
Abstract
Hypertension is the leading cause of disability and cardiovascular mortality world-wide. Approximately one-third of the US adult population and over a billion people world-wide have hypertension. Despite increased awareness of hypertension and availability of many effective antihypertensive agents, only one third of patients achieve their target blood pressure (BP). All expert panels now recommend use of combination therapy for stage 2 and higher hypertension and for individuals who are at increased risk of cardiovascular disease (CVD). Amlodipine, a dihydropyridine calcium channel blocker and Valsartan, an angiotensin II receptor (AT1-R) antagonist are widely used antihypertensive agents. Their efficacy in lowering systolic and diastolic BP and reducing CVD events has been demonstrated in several randomized trials. Fixed-dose combination of amlodipine and valsartan (A/V) has been shown to be more effective in lowering BP than monotherapy with either of these agents alone in randomized trials with comparable side effect profile. Approximately 80%-90% of patients with stage 1-2 hypertension receiving A/V fixed-dose combination achieve significant response, defined as a mean sitting diastolic BP < 90 mmHg or > 10 mmHg reduction from the baseline. Subgroup analyses show that A/V fixed-dose combination is equally effective in older individuals (>65), Blacks, in patients with isolated systolic hypertension, and in those who fail monotherapy. Furthermore, A/V fixed-dose combination is well tolerated and simplifies antihypertensive regimen enhancing patient adherence and a better BP control compared to monotherapy.
Introduction
Hypertension is a major health problem world-wide and exceeds smoking as a causal factor in attributable mortality, accounting for 12.8% of all deaths. In 2000, approximately 1 billion people world-wide had hypertension and this number is expected to increase by 60% to a total of 1.56 billion by 2025. 1 Hypertension is a continuous variable and increases the mortality from ischemic heart disease and stroke in a log linear fashion between 40 to 89 years of age. 2 In the US 32% of all adults and 66% of those above the age of 60 have hypertension which accounts for 27.1% of the incident cases of End Stage Renal Disease (ESRD). 3 The highest prevalence rates are found among Black patients. 4 Effective, long-term control of BP to less than 140/90 mmHg reduces the incidence of heart failure by 50%, myocardial infarction by 25% and stroke by 40%. 5 Patients with chronic kidney disease (CKD) and those with diabetes benefit from further BP reduction to < 130/80 mmHg. 6 Despite the strong evidence and the availability of several effective antihypertensive agents, only 36.8% of all hypertensive patients achieve the rather conservative target BP of < 140/90 mmHg and only 37.5% of hypertensive diabetic patients achieve target BP of < 130/80 mmHg. Among patieints with CKD (defined as the presence of albuminuria or eGFR < 60 ml/min/1.73 m2) only 37% achieve the recommended target BP of ≤ 130/80 mmHg. 7
Compliance to prescribed antihypertensive regimen is essential to achieve the target BP. 8 Among many factors, the complexity and tolerability of the anti-hypertensive regimen are two major determinants of patient compliance. 9 Multiple antihypertensive agents needed to achieve the target BP control in majority of the patients add to the complexity of such therapy. Fixed-dose combinations of anti-hypertensive agents effectively lower BP and help simplify the therapeutic regimen and increase compliance. Several fixed-dose combinations of antihypertensive agents with different and often complementary mechanisms of actions are available in the market. The blockers of AT1-R and calcium channels are highly effective and commonly used BP lowering agents. A fixed-dose combination of an AT1-R, valsartan and a non-dihydropyridine CCB, amlodipine marketed as Exforge® is the focus of this review. A discussion of the general advantages of the fixed-dose combinations is followed by a discussion specific to Exforge®.
Advantages of Fixed-dose Combinations
Better BP control
In the US, the control of BP to < 140/90 mmHg increased from 29% in 1999 to 37% in 2003. 10 However, it remains unacceptably low given the evidence that achieving optimal BP control is the single most important intervention in the management of hypertension. Furthermore the target achieved (140/90 mmHg) is rather conservative especially for patients with diabetes and proteinuric CKD. Combining antihypertensive agents with complementary mechanisms of action is more effective in lowering BP and may counteract some of the adverse effects seen with the individual drugs (Table 1). Furthermore, combination therapy can achieve a better BP control without having to maximize the dose of a single agent thus reducing the dose-dependent side effects.
Benefits of combination therapy in hypertension.
Several large randomized trials have shown that monotherapy is ineffective in reducing BP to predetermined target range. For instance, in the Antihypertensive and Lipid Lowering Treatment to Prevent Heart Attack (ALLHAT) trial only 27% of 42,418 participants achieved the goal BP (< 140/90 mmHg) on monotherapy from a baseline mean systolic BP of 146 mmHg and 156 mmHg for previously treated and untreated patients, respectively. 11 In the Losartan Intervention For Endpoint (LIFE) trial, 90% of the 9193 participants with hypertension and left ventricular hypertrophy required more than one antihypertensive agent to achieve similar BP target (< 140/90 mmHg) from a mean baseline of 174/97.8 mmHg. 12 In the Avoiding Cardiovascular events through Combination therapy in Patients Living with Systolic Hypertension (ACCOMPLISH) trial 32.3% participants treated with benazepril/amlodipine or benazepril/HCTZ required additional antihypertensive agents to reach the target BP of < 140/90 mmHg (< 130/80 mmHg for patients with CKD) from a baseline of 145/80 mmHg. 13 In this randomized double-blind trial, the target BP (< 140/90 mmHg) was achieved in over 78% of the patients in the US cohort on amlodipine/benazepril combination. In diabetics and in patients with CKD the control rates were 72.5% and 70.8%, respectively. These results demonstrate that monotherapy is ineffective in achieving the target BP in majority of the hypertensive individuals. This is reflected in the recommendations by several advisory panels (Table 2). The JNC-7 guidelines recommend initiating therapy with two antihypertensive agents in patients with stage 2 hypertension, defined as systolic BP (SBP) 160 mmHg or above, a diastolic BP (DBP) 100 mmHg or above, or SBP/ DBP 20/10 mmHg above the goal. 6 The European Society of Hypertension also recommends initial combination antihypertensive therapy in patients at high cardiovascular risk. 14 Calcium channel blockers and the antagonists of the rennin-angiotensin system (RAAS) are being increasingly offered in fixed-dose combinations. In addition to lowering BP these drugs have vasculoprotective and pleiotropic properties.15,16
Guidelines for initial combination therapy.
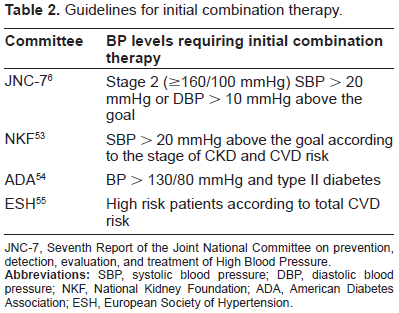
JNC-7, Seventh Report of the Joint National Committee on prevention, detection, evaluation, and treatment of High Blood Pressure.
Patient adherence
Patient adherence to prescribed therapy and advice is a strong predictor of achieving BP control. 8 The number of medications prescribed and the complexity of the treatment regimen are two important determinants of patient adherence. 17 This has been shown in patients with a variety of different diseases. Adherence improves with fewer medications or pills prescribed. Reducing the number of pills by using combination of drugs reduces non-adherence compared with the same drugs given separately even with the same frequency. 18 A meta-analysis of 9 studies comparing fixed-dose combinations versus the same drugs given separately for treatment of diabetes, hypertension, tuberculosis, and human immunodeficiency virus disease, showed that the fixed-dose combinations reduced the rate of non-adherence by 26%. 18 In this meta-analysis a subgroup analysis of the four studies in hypertension showed that the fixed-dose combinations decreased the risk of medication non-adherence by 24% compared with free-drug combinations. In a study of 198 hypertensive patients randomized to receive diltiazem twice-daily or amlodipine once daily, the patients on once-daily regimen took their study drug on a regular schedule 86% ± 2% of the times compared with 76% ± 2% for those who were on twice daily dosing schedule. 19 In a retrospective analysis of the data from a pharmacy claims database in the US, 20 adherence to a fixed-dose combination of amlodipine and benazepril was compared with the adherence to free-dose combination therapy of the two agents. Patients given two or more prescriptions for the fixed-dose combination (n = 2,839) or the two components separately (n = 3,367) were identified and followed up for an average of 259 days and 247 days, respectively. Adherence to the fixed-dose combination therapy (88%) was significantly greater compared to the free combination therapy (69%). The average annual cost of CVD-related care per subject was also significantly lower in patients receiving the fixed-dose combination. Other studies have shown that adherence to prescribed antihypertensive regimen is a direct determinant of the BP control achieved. 21
Fixed combination of Amlodipine and Valsartan
Next few paragraphs will present a brief overview of the pharmacology and efficacy of the individual drugs in this fixed-dose combination.
Amlodipine
Amlodipine is a third generation dihydropyridine CCB and is the most commonly used agent in its class. 22 More than 90% of amlodipine is absorbed and 95% of the circulating amlodipine is bound to plasma proteins. Due to lack of significant first pass hepatic metabolism, it has a prolonged duration of action. Like other CCBs, it acts by decreasing Ca++ entry to cells through the L-type Ca++ channels resulting in vascular smooth muscle relaxation. Its action peaks at 10-14 hours and steady state plasma levels reach in 7-8 days. Its half-life is 35-45 hours. About 90% of amlodipine is converted to inactive metabolites via hepatic metabolism, and 60% of the metabolites are excreted in the urine. In patients with kidney disease, the pharmacokinetics of amlodipine are minimally changed. The dose adjustment may be needed in hepatic disease. Aging slows the metabolism of amlodipine, likely due to a reduction in hepatic blood flow. 23 Reflex sympathetic activation is not seen with long term use of amlodipine. 24
In addition to being an effective antihypertensive agent amlodipine (with the possible exception of azelnidipine) also possesses antioxidant activity. Amlodipine is superior to felodipine, diltiazem, verapamil, and captopril at pharmacologically relevant doses in inhibiting lipid peroxidation in isolated membrane vesicles enriched with polyunsaturated fatty acids. 25 This antioxidant property of amlodipine is independent of calcium channel blockade and relates to its chemical structure and direct physio-chemical interactions with the membrane lipid bilayer. Due to high lipophilicity, amlodipine is highly concentrated in the cell membrane, which enables it to effectively scavenge free radicals and break the lipid peroxidation chain reaction. Two abstractable hydrogen atoms associated with its aromatic rings further enhance its antioxidant activity. 26 There is also evidence that amlodipine modulates the activity of PKC-α 27 which is a powerful activator of NADPH oxidase, the major superoxide anion generating system in the vasculature. Several animal and clinical studies have documented in-vivo antioxidant activity of amlodipine.28,29 In patients on maintenance hemodialysis, the reduction in oxidative stress is accompanied by a reduction in the plasma levels of asymmetric dimethylarginine (ADMA), an endogenous inhibitor of nitric oxide synthase. 28
Efficacy and Safety of Amlodipine
Amlodipine is very effective in lowering BP and reduces CVD morbidity and mortality. This was shown in the ALLHAT 30 which randomized 42,418 high risk patients to receive chlorthalidone, amlodipine, lisinopril, or doxazosin. The study participants were >55 years of age, had stage 1 or 2 hypertension with one additional CVD risk factor and 36% had diabetes. In this study, amlodipine was as effective as chlorthalidone in reducing the primary combined endpoint of fatal coronary heart disease or nonfatal myocardial infarction (RR, 0.98; 95% CI, 0.90-1.07). Its efficacy in reducing combined coronary heart disease events and ESRD was comparable to that of chlorthalidone. However, incidence of heart failure was 38% higher in patients assigned to amlodipine than those assigned to chlorthalidone in the absence of concomitant RAAS inhibitor therapy in either group. The incidence of other adverse effects was similar in both groups. This study is discussed in detail previously. In the Valsartan Antihypertensive Long-Term Use Evaluation (VALUE) trial, 31 amlodipine was more effective than valsartan in reducing the pre-specified secondary endpoint of fatal and nonfatal myocardial infarction (4.1% vs. 4.8%, p = 0.02). Overall there were no differences in the primary composite endpoint of the time to first cardiac event. In this study SBP control (< 140/90 mmHg) was achieved in 4392 (58%) of patients on valsartan and 4793 (64%) of those on amlodipine. The DBP (< 90 mmHg) control was achieved in 6652 (88%) and 6940 (92%) for valsartan and amlodipine, respectively. The target BP (both <140 mmHg systolic and <90 mmHg diastolic) was achieved in 4274 (56%) patients in the valsartan group and 4694 (62%) in the amlodipine group. The baseline BP in both groups was 154/88 mmHg. Both treatments were well tolerated. The incidence of edema was twice as high in amlodipinetreated patients (32.9%) as in valsartan-treated patients (14.9%), and hypokalaemia was seen in the 6.1% of the patients treated with amlodipine vs. 3.2% in the valsartan treated group. A later sub-study analysis of 7080 participants analyzed according to whether they were still on monotherapy at the end of the first six months showed that amlodipine increased the risk of CHF by 22%, 32 although the original analysis had shown no difference. Both of these large randomized trials suggested a higher risk of new onset CHF with amlodipine monotherapy. However, in patients with preexisting CHF, addition of amlodipine does not increase the mortality or morbidity. 33 Furthermore, the increased risk of CHF seen with amlodipine mono-therapy may be neutralized when it is combined with the inhibitors of RAAS. 34
Valsartan
Valsartan is a non-peptide, orally active and specific AT-R1 antagonist. The absolute average bioavailability of valsartan is 23%, although bioavailability as high as 51% has been reported. 35 Valsartan does not require metabolism to be active. Its antihypertensive effect is achieved within 2 h and the maximal reduction in BP is seen within 4-6 h. The antihypertensive effect lasts ≥24 h. There is similar tissue distribution among mammals, with the highest concentration in blood, kidneys, and liver. In total, 94%-97% of valsartan is bound to plasma proteins, mainly albumin. Plasma values decrease bio-exponentially, with a t½ of 7-8 h. It is eliminated mostly unchanged in bile (>80%) and urine (<20%). 36
Valsartan like other RAAS antagonists also exerts significant BP independent beneficial effects. It ameliorates oxidative stress by reducing the expression of NADPH-oxidase. 37 In patients on maintenance hemodialysis it reduces oxidative stress and plasma levels of ADMA similar to amlodipine. 28
Efficacy and Safety of Valsartan
Valsartan is an effective antihypertensive agent for all stages of hypertension and both in men and women. 38 An integrated analysis of efficacy data from nine double-blind, randomized, placebo-controlled, parallel studies of similar design and of at least 4 weeks’ duration confirmed the dose efficacy of valsartan as an antihypertensive agent. 39 This intent-to-treat analysis included 4067 patients with mild-to-moderate hypertension who had received valsartan (n = 2901) 10, 20, 40, 80, 160, or 320 mg once daily or placebo (n = 1166). Blood pressure was assessed at 24 hours after the last dose. In all nine studies, valsartan doses ≥80 mg produced statistically significant reductions in supine or seated diastolic blood pressure (SDBP) and systolic blood pressure (SSBP) compared with placebo (P < 0.05). There was an increase in valsartan's efficacy with increasing dose across the range 10 to 320 mg (placebo-subtracted mean changes from baseline to end point for valsartan 10, 20, 40, 80, 160, and 320 mg, respectively: SDBP, -0.8, -2.8, -2.6, -3.9, -5.1, and -6.4 mm Hg; SSBP, -1.3, -5.7, -5.3, -6.8, -8.6, and -9.0 mm Hg). The results of VALUE trial are discussed above. Efficacy of valsartan is also well established in the elderly and black patients. 40
Valsartan is taken once daily and is well tolerated with a placebo-like side-effect profile and its tolerability profile is similar to other ARBs. 41 The incidence of cough is lower with ARBs than ACEi, 3.2% versus 9.9%. 42 The incidence of angioedema also appears to be lower with the ARBs.
Dosage and Administration of the Fixed Dose Combination
The combination of amlodipine and valsartan is marketed by Novartis Pharmaceuticals as Exforge®. The different dose combinations available in the US are 5/160, 10/160, 5/320, and 10/320 mg of amlodipine and valsartan (A/V) whereas in the EU the available fixed-dose combinations are 5/80, 5/160, or 10/160 mg.
Although monotherapy can be directly switched to fixed-dose combination, it is recommended to titrate the individual components separately until a suitable dose of each drug is established before switching to the fixed-dose combination. 43
Caution should be exercised in prescribing fixed-dose combination to patients with hepatic dysfunction and biliary obstruction. The fixed-dose combination should be started at the lowest dose in elderly patients (>65) and in patients with chronic kidney disease. Serum potassium and creatinine should be monitored closely during the initiation or up-titration of the ACEi and ARBs containing fixed-dose combinations. 44
Peak plasma concentrations of amlodipine and valsartan are reached in 6-8 hours and 3 hours, respectively, following oral administration of the fixed-dose combination. 43 No specific data exists regarding the pharmacokinetics and drug interactions of the fixed-dose combination. The guidelines for the individual components should be followed.
Efficacy
The combination of amlodipine with valsartan is more effective in lowering BP than either of these agents used as monotherapy. This is due to interruption of different pressor pathways by these individual drugs. The studies on the efficacy of A/V fixed-dose combinations have used BP control or reduction as an endpoint and have not looked at any clinical endpoints. Two of these studies were published as a single report. 45 In these two placebo-controlled, double-blind studies, 2,478 hypertensive patients received either amlodipine 2.5 or 5 mg once-daily, valsartan 40, 80, 160 or 320 mg once-daily, the combination of amlodipine 2.5 or 5 mg with valsartan 40, 80, 160 or 320 mg once daily, or placebo for eight weeks. The main inclusion criterion for these studies was stage 1-2 essential hypertension with a mean SDBP ≥ 95 and ≤ 110 mmHg. There was a 2-week washout period followed by a 2-4 week single blind placebo run-in period followed by 8-week active treatment period in a double-blind fashion. The primary endpoint of these studies was change from the baseline in mean SDBP at the end of 8-week study period. An intent-to-treat analysis was employed. Response rate defined as the percentage of patients achieving a mean SDBP < 90 mmHg or ≥10 mmHg reduction from baseline constituted a secondary endpoint. Mean baseline sitting BP ranged from 152.8/99.3 and 156.7/99.1 mmHg in these two studies. Both amlodipine and valsartan were effective in lowering BP in a dose dependent manner. Reduction in the mean SDBP (14.2-15.9 mmHg) with fixed-dose A/V (5/80, 5/160, 5/320 mg daily) treatment for 8 weeks was significantly larger than the reduction seen with the same dose of amlodipine (11.5 mmHg) or valsartan (9.7-13.4 mmHg) monotherapy. Similarly the reduction in the mean SSBP was greater with the fixed-dose combination (19.5-22.7 mmHg) compared to monotherapy with amlodipine (12.4-15.1 mmHg) and valsartan (12.9-15.7 mmHg). This data is presented in Table 3. The response rates with the fixed-dose combination (81.1%-91.3%) were also significantly higher than those seen with amlodipine 5 mg (71.9%) or valsartan (57.7%-73.4%) monotherapy, although the response rates with the fixed-dose combination were not statistically different compared with amlodipine 10 mg monotherapy (86.6%) in the second study. The first study did not use this dose of amlodipine as monotherapy. Subgroup analyses of these studies confirmed similar efficacy across different levels of baseline BP, age, and race. Another double-blind study compared the efficacy of valsartan/amlodipine combination to an ACEi/diuretic combination in 130 patients with stage 2 hypertension. 46 The patients were randomized to receive for six weeks either a combination of amlodipine (5-10 mg) and valsartan (160 mg), or a combination of lisinopril (10-20 mg) and hydrochlorothiazide (12.5 mg). Both combinations were equally effective in lowering BP. The A/V fixed-dose combination reduced mean seated SBP (MSSBP) by 35.8 mmHg. Patients with MSSBP ≥ 180 mmHg at baseline had even a greater reduction (43.0 mmHg). At completion of the trial, 67.2% of patients had BP < 140/90 mmHg on A/V, versus 56.1% of the patients assigned to lisinopril/HCTZ.
Mean reduction in BP (systolic/diastolic, mmHg) with 8 weeks of once daily therapy with different doses of amlodipine and valsartan alone and in combination. 45
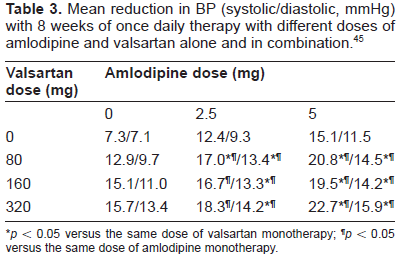
p < 0.05 versus the same dose of valsartan monotherapy;
p < 0.05 versus the same dose of amlodipine monotherapy.
Amlodipine and Valsartan Combination in Special Groups
Older patients
The prevalence of hypertension increases with age, affecting >63% of people aged 60-79 years and 74% of those over the age of 80 years. Treatment of hypertension in this age group is complicated by age-related differences in efficacy and tolerability. Kostis 47 analyzed the data for patients over the age of 65 from the two randomized trials of the fixed-dose A/V 45 discussed in the previous section. In these studies, 704 of 3155 (22.3%) patients were over the age of 65. Reduction in BP with A/V fixed-dose combination was similar among patients below and above the age of 65 years. Analysis of patients over the age of 65 from one of these studies (n = 358/1250) showed a decrease in blood pressure by 25.2/15.7 mmHg with the 10/160 mg dose and 27.9/18.2 mmHg with the 10/320 mg dose. The corresponding reduction in the MSSBP/MSDBP with amlodipine 10 mg, valsartan 160 mg, valsartan 320 mg, and placebo were 23.3/15.9, 18.7/15.6, 20.9/15.4, and 8.0/6.6 mmHg, respectively. Similar trends were observed in the second study (n = 347/1911) in patients ≥65 years of age. In another randomized double-blind study, 894 hypertensive patients (mean age 58.5 years, 30.6% patients ≥65 years of age) previously uncontrolled on monotherapy, were switched to either 5/160 or 10/160 mg dose of fixed-dose A/V combination. For patients with uncontrolled BP (defined as > 140/90 mmHg or > 130/80 mmHg for diabetics) on fixed-dose combination therapy for 8-12 weeks, open-label hydrochlorothiazide (HCTZ) 12.5 mg/d was added. If the BP in patients who required HCTZ at 8 weeks remained uncontrolled at 12 weeks, the dose of HCTZ was increased to 25 mg/d. The combination therapy significantly improved the BP control after 16 weeks in both the young (<65 years) and the older (>65 years) patients. The mean reduction from baseline in MSSBP and MSDBP at 16 weeks were similar in the younger (17.9/11.6 mmHg) and the older patients (20.6/12.6 mmHg) with 5/160 mg and (18.2/9.8 mmHg and 21.2/11.3 mmHg) with the 10/320 mg combination. At week 16, in the younger group the BP control rates were 73.4% and 78.6% with 5/160 and 10/320 mg, respectively. In the older group the BP control rates were 71.2% and 66.4%, for the same two doses of the fixed-dose combination. 48 In general the results were similar in diabetic and non-diabetic patients. The combination therapy was generally well tolerated with a lower overall incidence of adverse events among elderly patients (32.5%) versus younger patients (45.3%) in all treatment groups. However, the peripheral edema rates were higher in older patients (9.9% vs. 4.3%) in this study.
These findings demonstrate that the fixed-dose combination of A/V is effective in achieving predefined target BP control in patients ≥65 years of age, and is generally well tolerated.
Black Patients
Adult blacks have the highest age-adjusted rates of hypertension with prevalence of 39.1%. 49 Blacks also have an earlier onset of hypertension, higher levels of BP once hypertensive, greater end-organ damage, and excess morbid and fatal CVD events including stroke, coronary heart disease, heart failure and CKD from hypertension. 6 Furthermore, the prevalence of resistant and poorly controlled hypertension is high among Blacks due to concurrent obesity, diabetes, salt sensitivity, and impaired renal function. 50 Combination therapy in Blacks has been shown to be more effective in achieving target BP than monotherapy.
In a prospective, randomized, double-blind study 573 Black hypertensive patients with stage 2 hypertension (MSSBP) > or = 160 and <200 mmHg) were randomized to receive either A/V or amlodipine therapy for 12 weeks. 51 After 2 weeks, there was forced titration of A/V 5/160 mg to 10/160 mg and of amlodipine 5 to 10 mg followed by 10 additional weeks of treatment. If SBP was ≥ 130 mmHg at week 4, the fixed-dose combination was allowed to be increased to 10/320 mg. At week 8, HCTZ 12.5 mg was optionally added to both arms if SBP was still ≥ 130 mmHg. A/V at week 8 lowered MSSBP last observation carried forward significantly than amlodipine (33.3 vs. 26.6 mmHg, P < 0.0001). Lowering of MSSBP with A/V significantly exceeded that of amlodipine in several specified subgroups-the elderly (> or = 65 years), those with isolated systolic hypertension, and those with body mass index (BMI) > or = 30 kg/m2. More patients treated with A/V than amlodipine achieved BP control (< 140/90 mmHg) both at weeks 8 (49.8 vs. 30.2%; P < 0.0001) and 12 (57.2 vs. 35.9%; P < 0.0001). A post hoc analysis showed a 30% reduction in the spot urinary albumin to creatinine ratio (UACR) with the fixed-dose A/V combination whereas amlodipine monotherapy increased UACR by 10%. There were no significant differences in adverse events among the two treatment groups.
Tolerability
In the single report of the two randomized studies (discussed above), the most frequently reported adverse events (AE) with fixed-dose A/V were peripheral edema, headache, nasopharyngitis, upper respiratory infection, and dizziness. Patients receiving fixed-dose A/V combination had a significantly lower incidence of peripheral edema compared with therapy with amlodipine monotherapy (5.4% vs. 8.7%; p < 0.05), although it was still higher than the incidence observed with valsartan monotherapy (2.1%; p < 0.001), Table 4. The overall incidence of AE with the fixed-dose A/V combination was similar to that of amlodipine (44.1% vs. 45.7%), but significantly higher than that of valsartan (39.8%). The incidence of therapy withdrawal was 1.8% and was not different among the patients treated with the fixed-dose A/V combination and those treated with placebo. Another study compared ankle edema in 80 patients on A/V (10/160 mg daily) vs. amlodipine monotherapy over a six-week period. 52
Adverse events with amlodipine, valsartan, fixed-dose A/V combination and placebo.
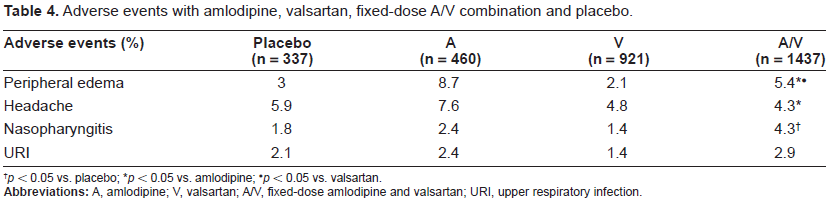
p < 0.05 vs. placebo;
p < 0.05 vs. amlodipine;
p < 0.05 vs. valsartan.
Treatment with the fixed-dose combination led to lesser gain in the ankle foot volume compared with the treatment with amlodipine monotherapy (+6.8% vs. +23%, p < 0.01). The change in pretibial subcutaneous tissue pressure was also significantly less with the former (+23.2% vs. 75.5%; p < 0.001). Valsartan monotherapy had no effect on these parameters.
Summary
Hypertension is the leading cause of CVD morbidity and mortality. Despite the availability of many effective antihypertensive agents, only 37% of the hypertensive patients achieve their target BP control. Majority of the patients with stage 2 or higher hypertension or those with high CVD risk require more than one agent to control their BP. Most guidelines now recommend initiating antihypertensive therapy with a combination of agents with complementary mechanisms of action in these patients. The fixed-dose combinations of various antihypertensive agents enhance patient adherence, convenience, and BP control while reducing adverse effects typically seen with using higher doses of a single agent. Calcium channel blockers and angiotensin receptor blockers are being increasingly used in fixed-dose combinations. Several randomized studies have demonstrated their superiority in achieving target BP control among various sub-groups while reducing the incidence of adverse events seen with monotherapy.
Disclosure
The author reports no conflicts of interest.