
Abstract
Sjogren's Syndrome (SS) is a chronic autoimmune disease characterized by the presence of xerostomia and xerophthalmia and by the dysfunction of salivary and lacrimal glands. The disease is frequently associated with other systemic manifestations, including vasculitis, pulmonary interstitial disorders and lymphoma. SS constitutes the primary cause of disability and xerostomia can represent an obstacle to deglutition and to oral hygiene, making it difficult for these patients to talk, eat, and swallow. In addition, it can cause tooth decay and recurring candidosis of the oral cavity, as well as premature teeth loss. The treatment of SS is based on the use of artificial tears, saliva substitutes, and lubricants to control the symptoms, and is usually associated with muscarinic agonist drugs such as pilocarpine, especially in cases of severe dryness. Pilocarpine has been proven to increase the secretion of saliva, but its use in clinical practices is highly limited to the short duration of its action, less than 3 hours, which considerably reduces its compliance. There have recently been studies of a new muscarinic receptor agonist, Cevimeline, which has a longer half-life than Pilocarpine (about 5 hours), and has already been commercialised in some countries. The purpose of this article is to review the published literature regarding the pharmacological and clinical properties of this drug, as well as its efficacy, tolerability, and safety in the treatment of xerostomia in patients suffering from primary and secondary SS.
Introduction
Sjogren's Syndrome (SS) is a chronic autoimmune pathology characterised by the presence of keratoconjunctivitis sicca (xerostomia and xerophthalmia) and by the dysfunction of the exocrine glands: salivary glands (parotid and minor glands) and lacrimal glands in particular. The disease is commonly associated with systemic manifestations, including vasculitis, pulmonary interstitial disorders and lymphoma, as well as the involvement of other glands, such as the pancreas and the exocrine glands of the skin and mucous. The SS can exist in a primary form, or associated with other autoimmune disorders (secondary SS) such as rheumatoid arthritis, systemic lupus erythematosus, scleroderma, myositis, autoimmune thyroiditis, and primitive biliary cirrhosis. 10 About 50% of patients exhibit primary form of SS, while the most common secondary form is due to rheumatoid arthritis (about 20%). 5 It is a relatively widespread pathology with a prevalence of 0.5%-1% on the general population, afflicting mainly middle-aged females; with a male:female ratio of 1:9. 11 It generally affects middle-aged subjects, with a peak in patients between 30 and 60 years.
On a physiopathological level, SS is defined as an autoimmune exocrinopathy, which can alter the functions of not only the salivary and lacrimal glands, but also the exocrine glands of the female genital tract, the skin, nose, trachea and the gastroenteric system. Histologically, inflammatory damage is documented by lymphocitary infiltrate, monocitary and plasmacellular at CD4+ pattern. There is no current clinical correlation between the graveness of the symptoms and permanent damages to the glandular tissues. 18 Therefore, other physiopathological hypotheses have been put forward: the first probable mechanism is linked to the possibility that cellular dysfunction is mediated by apoptotic damages, preceded by lymphocitic infiltration, and that the production of typical autoantibodies (ANA and anti-Ro/SSA and anti-La/SSB) is triggered by intracellular epitope. Another hypothesis is correlated to the manifestation of an organ-specific antibody pattern represented by the muscarinic M3 receptor. These antibodies can cause glandular damages through mechanisms similar to the anti-thyroid antibodies, stimulating the thyroid receptors in patients with autoimmune thyroiditis. 30 At the serological level, the prevailing alterations observed are the positivity of the anti-Ro/SSA and anti-La/SSB antibodies, the ANA and the rheumatoid factors. At the histopathological level, there is the CD4-positive T-lymphocyte infiltration of the minor salivary glands of the lower lip.
Sicca syndrome constitutes the primary cause of disability in affected patients since it conditions their quality of life. In fact, xerostomia can represent, other than a subjective symptom, an objective obstacle to deglutition and to oral hygiene, making it difficult for these patients to talk, eat, and swallow. In addition, it can cause tooth decay and recurring candidosis of the oral cavity, as well as premature teeth loss.5,11,18
The treatment for this disease is based on the use of artificial tears, saliva substitutes, and lubricants to control the symptoms, and is usually associated with muscarinic agonist drugs such as Pilocarpine, especially in cases of severe dryness.18,19 Only rarely, as in disabling cases, it is necessary to resort to surgical sutures of the punctum in order to prevent the rapid loss of the little lacrimal liquid produced and to irrigate the salivary glands with corticosteroids. Pilocarpine has been proven to increase the secretion of saliva, but its use in clinical practices is highly limited to the short duration of its action, less than 3 hours, which considerably reduces its compliance. 5 There has recently been studied a new muscarinic receptor agonist, cevimeline, which has a longer half-life than Pilocarpine (about 5 hours), and has already been commercialised in some countries.
The purpose of this article is to review the published literature regarding the pharmacological and clinical properties of this drug, as well as its efficacy, tolerability, and safety in the treatment of xerostomia in patients suffering from primary and secondary SS.
Mechanism of Action, Metabolism and Pharmacokinetic Profile
Cevimeline, a quinuclidine derivative of acetylcoline, acts as a muscarinic receptor agonist. Its effects on salivation depends mainly on the direct stimulation of the M3 receptors of the salivary glands.17,27,31
It is common knowledge that salivation and lacrimation are regulated by the acetylcholine mediators on the receptors, and muscarinic effects on the M1 and M3 subcategories, with a prevalence of 93% of the M3 subcategory on the parotid glands.
Recent studies have revealed that in SS autoantibodies are produced to fight against the subcategory M3 receptors (anti-M3R), and that such mechanism can be the cause of saliva reduction.8,12
The pharmacodynamic profile of cevimeline has been experimented both on animals (rats, mice, guinea pigs, cats and dogs) and on humans (healthy subjects and subjects afflicted with SS). The link between quinuclidinyl benzilate in rats and mice to the muscarinic receptors of the submandibular glandular membrane and the sublingual membrane seems to be saturable, with a constant dissociation equal to 1.2 μmol/L. and can, therefore, increases the secretion of saliva. 13 The dominant characteristics of this drug compared to Pilocarpine are its longer lasting effect on salivation, from 1.4 to 1.8 times longer in rats, and twice as long in dogs. 17 The studies on rats have also demonstrated that cevimeline is able to induce lacrimal secretions without having to increase the intake of water with the dosage necessary for the induction of salivation. 25 The doses used in experiments on animals provoked the increase of salivation (3-10 mg/Kg) without causing any particular systemic effects when the treatment was administered orally. On the other hand, effects on the central nervous system, peripheral, respiratory, and cardio-circulatory systems, as well as the genital-urinary and gastroenteric systems were observed at dosages greater than 10 mg/kg when administered intravenously.1–4,22 Instead, oral doses ≥ 10 mg/kg brought on mydriasis in mice and rats.13,25
The increase in salivary secretions has been widely studied in several animals, and has also been confirmed in experimental models of Sjogren's Syndrome in rats and mice with effective doses of 10-30 mg/kg, without inducing tolerance1–4,13–15,17,22
Studies on human subjects have shown that a single dose of 30-50 mg of cevimeline on healthy subjects produces a marked increase in the secretion of saliva, with a peak at 1-3 hours after oral administration. 15
The oral assumption of a single dose of cevimeline at 30 mg by 12 females with SS provokes a significant increase in their salivary secretions (p = 0.0496); from 0.4 mL/min at baseline to 0.13 mL/min after 90 minutes. 27
Pharmacokinetic aspects of cevimeline have been studied both on healthy volunteers and sick subjects. The peak level of the maximum plasmatic concentration (Cmax) is at 59.9 ng/mL, with a mean time of 1.8 hours in healthy subjects who were given 30 mg of cevimeline three times a day for 7 days, without the accretion of the drug nor its metabolism.7,21 Cmax in the elderly (62-80 years) taking 30 mg of cevimeline is 90.8 ng/mL after a median of 1.5 hours and with an area under the plasma concentration vs time curve (AUC∞) equal to 774.6 ng·h/mL, while the Cmax of patients with SS is 91.6 ng/mL after 1.5 hours with an (AUC∞) median of 711.1 ng·h/mL. 15 The consumption of food reduces absorption by 17.3%. The volume of distribution of cevimeline is about 6 L/kg with a link to the plasmatic proteins inferior to 20%. Metabolism is linked to cytochrome P450 (CYP) and to the isoenzymes CYP2D6 and CYP3A3/4 in particular; they are, however, not involved in vitro, hence they do not inhibit the CYP1A2, CYP2A6, CYP2C9, CYP2C19, CYP2D6, CYP2E1 and CYP3A4. 14 In the 24 hours following the consumption of 30 mg of cevimeline, 87% is eliminated, 16.0% is not metabolised, 35.8% is metabolised at 8.7% trans-sulfoxide and 14.6% cis-sulfoxide as glucuronic acid of cevimeline, 7.7% as glucuronic acid of trans-sulfoxide metabolite and 4.1% as N-oxide of cevimeline. 7 The derivatives of cis and trans sulfoxides are not active drugs. 33 A dose of 30 mg of cevimeline three times a day, administered to healthy subjects, shows a mean elimination half-life of 3.3 hours. The same dose in patients with SS has a t1/2β of 5.1 hours14,15,21,27 Elimination is mostly by means of the urinary tract; after one week of treatment, 97.3% is eliminated through the urine and 0.5% is excreted through the faeces. 29
Metabolism in subjects with liver or renal deficiency has not been studied, just as the differences in ethnicity has not been taken into consideration either. Instead, Cevimeline must be prescribed with caution for subjects with suspected or confirmed CYP2D6 deficiency. 7 Therefore, the concomitant use with other drugs can trigger a pharmaco-kinetic interaction, which can lead to the inhibition of CYP2D6 and CYP3A3/4, causing the metabolism of cevimeline to slow. Alternately, the pharmaco-dynamic interactions can be brought on with beta-adrenergic receptor antagonists, which, when taken with other drugs, can provoke alterations in the heart conduction system, and with alpha-sympathico-mimetic drugs or anti-muscarinic drugs. 7
Adverse effects have been reported in phase II studies, though none of which is very grave; the most common are: hyperhydrosis which is linked to the muscarinic action of the drug, and gastrointestinal disorders such as nausea, diarrhroea and cephalalgia.
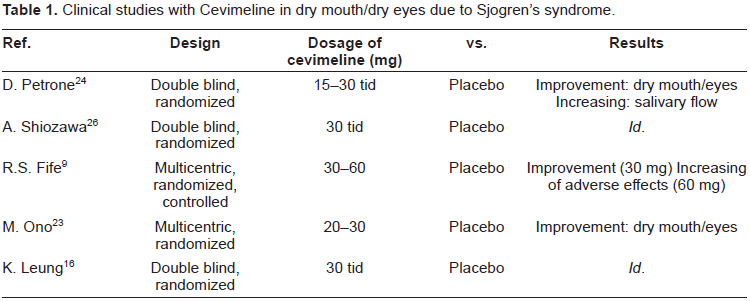
Clinical studies with Cevimeline in dry mouth/dry eyes due to Sjogren's syndrome.
Clinical Studies
Several phase II and III studies have been conducted on the use of cevimeline in patients suffering from SS. The studies, most of which were double-blind, randomised and controlled, assessed the profiles of efficacy and tolerability with dosages of 15, 30 and 60 mg three times a day versus the placebo.
The first was a double-blind, randomized study, published in 2002 by Petrone in Texas. This study evaluated the efficacy end points of cevimeline at doses of 15 and 30 mg three times daily, taking into consideration both the global assessment of dryness and the subjective global assessment of dry eyes and dry mouth, plus the measurement of lacrimal and salivary flows. The results confirmed a significant improvement in dry eyes and mouth, and an increase in salivary flow at a dosage of 30 mg three times daily. Furthermore, the study also reported an improvement in ocular parameters with respect to the placebo (evident in lacrimal flow and Schirmer's test). Common side effects noted were cephalalgia, increase in perspiration, abdominal pains and nausea. 24
A few months later, a similar double-blind, randomized and controlled study was published in Japan, confirming the efficacy and safety of cevimeline at 30 mg three times a day for 4 weeks and 52 weeks. 26
Another multicentric American study, published in 2002 and also double-blind, randomized and controlled, investigated dosages of 30 and 60 mg three times a day for 6 weeks. This study reported the effects of cevimeline on xerostomia, and by means of a visual analogic scale, objective assessments and measurements of salivary flow, demonstrated that the results of 30 mg doses three times a day were effective in controlling dry mouth, with a good tolerability profile. Dosage of 60 mg, although effective, brought on a greater number of adverse effects. 9
In 2004, the use of Cevimeline with water (30 mg in 100 ml of water three times a day) was tested by a Japanese group, considering the frequent onset of adverse effects. The experiment, initially conducted on 11 healthy volunteers and then subsequently on 5 patients suffering from SS, showed an increase in salivary flow in 3 subjects out of 5, without any onset of side effects. No other similar case studies is available with a greater number of patients. 28
There was another multi-centric Japanese study (2004), which tested the effects of Cevimeline on xerophthalmia. Sixty patients were enrolled and randomized into three groups: the placebo group, the group receiving 20 mg three times daily, and the third group receiving 30 mg three times daily. Assessment made at pre-treatment (2 and 4 weeks) were based on the visual analogue scale (VAS) of symptoms, the rosa bengala test, Schirmer's test, clinical exams on the state of the keratoconjunctival epithelium and assessment of tear dynamics. The results from this study demonstrated the efficacy of 20 mg doses three times daily in the improvement of symptoms of dry eyes. 23
In 2008 the first investigation on the safety and efficacy of Cevimeline on the Chinese population was published. Evaluations on 30 mg three times a day were made at 0 and 10 weeks of treatment, and after 4 weeks of wash-out, the following questionnaire was evaluated: xerostomia inventory (XI), general oral health assessment index (GOHAI), ocular surface disease index (OSDI) and the medical outcomes short form (SF-36), accompanied by clinical data and by sialometry. The result showed a significant improvement in XI and in GOHAI, as well as objective data of sialometry. However, there was no improvement in salivary flow or xerostomia. The SF-36 score, based on patients with SS, did not improve after treatment. 16
Safety
Cevimeline, at dosages of 15 and 30 mg three times daily, has proven to be well tolerated. Nausea, diarrhea, cephalalgia and hyperhydrosis represent the most common side effects. At least one event of adverse effect on 82.2% of the subjects treated in the Texan study was reported in their study in 2002, but such events did not necessitate the suspension of treatment if not in the 13.8% of subjects treated with 15 mg and 16.1% of those treated with 30 mg. Severe side effects were verified in 1.5% of those treated with 15 mg and 1.6% of subjects treated with 30 mg. It must, however, be noted that such adverse effects, even the serious ones, were also reported in the placebo group with a percentage of 25.7%. 24
Safety of Cevimeline in clinical studies for Sjogren's syndrome.
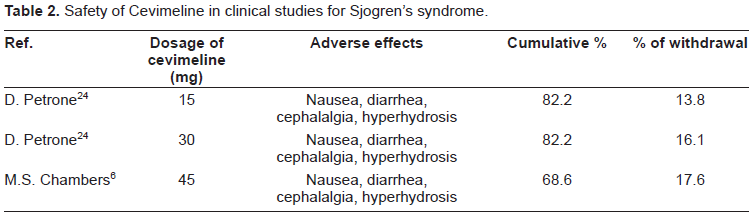
The safety of Cevimeline, 45 mg three times a day, has also been studied in subjects with glandular dysfunction after having undergone radiation therapy for neoplasia of head and neck. Likewise, in this study, which is open-label and long-term, 68.6% of the 255 patients studied for 52 weeks experienced at least one form of adverse effects, but only 17.6% had to interrupt the treatment. 6
Product specifications, available on-line, give an extended list of side effects during the pre-marketing stage, the most common of which are represented by muscarinic effects: sweating, cephalalgia, nausea and dyspepsia, sinusitis, infection of the upper respiratory system, rhinitis and diarrhea. In the postmarketing stage, only cholecystitis is listed as a side effect.
Contraindications of Cevimeline are represented by flare of bronchial asthma plus all the other conditions in which myosis is not desirable, such as in glaucoma at closed angle, and in acute iridocyclitis, as well as in the hypersensitivity noted for the constituents.
Particular attention must be given to patients suffering from cardiopathy such as cardiac failure and ischemic cardiopathy since they can, theoretically, provoke alterations in rhythm and cause sudden hemodynamic changes.
Patients with pulmonary diseases, in which Cevimeline can trigger an increase in air resistance and bronchial secretions, must be treated under strict control.
Precautions in the use of Cevimeline is critical in subjects with a medical history of renal lithiasis and cholecystitis, as Cevimeline can precipitate episodes of cholecystitis, cholangitis, and renal colic due to its effect on smooth musculature. 7 Cevimeline can also alter the visual acuity, especially at night, in subjects with macular alterations.
In its pre-marketing stage, the carcinogenic potential of Cevimeline has been tested in mice and rats, showing an increase in the incidence of uterine adenocarcinoma in rats treated with doses 8 times greater than the therapeutic dosage (100 g/kg/die). There was no evidence, however, of mutagenicity and clastogenicity in other bacteria assay in vitro and other live studies. 7 Furthermore, Cevimeline did not seem to compromise reproductiveness in rats. 7 Neither studies nor case reports have been made on humans in this respect, thus Cevimeline is not recommended for pregnant women or for patients wishing to become pregnant after the initial consumption of this drug. There is no data regarding the excretion of breast milk. 7 In addition, Cevimeline is not recommended to children under 18 since its efficacy and safety has not been determined for those of pediatric age. The use of Cevimeline in geriatric age is limited to cases with the appropriate comorbidity. 7
Efficacy
Cevimeline, at a dosage of 30 mg three times daily, appears to be effective in controlling xerostomia in patients suffering from SS. 24
It has proven to be particularly more effective in subjects with minor structural damages to the glands (biopsy of the minor salivary glands with scores between 0 and 2, and sialography with scores equal to 0).20,32
Patients Preferences
There is no existing published literature on the preference of the consumption of Cevimeline on the part of the patients. For its pharmacokinetic properties, the consumption of Cevimeline in conjunction with meals is counter-productive since it reduces absorption. Cevimeline was administered in tablets orally in most of the studies conducted, after meals three times a day in compliance with the treatment: low percentage of missed tablets (10%-25%). 28
Cevimeline in tablets to be administered orally is the type currently on the market.
In comparison to Pilocarpine, which has the same indications but must be taken four times daily, Cevimeline is taken three times a day, which is certainly more convenient for the patient. Moreover, the fewer the tablets of consumption necessary, the less likely it is to miss a tablet, thus making the treatment more effective.
Place in Treatment
Cevimeline can be used to treat xerostomia in patients with SS at a dosage of 30 mg three times a day. Its efficacy has been demonstrated by well conducted studies, however, its use is limited, although only slightly, by the onset of adverse effects such as hyperhydrosis, cephalalgia, nausea and intestinal disorders.
A published study on the predictive factors of the efficacy of treatment with Cevimeline has made it possible to individualize the categories of patients with the highest probability of response to treatment, including subjects with low bioptic scores from the salivary glandular biopsy, and scores inferior to sialography, as well as those patients who do not present the anti-M3R antibodies. 32
Conclusion
Cevimeline has been used, at a dosage of 30 mg three times daily, in the treatment of symptoms of keratoconjunctivitis sicca, xerostomia in particular, in patients afflicted with SS.
A fair number of clinically controlled trials vs placebo have been well conducted, showing the efficacy of Cevimeline in reducing xerostomia and in blocking the reduction of salivary flow, without inducing drug tolerance.
Such studies have also demonstrated that the safety of Cevimeline is due to its tolerability at the dosages tested, and the higher incidence of adverse effects compared to the placebo.
Minor side effects such as cephalalgia, diarrhea, nausea, increase in perspiration, as well as rhinitis and upper respiratory infections reported in patients with SS, are associated with the pharmacological actions of Cevimeline, especially by its muscarinic activities. Cevimeline is currently available in several countries, among which are the United States (since 2000), Japan and Taiwan.
Disclosures
The authors report no conflicts of interest in their work.
Footnotes
Aknowledgment
The Authors would like to thank Mrs Trisha Pham for the revision of the manuscript.