
Abstract
Excessive sleepiness (ES) is responsible for significant morbidity and mortality due to its association with cardiovascular disease, cognitive impairment, and occupational and transport accidents. ES is also detrimental to patients’ quality of life, as it affects work and academic performance, social interactions, and personal relationships. Armodafinil is the R-enantiomer of the established wakefulness-promoting agent modafinil, which is a racemic mixture of both the R- and S-enantiomers. R-modafinil has a longer half-life and is present at higher circulating concentrations than the S-enantiomer following chronic administration of modafinil and may therefore be the enantiomer predominantly responsible for the beneficial effects of the racemic compound. Armodafinil has been approved by the Food and Drug Administration for the improvement of ES associated with narcolepsy, shift-work disorder, and obstructive sleep apnea following a program of randomized, placebo-controlled clinical trials. This comprehensive medication review discusses the pharmacologic profile of armodafinil and the current evidence regarding its efficacy, safety, and tolerability; appraises patient-reported outcomes data; and suggests additional indications in which armodafinil may be of use.
Introduction
Excessive sleepiness (ES) is drowsiness that occurs at inappropriate times and may happen for myriad reasons including insufficient sleep (due to insomnia or poor sleep habits), interrupted sleep (as experienced by patients with obstructive sleep apnea [OSA]), neurologic disorders (e.g. narcolepsy, dementing illnesses, or stroke), sleep-timing issues (e.g. the circadian rhythm disorders shift-work disorder [SWD] and jet lag), and side effects from pharmacologic agents (such as some antidepressants and pain medications).
A dramatic example of ES associated with OSA occurred in February 2008 when a regional jet overflew its destination on a regularly scheduled mid-morning flight between the Pacific islands of Oahu and Hawaii. Go! flight 1002 left Honolulu airport at 0916 hours without incident. When the Hilo air-traffic controller radioed the aircraft with landing instructions only 24 minutes later, neither the 23-year-old first officer nor the 53-year-old captain responded. Go! flight 1002 flew past the Kona airport and continued over the Pacific Ocean for 18 minutes for a distance of approximately 26 miles before the pilots finally awoke and responded. The captain reported that he often intentionally napped during flights and was subsequently found to have OSA. 1
ES is associated with significant morbidity and mortality, independent of accompanying conditions. For example, ES has been linked with a greater risk of developing cardiovascular disease and death from cardiovascular disease 2 ; a recent study has reported that this is not as a result of coronary artery calcification. 3 There is some evidence, however, that ES is implicated in hypertension, which could be involved in the pathology of heart disease in these patients. 4 For example, ES may promote hypertension in patients with OSA, as patients with OSA and ES who are treated effectively for these conditions experience reductions in blood pressure, while those with OSA in the absence of ES do not experience reductions in blood pressure.5–8 One possible mechanism for ES-related hypertension may be increased circulating catecholamines resulting from a chronically increased sympathetic drive brought about by attempting to remain awake, as suggested by studies of the influence of posture in preserving alertness.9,10
ES and hypoxia both play a role in the cognitive impairment experienced by patients with OSA; however, a study comparing cognitive impairment in patients with chronic obstructive pulmonary disease (who experience hypoxia but not ES) and patients with OSA and ES (who experience both hypoxia and ES) showed that patients with OSA had poorer attention and vigilance, suggesting that the cognitive deficits in OSA may be due to ES. 11
Cognitive impairment and falling asleep as a result of ES are thought to be responsible for a large proportion of the motor vehicle crashes that occur in patients with OSA.12–16 In addition, cognitive impairment as a result of ES in the absence of falling asleep has been shown to impair the flight performance of sleep-deprived military pilots17,18 and to impair driving performance. 19 Furthermore, ES as a result of sleep deprivation, circadian rhythm misalignment, or OSA has been cited as a causative factor in a number of air and train crashes.1,20–22 Having both ES and snoring doubles an individual's risk of experiencing an occupational accident compared with those who have either of these conditions in isolation. 23
In addition to its detrimental effects on patient health, ES may impinge on activities of daily living. A study by Sforza and colleagues 24 reported that ES contributed more significantly to impairment in all domains of the Medical Outcomes Study Short-Form (36-item) Health Survey (SF-36) than sleep-disordered breathing. ES may also lead to unemployment, relationship issues, reduced social interaction, and poor performance at work, school, or college. 25 For example, Mulgrew and colleagues 26 demonstrated that patients with ES experience significant limitations at work in terms of time management (p < 0.001), mental–interpersonal relationships (p < 0.001), and work output (p < 0.001).
There are two main objective measures of ES employed by sleep clinicians: the Multiple Sleep Latency Test (MSLT) and the Maintenance of Wakefulness Test (MWT). The MSLT consists of four or five 20-minute nap opportunities spaced 2 hours apart and measures the duration from the start of the nap period to the first signs of sleep in the patient. 27 The MWT also consists of multiple 20- to 40-minute potential nap opportunities spaced over the course of a day and is performed in a darkened room in a semi-reclining position. 28 While the MSLT assesses the patient's ability to fall asleep, the MWT conversely assesses their ability to stay awake. Sleep latency is judged to be the period from the beginning of the test to the first of three consecutive epochs of stage 1 sleep or one epoch of any other sleep stage. Conventionally, the onset of sleep during laboratory-based evaluations of ES is assessed using an electroencephalogram, left and right eye electro-oculograms, a mental/submental electromyogram, and an electrocardiogram. 28
ES can also be assessed subjectively using the Epworth Sleepiness Scale (ESS), the Karolinska Sleepiness Scale (KSS), and the Stanford Sleepiness Scale (SSS).29–31 The ESS is the most commonly used scale as it is a simple self-report test that can be finished in as little as 2 minutes. The patient completes a set of questions regarding their perceived ES in a series of situations such as sitting and reading or talking with friends. Total scores range from 0 to 24, with a score of ≥10 being indicative of ES. 31 As the ESS allows a patient to recall ES that has occurred over a number of preceding weeks, it is perceived to give a more accurate diagnosis than the KSS and SSS, which only allow assessment of ES at a single point in time. 32
Armodafinil is the R-enantiomer of the established wakefulness-promoting agent modafinil, which is a racemic mixture of the R- and S-enantiomers. 33 The half-life of R-modafinil is three times longer than that of S-modafinil (14 hours versus 3-4 hours, respectively).34–36 Patients receiving chronic treatment with racemic modafinil have threefold higher circulating levels of R-modafinil than of S-modafinil.34,35 The prolonged circulation of R-modafinil may mean that the majority of effects attributed to modafinil are due to R-modafinil; this hypothesis resulted in further investigation of R-modafinil (armodafinil) in patients with a variety of disorders.37–39 Further to this, armodafinil was approved by the Food and Drug Administration in June 2007 for the improvement of wakefulness in patients with ES as a result of OSA, narcolepsy, and SWD. 33
Pharmacology
The chemical names for armodafinil are 2-[(R)-(diphenylmethyl)sulfinyl]acetamide and 2-(R-benzhydryl-sulfinyl)acetamide. 33 The chemical structure of armodafinil is shown in Figure 1. At the time of publication, armodafinil is not yet marketed in the USA; however tablets containing armodafinil 50, 150, or 250 mg have been approved by the FDA. Patients with narcolepsy or OSA are usually prescribed armodafinil 150-250 mg each morning, while patients with SWD take armodafinil 150 mg 1 hour before the start of their shift.
Structure of armodafinil.
Pharmacodynamics
As armodafinil is an enantiomer of modafinil, much of the following information has been extrapolated from data concerning modafinil. The exact mechanism of action of armodafinil is unknown, although modafinil has some effect on dopaminergic, noradrenergic, and serotonergic receptors.40–42 However, these effects are not well characterized and although ex vivo assays have shown that armodafinil binds to the dopamine transporter and inhibits dopamine reuptake, resulting in increased extracellular dopamine levels in some animal brain regions, armodafinil is not a direct nor an indirect dopamine receptor agonist. 33 Modafinil is known to promote activation of the central nervous system via the hypothalamus, prefrontal cortex, and the anterior cingulate cortex.43,44 Hypocretin (also referred to as orexin) is a neuropeptide that is thought to prevent inappropriate changes in consciousness.45,46 Hypocretin-producing neurons are located within the hypothalamus and project into different brain regions. It is theorized that modafinil activates these neurons to release dopamine and norepinephrine to promote wakefulness and may also inhibit reuptake of these neurochemicals.47,48 However, research in a hypocretinnull mouse model has indicated that the presence of hypocretin is not required for modafinil to have wakefulness-promoting effects. 49 There are further clues to the mechanism of action of armodafinil through research conducted with modafinil. For example, haloperidol and α-methyl-p-tyrosine antagonize the effects of amphetamines but do not block the effects of modafinil, indicating that armodafinil has a different mechanism of action to these drugs. 50 In addition, recent work in rats has indicated that modafinil promotes arousal by increasing electrical coupling at gap junctions.51,52 The metabolites of armodafinil–-modafinil sulfone and R-modafinil acid–-do not contribute to its wakefulness-promoting effects. 33 It appears that additional work is required before the mechanism of action of modafinil and armodafinil is completely elucidated.
Pharmacokinetics
The pharmacokinetics of armodafinil have been characterized in a pooled analysis of three separate randomized studies. In total, 119 healthy subjects received single or multiple doses of armodafinil 50 to 400 mg once daily for up to 14 days. 53 In addition, the pharmacokinetics of armodafinil and modafinil have been compared directly in a single-dose study of healthy male volunteers undergoing acute sleep loss. 54 During this 2-day laboratory assessment, male volunteers aged 18-40 years with stable sleep/wake schedules were randomized to receive 100 mg (n = 18), 150 mg (n = 18), 200 mg (n = 17), or 300 mg (n = 18) of armodafinil, 200 mg of modafinil (n = 18), or placebo (n = 18) in the evening and were then prevented from sleeping until 1100 hours the next day. MWT assessments, blood samples, and psychomotor vigilance tasks were performed during the night. The pharmacokinetic parameters of armodafinil and modafinil given to healthy individuals in the postprandial state are shown in Table 1.
Pharmacokinetic parameters of armodafinil and modafinil following administration of single doses with food in healthy young men (reproduced with permission from Dinges et al. 2006).54
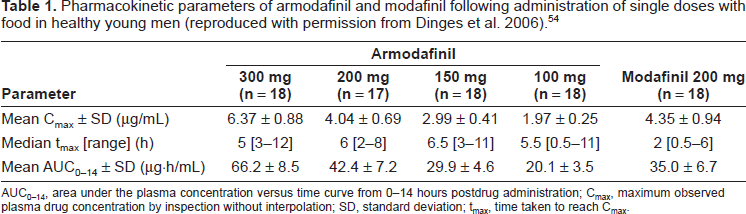
AUC0-14, area under the plasma concentration versus time curve from 0-14 hours postdrug administration; Cmax, maximum observed plasma drug concentration by inspection without interpolation; SD, standard deviation; tmax, time taken to reach Cmax.
Systemic exposure to armodafinil was proportional to its concentration at administration and no changes in kinetics were observed when this agent was administered at doses ranging from 50 to 400 mg over a 12-week period. 53 With chronic administration of armodafinil, steady state was reached within 7 days. 53 On Day 7 and Day 14 of chronic administration, systemic exposure to armodafinil was 1.8 and 1.7 times higher, respectively, than achieved with single doses. 53 After single or multiple doses of armodafinil, the pharmacokinetics of its metabolite R-modafinil acid paralleled those of the parent compound but at approximately tenfold lower concentrations. The time (tmax) to attain peak plasma concentration (Cmax) and the apparent terminal half-life of R-modafinil acid were similar to that of armodafinil. 53 Concentrations of modafinil sulfone were approximately 33% and 56% of that of the parent drug after single-dose and multiple-dose administration, respectively. The terminal half-life of modafinil sulfone was considerably longer on Day 14 than that of armodafinil (39 hours versus 17 hours, respectively). 53
The tmax of armodafinil 200 mg was 3-4 hours later than that for modafinil 200 mg and the decline from Cmax was slower for the R-enantiomer. 54 These differences between armodafinil and modafinil are due to the presence of the short-lived S-enantiomer in the racemic compound, which means that the Cmax for modafinil would need to be substantially higher than that of armodafinil in order to maintain comparable late-day exposure. 54
Absorption
Oral armodafinil is readily absorbed, with Cmax being achieved in approximately 2 hours, although, as shown in Table 1, this may be delayed by 2-4 hours if armodafinil is taken with food.53,54 Food has no effect on the overall bioavailability of armodafinil when compared with the fasting state. The absolute oral bioavailability of armodafinil has not been determined due to its aqueous insolubility, which precludes intravenous administration. 33
Distribution
Armodafinil has an apparent volume distribution of approximately 42 L after single doses and 47 L after 14 days’ administration. 53 As these values are approximately equal to the estimated total water content of the human body, the volume distribution of armodafinil indicates that this wakefulness-promoting agent is widely distributed outside the vasculature but does not have a high affinity for tissues. 53 It is unlikely that armodafinil interacts with highly protein-bound drugs, although it does bind moderately with albumin. 33
Metabolism
Armodafinil undergoes hydrolytic deamidation, S-oxidation, and aromatic ring hydroxylation, with subsequent glucuronide conjugation of the hydroxylated products. As amide hydrolysis is a noncytochrome P450 (CYP)-related pathway, the pharmacokinetic profile of armodafinil is unlikely to be affected by medications that are metabolized by or interact with the CYP enzymes. 33 However, the pharmacokinetic profile of armodafinil may mean that this wakefulness-promoting agent affects medications that are metabolized by or interact with the CYP1A2, CYP219, or CYP3A4/5 enzymes.
Elimination
Modafinil data indicate that elimination of armodafinil may occur predominantly through metabolism in the liver, with < 10% of the parent compound excreted in the urine. 33 After oral administration, armodafinil exhibits an apparent monoexponential decline from its peak plasma concentration with an apparent terminal half-life of approximately 15 hours. 53 By contrast, the presence of the short-lived S-enantiomer in the racemic compound results in a biphasic decline in modafinil plasma concentrations.35,36 The oral clearance of armodafinil is reported to be 39 mL/min after a single dose and 33 mL/min after repeated administration for 14 days.33,53 Oral clearance of modafinil was reported to be reduced (~20%) in two studies of elderly patients (mean age 63 years and 82 years). This finding may be in part due to the effects of aging but may also be attributed to the number of concomitant medications taken by elderly patients. As these results indicate that clearance of modafinil is reduced in the elderly, it is likely that this will also be the case with armodafinil. 33 The pharmacokinetics of armodafinil were not significantly altered in patients with chronic renal failure; however, in the presence of hepatic impairment, modafinil clearance was decreased by about 60% and steady-state concentrations were doubled. Therefore, until the pharmacokinetics of armodafinil are better characterized in this regard, armodafinil should be used at reduced doses in patients with severe hepatic impairment. 33
Drug–drug interaction profile
The drug-drug interaction profile of armodafinil has been reported recently in a study of healthy subjects that based its selection of specific probe substrates on the known in vivo and in vitro drug profile of modafinil. 55 CYP enzymes are membrane-bound proteins that catalyze the metabolism of multiple substrates. For example, CYP3A4 metabolizes, among other substrates, benzodiazepines and immunosuppressants, while CYP2C19 metabolizes proton pump inhibitors and antiepileptic drugs. 56 Modafinil has been shown to have the potential to induce CYP1A2, CYP3A4, and CYP2B6, to suppress CYP2C9, and to inhibit CYP2C19.57,58 In common with modafinil, armodafinil moderately induced CYP3A4 activity in the intestine and liver, as shown by reductions in systemic exposure to oral and intravenous midazolam (by 32% and 17%, respectively) and increased systemic exposure to 1‘-hydroxymid-azolam following prolonged administration of armodafinil. Armodafinil also moderately inhibited CYP2C19 activity, as indicated by decreased area under the concentration versus time curve and Cmax values for the principal metabolite of omeprazole – 5‘-hydroxyomeprazole – and increases in the median ratio of omeprazole: 5‘-hydroxyomeprazole after administration of armodafinil. Unlike modafinil, armodafinil was shown not to affect CYP1A2 activity, as it had little effect on the tmax and total oral clearance of caffeine and did not change systemic exposure to caffeine in healthy subjects. 55
Data from studies of modafinil indicate that steroidal contraceptives may have reduced effectiveness when used with this wakefulness-promoting agent and for 1 month after its discontinuation. Patients should thus be advised to use alternative or additional methods of contraception when taking armodafinil. 59 Similarly, blood levels of the immunosuppressant drug ciclosporin may be reduced when used with armodafinil. Monitoring of circulating ciclosporin concentrations and appropriate dose adjustment for ciclosporin should therefore be considered when these drugs are used concomitantly. 33
Summary of pharmacologic findings
Armodafinil is the R-enantiomer of modafinil. Both armodafinil and modafinil are wakefulness-promoting agents with an unknown mechanism of action, although it is thought that modafinil may produce its effects via the hypocretin system through dopamine- and/or norepinephrine-related pathways, or by increasing electrical coupling at gap junctions.47,48,51,52
Armodafinil achieves its Cmax within approximately 2 hours in the fasted state and 4-6 hours in the postprandial state.53,54 The tmax of armodafinil is 3-4 hours later than that of modafinil, meaning that it may have prolonged wakefulness-promoting effects later in the day than modafinil. 54
Armodafinil appears to be widely distributed in the body, does not have a high affinity for tissues, and is unlikely to interact with highly protein-bound drugs.33,53 Armodafinil is metabolized by amide hydrolysis, a CYP450-independent pathway, and is therefore unlikely to be affected by medication that interacts with CYP enzymes. 33 Armodafinil has been shown to induce CYP3A4 activity and moderately inhibit CYP2C19. 55 This wakefulness-promoting agent is thought to be eliminated predominantly by the liver and demonstrates a monoexponential decline from its Cmax with a terminal half-life of approximately 15 hours.33,53
Efficacy
Preclinical
Armodafinil 100 mg/kg was found to have equivalent wakefulness-promoting effects to D-amphetamine 1 mg/kg when injected intraperitoneally into rats. 60 Armodafinil 100 mg/kg and D-amphetamine 1 mg/kg both increased latency to the onset of consolidated sleep in rats. However, intraperitoneal injection of D-amphetamine 1 mg/kg resulted in rebound hypersomnolence, as indicated by decreases in brief awakenings from sleep and increases in both nonrapid eye movement sleep (NREMS) as a percentage of total sleep time and NREMS bout duration. These changes are characteristic of sleep deprivation and were not experienced by the rats administered armodafinil 100 mg/kg or 300 mg/kg in this study. 60 Furthermore, while D-amphetamine increased body temperature and the intensity of locomotor activity during wake periods, armodafinil 100 mg/kg did not significantly affect physiologic or behavioral parameters compared with a sterile methylcellulose vehicle placebo in the animals assessed. 60
Armodafinil administered at a high dose (300 mg/kg) had greater wakefulness-promoting effects than D-amphetamine and did not increase locomotor activity; however, this higher dose of armodafinil did result in a statistically significant decrease in body temperature (p < 0.001) compared with the methylcellulose vehicle. 60 Administration of armodafinil at a low dose (30 mg/kg) resulted in significantly increased locomotor activity (p = 0.002) and significantly increased body temperature (p = 0.006) compared with the vehicle solution. 60
Clinical
The efficacy of armodafinil in combating ES has been assessed in one single-dose study in healthy subjects and in four 12-week randomized, placebo-controlled clinical trials–-one study in patients with SWD, one study in patients with narcolepsy, and two studies in patients with residual ES associated with OSA.37–39,61–63 A summary of the results of these clinical trials is given in Tables 2 and 3. In addition, there are two ongoing open-label trials of armodafinil: one in trial-naïve patients (with narcolepsy, OSA, or SWD) and one extension study in patients who completed any of the randomized trials and were able to participate for 12 months or longer.
Average baseline sleep latency and change from baseline at final visit in patients given armodafinil for a variety of conditions (MWT and MSLT in minutes).
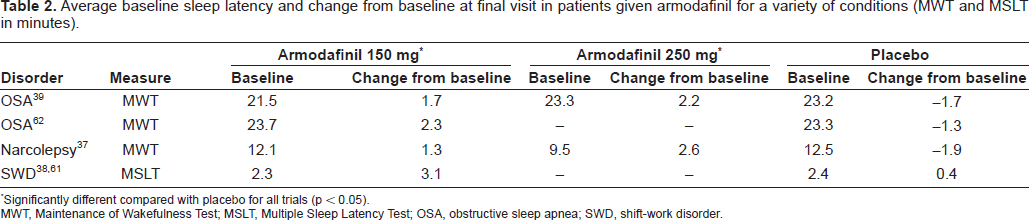
Significantly different compared with placebo for all trials (p < 0.05).
MWT, Maintenance of Wakefulness Test; MSLT, Multiple Sleep Latency Test; OSA, obstructive sleep apnea; SWD, shift-work disorder.
Clinical Global Impression of Change in patients given armodafinil for a variety of conditions (percentage of patients who improved at final visit).
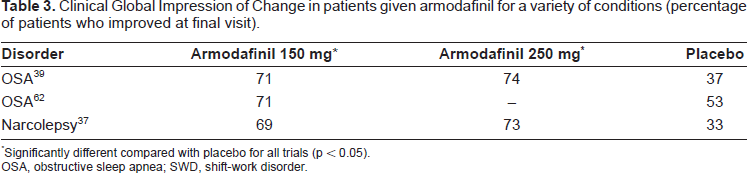
Significantly different compared with placebo for all trials (p < 0.05).
OSA, obstructive sleep apnea; SWD, shift-work disorder.
Healthy subjects
In a single-dose study of healthy males, subjects were required to stay awake between 0700 hours on Day 1 and 1100 hours on Day 2. 54 Armodafinil 100 mg, 150 mg, 200 mg, and 300 mg, or modafinil 200 mg were given to subjects at 1925 hours; subjects were then assessed using six 20-minute MWT assessments conducted every 2 hours between 2200 hours on Day 1 and 0800 hours on Day 2. Armodafinil and modafinil significantly improved wakefulness compared with placebo (mean wake time for the doses listed above was 16.1 minutes, 16.8 minutes, 18.5 minutes, 18.5 minutes, and 16.4 minutes, respectively, versus 10.5 minutes for placebo; p < 0.0001). 54 Armodafinil and modafinil also significantly improved sustained attention performance (measured using the Psychomotor Vigilance Test) compared with placebo in healthy subjects, with fewer lapses of attention and shorter median reaction times during the period of enforced sleep loss (p < 0.0001 for both drugs).
Although armodafinil and modafinil required 5-6 hours and 2 hours, respectively, to reach tmax, both agents demonstrated significant wakefulness-promoting effects compared with placebo at the earliest recorded timepoint (2200 hours, i.e, approximately 2.5 hours after drug administration). However, when the effects of armodafinil 200 mg and modafinil 200 mg were compared, MWT sleep latencies were numerically longer and lapses in attention were numerically fewer for subjects receiving armodafinil. The differences between the compounds were evident from 6 hours after administration, with the greater effects of armodafinil lasting for up to 13.5 hours. On Day 2 of the study (during recovery sleep following sleep loss), decreases in sleep efficiency were observed in subjects who had received the higher doses of armodafinil (p < 0.01 versus pretreatment values). 54
Narcolepsy
Hypocretins are neuropeptides that are thought to prevent inappropriate fluctuations between states of consciousness. Abnormalities in the hypocretin system–-particularly loss of the neurons that produce hypocretins in the hypothalamus–-are a defining feature of narcolepsy with cataplexy (sudden loss of muscle tone).64,65 Narcolepsy is universally characterized by ES; however, cataplexy is found in only 60%-70% of patients with narcolepsy.66,67 The prevalence of narcolepsy with cataplexy is estimated to be 0.02%-0.05%, while the incidence of this disorder is thought to be 0.74 per 100 000 person-years. 68
There is currently no cure for narcolepsy, instead treatment focuses on addressing the symptoms of ES and cataplexy. A 12-week, randomized, doubleblind, placebo-controlled trial of armodafinil 150 mg or 250 mg once daily in the treatment of ES associated with narcolepsy was conducted in 47 centers located across the USA, Canada, France, Australia, Germany, and Russia. 37 Patients with or without cataplexy were permitted to enroll in the study provided that they were on a stable dose of anticataplectic medicine and were not taking sodium oxybate; patients were excluded if they were receiving melatonin or sedatives such as barbiturates, benzodiazepines, and zolpidem. Patients were randomized to receive armodafinil 150 mg (n = 64), 250 mg (n = 67), or placebo (n = 63). The primary endpoint of this study was change in mean sleep latency, assessed using the MWT between 0900 and 1500 hours, and the proportion of patients demonstrating improvements on the Clinical Global Impression of Change scale (CGI-C). Study medication was taken by patients approximately 30 minutes before breakfast. Laboratory assessment of each patient was carried out at baseline and at Weeks 4, 8, and 12.
At the final visit (Week 12 of the study or the last scheduled clinic visit before discontinuation) treatment differences in sleep latency between 0900 and 1500 hours relative to placebo were 3.2, 4.5, and 3.8 minutes for the 150 mg and 250 mg groups and for both treatment groups combined, respectively (p < 0.001 for all comparisons). Sleep latency relative to placebo was also improved when measured later in the day. Between 1500 and 1900 hours, treatment differences relative to placebo were 2.7, 2.8, and 2.8 minutes in the 150 mg, 250 mg, and armodafinil combined groups, respectively (p < 0.05 for the combined group and the 150 mg group versus placebo). At the final visit, the proportion of patients who were judged by the study investigators to have experienced at least minimal improvement in their CGI-C ratings was significantly higher in all active-treatment groups compared with placebo (p < 0.001). In patients receiving armodafinil, attention (p < 0.05 for the 150 mg group and the combined group) and episodic secondary memory (p < 0.05 for all groups) were also significantly improved at the final visit compared with those receiving placebo. Night-time sleep was not affected in patients administered armodafinil. 37
Obstructive sleep apnea
OSA is a sleep disorder characterized by episodes of partial or complete collapse of the airway and is associated with increased morbidity and mortality. 69 The most common symptom of OSA is ES. Approximately 2% and 4% of men and women, respectively, in the USA have OSA with ES. 70 Current evidence indicates that up to 93% of women and 82% of men with moderate to severe OSA remain undiagnosed. 71 OSA is most commonly treated using a continuous positive airway pressure (CPAP) device, which maintains an open airway during sleep. Dental devices and surgery are also indicated for the treatment of patients with OSA. 72 ES persists in 22% and 52% of patients with OSA assessed using the ESS or MSLT, respectively, even after treatment with CPAP. 73
Armodafinil 150 mg or 250 mg once daily is indicated as an adjunctive pharmacotherapy to CPAP or other forms of treatment for OSA in order to reduce ES, although it is important that patients are counseled to remain compliant with their primary treatment modality. Roth and colleagues 39 have studied the efficacy of armodafinil for ES associated with OSA in a 12-week, double-blind, randomized, placebo-controlled trial conducted in 37 centers across the USA and Canada. Patients aged 18-65 years with moderate OSA and residual ES despite ≥4 weeks of adequate CPAP treatment were randomized to take armodafinil 150 mg (n = 133), 250 mg (n = 131), or placebo (n = 131) once daily before 0800 hours, approximately 30 minutes before breakfast. The primary endpoints of this study were the change from baseline to Week 12 (or discontinuation) in mean sleep latency across the first four 30-minute MWT assessments performed each day (at 0900, 1100, 1300, and 1500 hours) and the rate of at least minimal improvement in the CGI-C. At the final visit, patients administered armodafinil (150 mg, 250 mg, and both treatment groups combined) demonstrated significant increases from baseline in sleep latency across the first four MWT assessments performed each day compared with the placebo group (p < 0.001). Significant changes were seen as early as Week 4, when patients in the armodafinil 150 mg and the combined groups experienced statistically significant mean changes from baseline in sleep latency across the last three MWT assessments of each day (at 1500, 1700, and 1900 hours) compared with placebo (p = 0.01 and p < 0.01, respectively). MWT results are shown in Figures 2A and 2B. At all timepoints, the proportion of patients with at least minimal improvement on the CGI-C was significantly greater in the armodafinil-treated group than in the placebo group (p < 0.001) (Figure 3). 39
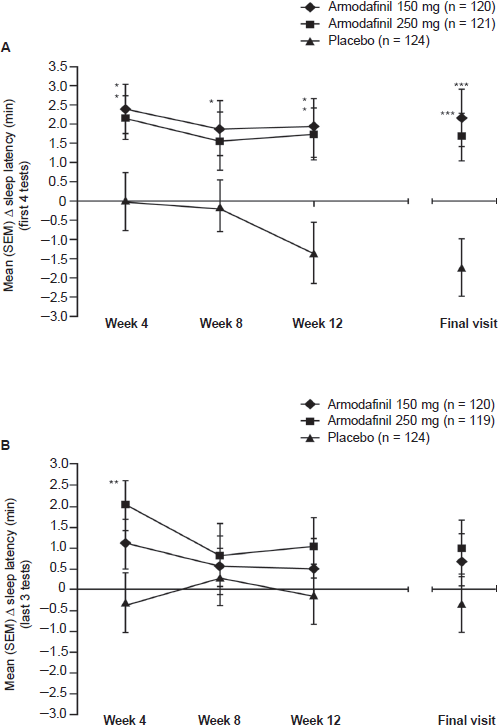
Sleep latency as assessed using the Maintenance of Wakefulness Test. (A) Mean change from baseline in sleep latency averaged across the first four tests (0900, 1100, 1300, and 1500). (B) Mean change from baseline in sleep latency averaged across the last three tests (1500, 1700, and 1900). SEM, standard error of the mean. *p < 0.05 versus placebo; **p = 0.01 versus placebo; ***p < 0.001 versus placebo. Reprinted from Clinical Therapeutics, Vol 28, Roth et al. Effects of armodafinil in the treatment of residual excessive sleepiness associated with obstructive sleep apnea/hypopnea syndrome, Page No. 689-706, Copyright (2006), with permission from Elsevier. 39
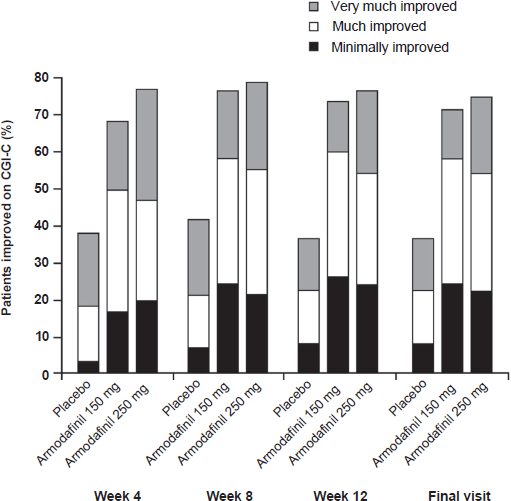
Proportions of patients who were rated as clinically improved on the Clinical Global Impression of Change (CGI-C). p < 0.001 versus placebo for all comparisons of proportions of patients who were at least minimally improved. Reprinted from Clinical Therapeutics, Vol 28, Roth et al. Effects of armodafinil in the treatment of residual excessive sleepiness associated with obstructive sleep apnea/hypopnea syndrome, Page No. 689-706, Copyright (2006), with permission from Elsevier. 39
Hirshkowitz and colleagues 62 also performed a 12-week, randomized, double-blind, placebo-controlled, parallel-group study of patients with at least moderate OSA and residual ES despite adequate CPAP treatment. This study took place in 36 centers across the USA, Australia, Russia, Germany, and France and randomized 131 patients to the armodafinil 150 mg arm and 132 patients to the placebo arm. The primary endpoints of this study were improvements from baseline in sleep latency at the first four MWT tests (0900, 1100, 1300, and 1500 hours) and improvements in clinical condition assessed using the CGI-C. Armodafinil significantly improved wakefulness compared with placebo at all assessment visits. At the final visit, sleep latency across the first four MWT assessments performed was significantly higher in the armodafinil group compared with placebo (+2.3 minutes versus placebo -1.3 minutes; p = 0.0003). At the final visit, sleep latency in the last three MWT assessments (performed at 1500, 1700, and 1900 hours) was also significantly increased in the armodafinil-treated patients compared with placebo (+1.8 minutes versus -0.5 minutes, respectively; p = 0.0435). At the final visit, the proportion of patients with at least minimal improvement in their clinical condition was significantly higher in the armodafinil group compared with the placebo group (71% versus 53%; p = 0.0069). In addition, episodic secondary memory was significantly improved at the final visit in patients taking armodafinil (p = 0.0102 versus placebo). 62
Pooled analyses of the results of these two studies 63 demonstrated that at the final visit, sleep latency was increased by 2.0 minutes with armodafinil versus a decrease of 1.5 minutes for placebo (p < 0.0001). Furthermore, patients treated with armodafinil had improved wakefulness later in the day (at the last three MWT assessments at 1500, 1700, and 1900 hours) compared with placebo (+1.1 minutes versus -0.3 minutes, respectively; p < 0.05). The quality of secondary episodic memory was also significantly improved with armodafinil (p < 0.05 versus placebo). Armodafinil treatment did not adversely affect night-time sleep in either of the 12-week studies as assessed by polysomnography. Although CPAP use did decline during the study (-0.3 hours versus -0.1 hours for armodafinil and placebo, respectively; p < 0.0001), this was not accompanied by an increase in the number of apneas or hypopneas (breathing interruptions) experienced by the study participants. 63
Shift-work disorder
The circadian rhythm disorder SWD is caused by enforcing an artificial pattern of sleep and wake that is misaligned with the body's internal circadian rhythm; the most obvious example of this is the nightshift, which requires workers to stay awake at night and sleep during the day. Not all shift workers develop SWD; those who do experience insomnia when attempting to sleep and ES during work hours. 74 Currently, the true prevalence of SWD is yet to be elucidated. The chronic strain of shift work in addition to sleep debt and circadian misalignment is thought to be responsible for the increased risk of cardiovascular disease seen in patients with SWD and their increased risk of peptic ulcers and mood disorders, such as irritability and depression.74,75 Furthermore, patients with SWD are more likely to miss work and social activities than symptom-free daytime workers. 75
To date, the single study of armodafinil in this indication has been reported in two abstracts. The study assessed armodafinil 150 mg in the treatment of ES associated with SWD in a 12-week, doubleblind, placebo-controlled, randomized study of 216 permanent- or rotating-shift workers.38,61 Study participants took armodafinil or placebo only on the nights when they worked a night shift or when they were assessed in a simulated night shift in the laboratory (at Weeks 4, 8, and 12). The primary endpoints of this study were sleep latency and clinical condition assessed using the MSLT and Clinical Global Impression of Improvement (CGI-I), respectively. At the final visit, patients administered armodafinil experienced significant increases in sleep latency compared with the placebo group (3.1 minutes versus 0.4 minutes, respectively; p < 0.0001). Furthermore, CGI-I ratings were improved in a significantly greater proportion of patients in the armodafinil group than in the placebo group (75% versus 59%, respectively; p = 0.001). Armodafinil also significantly improved attention and episodic secondary memory relative to placebo (p < 0.05) and patients taking armodafinil in this trial reported that the study medication did not affect their ability to sleep during the daytime.38,61
Summary of efficacy data
In a preclinical study in rats, armodafinil had equivalent wakefulness-promoting effects to D-amphetamine, without leading to symptoms characteristic of sleep deprivation. 60 Both modafinil and armodafinil have been reported to demonstrate significant wakefulness-promoting effects compared with placebo in sleep-deprived healthy subjects; however, armodafinil also demonstrated numerically longer increases in sleep latency and numerically fewer lapses in attention compared with modafinil in this study. The effects of armodafinil lasted for up to 13.5 hours in healthy subjects. 54
Armodafinil significantly increased sleep latency compared with placebo in patients with narcolepsy, SWD, and treatment-resistant ES associated with OSA and also significantly improved patients’ clinical condition, as assessed using the CGI-C or CGI-I. In addition, armodafinil increased attention and secondary episodic memory compared with placebo in patients with narcolepsy or SWD and improved secondary episodic memory in patients with ES associated with OSA.37–39,61–63
Safety and Tolerability
Armodafinil is generally well tolerated, with headache being the most common adverse event associated with use of this medication. In a single-dose pharmacokinetics study in healthy subjects, abdominal pain and nausea were reported in 13% of subjects administered armodafinil and the incidences of headache and nausea increased in the higher dose (200 mg and 300 mg) groups. 54 Pooled safety data from 14-day pharmacokinetics studies of armodafinil indicated that armodafinil 400 mg daily appeared to be an intolerable dose and therefore this regimen was discontinued after 7 days.
Headache, nausea, dizziness, and decreased appetite were the most commonly reported adverse events in a 12-week randomized trial of armodafinil in patients with narcolepsy. 37 These events were usually mild to moderate in severity and occurred with greatest frequency during the first 2 weeks of the study. In the study of patients with narcolepsy, one serious adverse event of severe acute urticaria and angioedema was reported in the armodafinil 150 mg group; however, owing to the patient's history, this event was judged by the study investigator to be unlikely to be related to treatment with armodafinil. In addition, analysis of armodafinil combined data showed a small but statistically significant increase in blood pressure relative to placebo (0.4 mmHg versus -2.6 mmHg, respectively; p = 0.0294). 37 Headache, nausea, nasopharyngitis, and anxiety were the most common adverse events in a 12-week study of armodafinil in patients with SWD. 38
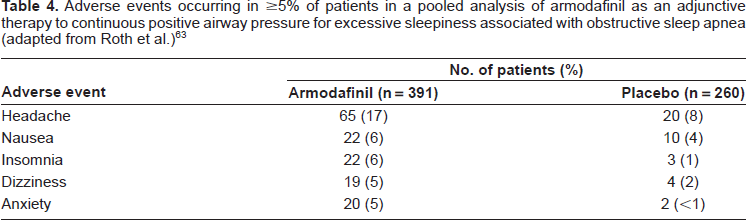
In a 12-week study of armodafinil in patients with ES despite CPAP treatment for OSA, the most frequent adverse event was headache, which was reported in 17.6% (46/262) of patients versus 8.5% (11/130) of patients who received placebo. 39 Most adverse events were of mild to moderate severity. Liver function tests showed that mean changes from baseline in γ-glutamyl transpeptidase and alkaline phosphatase concentrations were statistically significantly higher in armodafinil-treated patients versus placebo (p < 0.01 and p < 0.001, respectively) but these changes were not considered to be clinically meaningful. When compared with placebo, armodafinil-treated patients experienced small increases from baseline in morning diastolic blood pressure (armodafinil +0.6 mmHg versus placebo -1.4 mmHg; p < 0.05) and evening heart rate (armodafinil +1.2 bpm versus placebo -1.2 bpm; p < 0.05). A study by Hirshkowitz and co-workers 62 in the same indication (residual ES associated with OSA) again reported that headache was the most common adverse event associated with armodafinil treatment, followed by nausea, diarrhea, dizziness, and anxiety (≥5% of patients). Adverse events were generally mild to moderate in severity and no clinically meaningful changes in laboratory measures, vital signs, or results of physical examinations were reported. 62 The safety and tolerability data reported in a pooled analysis 63 of the studies by Hirshkowitz and colleagues 62 and Roth and colleagues 39 are shown in Table 4. These data indicate that, in addition to the aforementioned headache, nausea, dizziness, and anxiety, insomnia is experienced by ≥5% of patients receiving armodafinil (6% versus 1% for patients given placebo). As reported in clinical trials of modafinil, insomnia may indicate that the medication was taken too close to bedtime, or in too high a dose. In the event that a patient experiences insomnia with armodafinil, dose reduction is recommended. 33
Adverse events occurring in ≥5% of patients in a pooled analysis of armodafinil as an adjunctive therapy to continuous positive airway pressure for excessive sleepiness associated with obstructive sleep apnea (adapted from Roth et al.)63
Armodafinil is contraindicated in patients with known hypersensitivity to modafinil and armodafinil or its inactive ingredients. Serious rash, including Stevens–Johnson syndrome, has been reported in patients receiving modafinil. While no serious skin rashes have been reported in clinical trials of armodafinil, a similar risk of serious rash with armodafinil cannot be ruled out.
Controlled trial data for armodafinil have shown that psychiatric events, such as anxiety, agitation, nervousness, and irritability, led to treatment discontinuation more frequently than in patients given placebo (1.2% versus 0.3%, respectively). 33 In addition, a number of psychiatric adverse events, including mania, delusions, and hallucinations, have been reported for modafinil in postmarketing surveillance data. The possibility that the same psychiatric events may occur cannot be ruled out for armodafinil.
Abuse potential with modafinil is low and thus may also be low with armodafinil. 76 Conversely, other treatments for ES, such as amphetamines or sodium oxybate, have a high abuse potential or a high likelihood of misuse. 77 For these reasons, armodafinil is a Schedule IV medication while amphetamines and sodium oxybate are Schedule II and III medications, respectively.
Summary of safety and tolerability
Armodafinil was generally well tolerated in clinical trials; headache, nausea, dizziness, decreased appetite, anxiety, and insomnia of mild to moderate severity were the most commonly reported adverse events.33,63 Statistically significant changes in blood pressure and liver function tests have been observed in armodafinil-treated patients, but were judged not to be clinically meaningful. 33
Although serious rash and psychiatric adverse events have not been reported for patients given armodafinil, these events have been observed in modafinil-treated patients; therefore, use of armodafinil is contraindicated in patients who are likely to be susceptible to such events. 33 Abuse potential with armodafinil is likely to be of a similar low level to that of modafinil and both agents are therefore Schedule IV medications. 33
Patient-Focused Perspectives
Patient-reported outcomes
Patient-reported outcomes have been assessed in studies of armodafinil for ES associated with narcolepsy, OSA, and SWD in the form of diary data and subjective measures of sleepiness, such as the ESS and KSS.
Patients administered armodafinil in a trial assessing the efficacy of this wakefulness-promoting agent in the treatment of ES associated with narcolepsy were given electronic diaries and were also questioned using the ESS. 37 Patients administered armodafinil 150 mg or 250 mg recorded that they experienced 33% and 44% reductions in the number of unintended daily sleep episodes, respectively; patients given placebo experienced a 10% reduction in such sleep episodes (p < 0.0001). In addition, daily naps were reduced by 41%, 44%, and 22% for patients who received armodafinil 150 mg, 250 mg, or placebo, respectively (p = 0.0039 for overall treatment effect). Moreover, at the final visit, 21% and 28% of patients in the armodafinil 150 mg and 250 mg groups had an ESS score < 10 (indicative of normal alertness) compared with 7% of patients in the placebo group (p = 0.0312 and p = 0.0023, respectively). Global fatigue–-assessed using the Brief Fatigue Inventory–-was also significantly improved in all treatment groups versus placebo at the final visit (p < 0.01 for all groups).
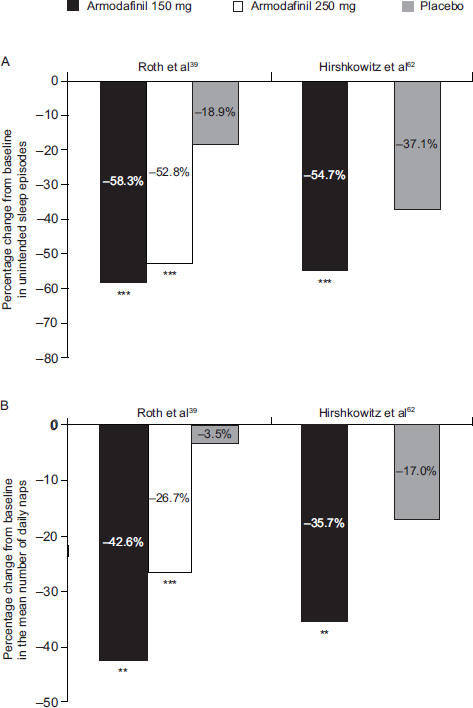
Diary data, ESS scores, and Brief Fatigue Inventory scores from patients enrolled in the two 12-week studies of armodafinil for residual ES associated with OSA reported that armodafinil reduced both fatigue and ES.39,62,63 The occurrence of unintended sleep episodes and daily naps was significantly reduced in the armodafinil-treated patients versus placebo39,62 (Figures 4A and 4B) and reductions in subjective ES were significantly greater in the armodafinil groups at all visits (Weeks 4, 8, and 12) compared with placebo (p < 0.01).39,62 Furthermore, at the final visit, armodafinil significantly reduced global fatigue and worst fatigue in the last 24 hours compared with placebo (p < 0.05).39,63 Average fatigue scores were significantly reduced following treatment with armodafinil 150 mg or 250 mg compared with placebo (p < 0.01). 63
Electronic diaries and the KSS were used in a trial of armodafinil in the treatment of ES associated with SWD, 38 in which the wakefulness-promoting agent significantly reduced the maximum level of ES experienced during night-shift work compared with placebo (1.1 versus 2.0 points, respectively; p < 0.0001). Compared with placebo, armodafinil also significantly attenuated ES during the commute home (1.2 for placebo versus 0.6 points for armodafinil; p = 0.0027). Subjective ES measured using the KSS was reduced with armodafinil relative to placebo (p < 0.005). 38
Quality of life
Data concerning the effects of armodafinil on patient quality of life are sparse and further studies are warranted. Based on available studies, quality of life would be improved by the reported reductions in fatigue and increases in episodic secondary memory in the trials of armodafinil in patients with residual ES associated with OSA.39,62,63
Rates of discontinuation in armodafinil studies
In the study by Roth and colleagues 39 of armodafinil in patients with residual ES associated with OSA despite adherence to CPAP treatment, 15% (40/264) of patients randomized to armodafinil discontinued treatment compared with 8% (11/131) of patients administered placebo. The difference in the rates of discontinuation between the two study groups did not reach statistical significance. A study of armodafinil in the same indication reported similar results with 15% (20/131) of patients in the active-treatment group discontinuing treatment compared with 11% (14/132) of patients given placebo. 62 Noncompliance was the reason for discontinuation in 3 patients who received armodafinil. 62 Overall, 7.5% (10/133) and 11.5% (15/131) of patients who received armodafinil 150 mg and 250 mg, respectively, discontinued treatment due to adverse events versus 3.8% (5/131) of patients given placebo in a study of patients with SWD. 38 In a study of armodafinil in patients with narcolepsy, 25% and 16% of patients randomized to receive armodafinil 150 mg or 250 mg, respectively, withdrew from the study compared with 14% of patients in the placebo group. Adverse events and withdrawal of consent were the most common reasons for discontinuation in this study. 37
Adherence and uptake
The benefits of modafinil do not always persist beyond a few hours, meaning that some patients may require dose escalation or split dosing. The wakefulness-promoting effects of armodafinil last longer than those of modafinil (as indicated by its longer tmax and presence at higher concentrations later in the day), which may facilitate once-daily dosing in patients receiving armodafinil, a feature that is convenient for patients and which may aid with compliance. 54 As shown in the “Rates of discontinuation in armodafinil studies” section, discontinuation rates in clinical trials of armodafinil have been low; however, until armodafinil becomes commercially available and postmarketing surveillance data can be gathered, any benefits of armodafinil in terms of patient compliance remain theoretical.
Summary of patient-focused perspectives
Armodafinil demonstrated significant reductions in subjectively measured ES in clinical trials of patients with ES associated with narcolepsy, SWD, or OSA.37–39,62,63 In addition, patients with ES associated with narcolepsy or OSA treated with armodafinil experienced significant reductions in the number of unintended daily sleep episodes and daily naps compared with patients given placebo.37,39,62,63 Fatigue scores were also significantly reduced by armodafinil in patients with ES associated with OSA.39,63 ES experienced during night-shift work and the consequent commute home was also significantly reduced in patients with SWD given armodafinil versus those given placebo. 38
These improvements in patient-reported outcomes alongside the increased attention and secondary episodic memory conferred by armodafinil37,38,62,63 are expected to improve patients’ quality of life; however, data in this respect are sparse and further studies are required. Discontinuation rates were comparable for patients given armodafinil or placebo in randomized clinical trials. Moreover, the prolonged wakefulness-promoting effects of armodafinil late in the day and once-daily dosing may improve convenience and increase patient compliance.
Conclusion and Place in Therapy
Armodafinil has demonstrated its efficacy as a wakefulness-promoting agent by increasing sleep latency and improving clinical condition in patients with ES associated with narcolepsy, SWD, and OSA. Furthermore, the effects of armodafinil may persist longer than those of modafinil, which could help patients stave off ES for longer. The possibility of once-daily dosing with armodafinil may also aid in patient compliance (although modafinil can also be given once daily in most patients). Armodafinil also improves attention and episodic secondary memory in patients with ES associated with OSA and reduces fatigue across the spectrum of patients assessed and is consequently likely to improve their activities of daily living and quality of life. Armodafinil was also well tolerated in these trials and most adverse events were mild to moderate in severity.
All of the trials conducted with armodafinil to date have been of 12 weeks’ duration and longer studies would assist in characterizing the long-term efficacy of armodafinil in patients with ES due to a variety of conditions. The results of the ongoing open-label trials are eagerly awaited for this reason. Furthermore, evaluations of armodafinil are planned for other indications, including bipolar depression, cognition deficits associated with schizophrenia, ES in Parkinson's disease, and fatigue in patients treated for cancer. 59
The author has observed that modafinil is an effective countermeasure to ES in his own traumatic brain injury population and armodafinil may also be of use in this indication. 78 In addition, armodafinil has been shown to attenuate sleep deprivation in healthy subjects 54 and may therefore be of assistance to healthy individuals in extreme circumstances, for example in military applications where a high level of vigilance is required for extended periods. Modafinil is approved by the U.S. Air Force for use by pilots during flights of long duration 79 and repeated doses of modafinil given prophylactically have been shown to improve alertness and performance in a simulator test of sleep-deprived army helicopter pilots. 80
Using quantitative electroencephalography, one may measure brainwave frequencies, amplitudes, and densities. Delta brainwave activity (1-3 Hz) is a representative sleep characteristic, while alpha brainwave activity (8-12 Hz) in the posterior brain regions is a representative awake characteristic. Delta brainwave activity is increased and alpha brainwave activity is reduced in sleep-deprived individuals, 81 and repeated doses of modafinil 100 mg have been shown to postpone the onset of these brainwave patterns for up to 42 hours and 46 hours, respectively, in healthy military aviators. 81 Train and truck drivers are also often required to work long and/or consecutive shifts carrying out tasks that may be repetitive or monotonous.82–84 Armodafinil may therefore be useful in promoting wakefulness in commercial/military aviators and drivers who are required to remain awake for long periods of time and further investigation into such matters is warranted.
In summary, armodafinil is the potent R-isomer of modafinil, with a longer duration of effectiveness than the racemic compound but with a similar tolerability and safety profile. It is currently approved as a wakefulness-promoting agent in patients with ES associated with OSA, narcolepsy, and SWD and has been shown to improve patient-reported outcomes in individuals with these conditions. Future potential applications may include ES associated with traumatic brain injury, chronic fatigue syndromes, hypersomnias, and other circadian rhythm disorders. Armodafinil is likely to further reduce the disability associated with ES and improve quality of life beyond the level of improvement conferred by modafinil in patients who are chronically drowsy.
Disclosures
The views expressed in this manuscript are those of the author and do not reflect the official policy or position of the Department of the Army, Department of Defense, or the U.S. Government.
The author would like to thank Jane Bryant of Anthemis Consulting Ltd for her editorial support, the Henry M. Jackson Foundation for their administrative support, and Cephalon Inc. for their financial support to the Henry M. Jackson Foundation. Colonel Russo was not compensated and retained full editorial control over the content of the paper.