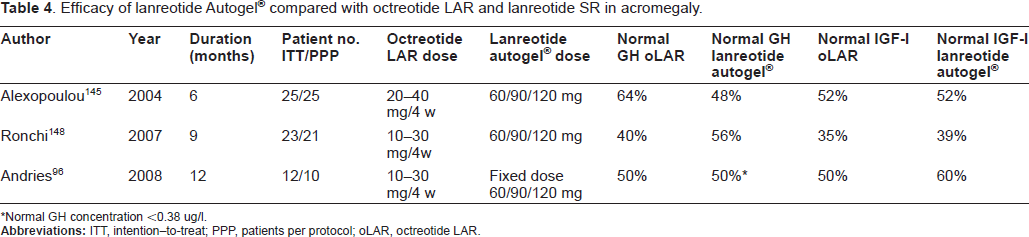
Normal GH concentration <0.38 ug/l.
Side Effects
The most frequent side effects of lanreotide (and other somatostatin analogs) are diarrhea, abdominal pain and nausea. These symptoms start mostly shortly after an injection, decrease subsequently, and tend to diminish in severity on continuing treatment. Table 5 lists the side effects mentioned in clinical studies with the two long-acting formulations of lanreotide. For the slow-release formulation the gastrointestinal side effects were observed in 48% of the patients and for the autogel® formulation in 52%. The most serious complication of somatostatin analogs is cholelithiasis.
The prevalence of somatostatin analogue-induced gallstones varies geographically and may be influenced by dietary, environmental and racial factors. The formation of gallstones involves the inhibition of gallbladder emptying and intestinal motility, the inhibition of the secretion of prokinetic peptides, including cholecystokinin, and the increased intestinal and biliary production of deoxycholic acid, all of which promote the nucleation of cholesterol crystals and their aggregation into stones 102,103We analyzed the occurrence of new cholelithiasis in patients who were already on somatostatin analog treatment, a condition thus not quite comparable to drug-naïve patients with risk of developing gallstones. The incidence of new gallstones was 6% for lanreotide SR and 8.7% for lanreotide Autogel®. These figures are smaller than usually cited in literature, but many patients already had cholelithiasis caused by previous treatment. One study reported a high incidence of symptomatic gallstones, following withdrawal of somatostatin analog therapy, particularly in males. 104
Other side effects were local pain after injection and rarely (less than 1%) the development of nodules at the injection site. However, local infiltration signs did not decrease the efficacy of the drug. Other uncommon side effects included sinus bradycardia, asthenia, headache, pruritus, decreased libido, increased serum bilirubin, fatigue, constipation and hair loss.
The Influence of Lanreotide Autogel® on Clinical Manifestations
Specific aspects of lanreotide action in acromegaly investigated included studies on glucose and insulin metabolism, effects on the cardiac function, tumor growth, the quality of life and predictors of clinical response. These reports are briefly summarized below.
Insulin and glucose homeostasis
GH is important in regulating glucose tolerance and insulin sensitivity. GH counteracts the effects of insulin by inhibiting the phosphorylation of the insulin receptor. Moreover, GH also inhibits the phosphorylation of one of the proximate molecules of the insulin signaling cascade, insulin receptor substrate-1 in response to insulin. 105 Several studies in acromegaly have shown that increased GH induces insulin resistance. 106 However, GH also potentiates the insulin release which is reflected in the high prevalence of high insulin levels both at rest and after glucose challenge. 107 Indeed, many untreated patients exhibit decreased glucose tolerance and more detailed studies have shown reduced insulin-stimulated glucose disposal in muscle and impaired non-oxidative glucose metabolism.108–112 Effects of somatostatin analogs on glucose homeostasis are the resultant of delayed intestinal absorption of carbohydrates, inhibition of the insulin release and increased insulin sensitivity via diminished GH secretion. Results from studies with lanreotide do not differ essentially from earlier data obtained with octreotide. The acute effect of subcutaneously infused lanreotide was studied in healthy subjects. Oral glucose tolerance worsened during the first day of administration, but was restored on day 7 while drug administration continued. 105 In a study in 27 patients the homeostasis model assessment (HOMA) index improved, but not the quantitative insulin check index (QUICKI) index. 113 In a cross-sectional study with 51 acromegalic patients of who 18 were on lanreotide Autogel® the pancreatic β-cell function deteriorated but insulin resistance remained unchanged. 114 The most precise study used the euglycemic hyperinsulinemic clamp. Twenty-four patients were studied at the base line and after 6 month treatment with either octreotide LAR or with lanreotide SR. HbA1c increased significantly. In patients with a normal glucose tolerance at baseline the glucose concentration at 120 minutes increased, together with decreased and delayed insulin response. Insulin sensitivity increased in all 12 clamped patients. The investigators could not demonstrate differences between octreotide and lanreotide, i.e. the effects on GH, IGF-I and insulin were all similar. 115 The effects of other medical therapies currently used for the treatment of acromegaly on glucose metabolism and insulin resistance were recently reviewed. 116 In most studies, not specifically focused on insulin and glucose metabolism, fasting glucose concentrations and/or HbA1c levels did not change significantly when the GH-suppressive medication was changed to lanreotide or when the period of lanreotide administration was compared with the period without GH-suppressive medication.
Cardiac effects
Acromegaly is associated with increased cardiac morbidity and mortality. Recognized cardiac manifestations include chronic cardiac failure due to systolic dysfunction (cardiomyopathy) or isolated diastolic dysfunction.11,13 In addition, our group documented the increased prevalence of regurgitant valvular heart disease. 13 Treatment with somatostatin analogs prevented the worsening of cardiac valve regurgitation. 117 An important question is whether effective GH–suppressive medication can improve the cardiac function. One of the first studies reported on 13 patients treated with lanreotide. In this study there was a parallel decrease in GH and IGF-I and in left ventricular mass index and these data were confirmed in another study.118,119 Octreotide was used in most studies on cardiac function, because this drug was the earliest available for clinical studies. These studies, summarized in a meta-analysis, indicate that effective GH-suppressive medication improves morphological and functional hemodynamic parameters, although medical therapy does not normalize all parameters. 120 These observations concur with results of another study, which compared outcome in long-term surgically cured patients with medically controlled patients, showing better results in the first group 121 suggesting that GH-suppressive therapy in its present form is unable to fully correct cardiac dysfunction. The impact of this finding on long-term mortality in acromegaly is unknown.
Tumor growth
The anti-tumoral effects of somatostatin analogs are linked to the activation of the subtype receptors SSTR1, SSRT2, SSTR4 and SSTR5, which all induce cell cycle arrest. Apoptosis is associated with SSTR3 and possibly also with SSTR2 signaling.69,70 GH secreting adenomas express different somatostatin receptors, as shown for example by a recent study in which 77% expressed SSTR2, 69% SSTR1 and SSTR3 and 60% SSTR5. In the same study, lanreotide inhibited cell proliferation in vitro in 10 out of 13 adenomas. 122 Lanreotide also stimulates apoptosis as was found in surgically removed GH secreting adenomas to 8.7% ± 2.6% in tumors compared to less than 3.5% in controls. 123 The clinical response in terms of GH control and tumor size reduction correlates with the expression of SSTR2.124,125 Preoperative treatment with lanreotide SR for 1-3 months in 104 acromegalic patients led to tumor size reduction in 66%, with a mean decrease of 152 mm3. A decrease in adenoma size of more than 20% was found in 29% of the patients. 126 Other studies in which the decrease in adenoma size could be evaluated are listed in Table 5. The meta-analysis of 14 clinical studies using somatostatin analogs as primary treatment, 36.6% of the patients exhibited a significant reduction in tumor size, with a weighted mean of 19.4%. 127 Factors (not necessarily predictors) associated with tumor shrinkage after primary therapy with somatostatin analogs were post-treatment IGF-I, the age of the patient and the percent GH decrease, 128 and essentially confirming previously reported findings. 126 In another meta-analysis of 44 trials, tumor shrinkage was related to the choice of the somatostatin analog. Octreotide LAR appeared to be more potent than lanreotide SR, with an odds ratio of 9.4. 94 At this time, no data on tumor shrinkage in treatment-naïve patients during lanreotide Autogel® therapy are available. Preliminary data on biochemical remission of acromegaly after somatostatin analogs withdrawal suggest that some well-responsive patients might be cured, but long-term follow up is clearly needed. 129
Side effects during treatment with lanreotide Autogel®.

Quality of life
Quality of life (QoL) is impaired in acromegaly even after successful pituitary surgery predominantly due to persisting joint-related complaints. 130 An early open study on the effect of lanreotide SR on QoL suggested a positive effect of treatment. 131 However, in another study comprising 52 acromegalic patients no differences could be shown between lanreotide-controlled and non-controlled patients using the AcroQoL, a questionnaire specifically developed for acromegaly. Interestingly, in the controlled group, surgically cured patients were much better off than patients controlled with lanreotide. 132 This observation underscores subtle differences between restoration of normal physiology and effective GH-suppressive medication, as found in intensive GH sampling studies in acro-megalic cohorts. 133 Finally, in a study of 93 patients with acromegaly control of GH and IGF-I had a positive impact on the subscale appearance, but overall QoL was severely impaired. 134
Failures of Medical Therapy
About half of patients with acromegaly have still increased IGF-I and/or GH levels under somatostatin analog treatment. Increase of the injection frequency of lanreotide Autogel® to once per 2-3 weeks is mostly not successful. 135 Another approach is to combine somatostatin analog treatment with a dopaminergic agonist.83,84 More effective is combined treatment with pegvisomant as demonstrated by a single center open labeled study. Long-term efficacy of combined treatment was demonstrated in 32 patients who all normalized IGF-I with pegvisomant in a dose of 40-160 mg given once or twice weekly. 136 Two large multicenter studies are respectively ongoing and complete, in which weekly administered pegvisomant is combined with lanreotide Autogel® in patients not controlled during treatment with 120 mg lanreotide Autogel® (ClinicalTrials.gov, NCT 00383708) and daily pegvisomant injections with Sandostatin LAR (Clinical-Trials.gov, NCT 0068029). Preliminary results of the latter study suggest equal efficacy in the two randomized parallel treatment groups towards serum IGF-I normalization, but with a higher incidence of side effects in the combined treatment group. 137 Considering the number of patients included, these studies will most likely answer questions about the efficacy of the combined somatostatin analog and GH-receptor blockage in the treatment of acromegaly. However, both studies did not exclude previous surgery or radiation therapy, so that any conclusions drawn from these studies may not be applicable to primary medical treatment.
The favorable receptor binding profile of SOM230 (pasireotide) suggests that this new drug is a powerful somatostatin analog, which can be used in therapy-resistant cases to the registered somatostatin analogs.138,139 Clinical Phase II studies in acromegaly are now being carried out in the U.S.A. with both the short-acting form as well as the slow-release formulation (ClinTrials.gov NCT000088582, NCT00171730, and NCT00600886). Other somatostatin agonists currently developed were recently reviewed. 140 Potential interesting drugs are chimeric somatostatin analogs. This class of drugs combines dopamine and somatostatin structural elements and retain affinity for specific somatostatin and dopamine receptor subtypes. These new drugs can not only suppress GH (and other pituitary hormones) better than currently clinically used drugs, but may also have much stronger antiproliferative actions, at least in vitro.141,142
Summary and Future Perspectives
Lanreotide Autogel® is an exceptional pharmaceutical achievement, based on the unique property of self-aggregation of lanreotide. The formulation is delivered in prefilled syringes and can be easily injected without medical supervision by the patient or partner after proper training, 143 whereas octreotide LAR requires qualified personnel for administration.
Lanreotide Autogel® controls GH in 58% and IGF-I in 48% of the patients. Compared with octreotide LAR lanreotide SR is less efficacious, but the difference is small. 94 No large-scale data are available for lanreotide Autogel®, a latecomer in this therapeutic field, to make a reliable comparison with octreotide LAR.
In most Western countries lanreotide Autogel® is about 20%-30% more expensive than octreotide. LAR. The associated long-term financial consequence could influence the preference of insurance companies for one of the drugs.
The present formulations of somatostatin analogs can be classified as the second generation of effective GH-suppressive drugs, but these agents are clearly not adequate for all patients, depending on tumor somatostatin receptor status. New somatostatin analogs include pasireotide, which is currently investigated in several trials in the U.S.A., and the potentially powerful chimeric drugs developed by Ipsen SA. These drugs, if successful in phase II-IV studies, will probably take another 5-10 years before becoming available for clinical use by endocrinologists.
At present, patients not controlled by somatostatin analogs should be treated with adjuvant pegvisomant, either as daily injections, as recommended by Pfizer, or as once- or two-weekly injections in a titrated dose, which data in the literature have suggested as sufficient.144,79,136,137 It is to be expected that other GH receptor blocking agents will become available in the future, which might not have the potential drawbacks of pegvisomant. 140
Declaration of Interest
The authors have no conflict of interest and have received no payment in the preparation of this manuscript.