
Abstract
Fluoroquinolone antibiotics are relatively new drugs in anti-tuberculosis (TB) treatment, with the potential to become the first new class of drugs to be recommended for routine treatment since rifamycins in the 1960s. Later generation fluoroquinolones, including levofloxacin, gatifloxacin, and moxifloxacin have been found to be safe and well-tolerated in observational studies and phase 2 clinical trials, except for a risk of severe dysglycemias with gatifloxacin. These drugs currently are used as second-line agents in treatment of TB cases with drug resistance and drug intolerance, and empirically in treatment of infected contacts of patients with multi-drug resistant TB. Widespread use of fluoroquinolones for treatment of community acquired pneumonia and other bacterial infections is leading to the emergence and spread of strains of Mycobacterium tuberculosis that are fluoroquinolone-resistant, putting at risk the potential effectiveness of these drugs against TB. Clinical trials are under way to determine whether fluoroquinolone-based treatment regimens can shorten the duration of TB therapy. The ultimate contributions of fluoroquinolones to TB control remain to be determined.
Introduction
Tuberculosis (TB) is an age-old disease with a rich but tragic legacy that included responsibility for up to 600 deaths per 100,000 population in London around 1740. It continued to kill about half of all people developing the disease until shortly after World War II. 1 With the discovery of antituberculosis drugs and proof of their effectiveness in clinical trials beginning in the 1940s, TB became a curable disease. 2 Even with effective drug treatment available for the past half century, one third of the world's population remains infected and almost 2 million people die each year from this disease. 3
Pulmonary disease comprises approximately 80% of all cases of reported TB in the United States, 4 making it by far the most common form of the disease. Since sputum provides a convenient specimen for diagnosis and sputum culture results demonstrate response to therapy, 5 pulmonary TB is most often the disease form evaluated in clinical trials. Treatment regimens developed for pulmonary TB usually form the basis for treatment of extrapulmonary forms of the disease. 6
The current standard treatments for TB have undergone only minor changes since the late 1980s. For several decades, however, calls have gone out to develop new drugs and regimens for TB treatment for several reasons. 7 The duration and dosing frequency of current regimens places a large burden on treatment programs and patients. New drugs are needed for increasingly common and complicated drug-resistant strains of M. tuberculosis and for patients intolerant of first-line TB drugs. More effective treatments also are needed for treatment of latent TB infection (LTBI). Among the promising new agents for TB treatment are the fluoroquinolones. 8
Quinolones were first discovered in the early 1960s as an impurity in the production of chloroquine. 9 From the seminal impurity, the first quinolone to be marketed, nalidixic acid, which is primarily active against Escherichia coli and is still commercially available, was synthesized. Subsequent generations of quinolone antibiotics have shown broader antimicrobial activity and have become so popular that ciprofloxacin and levofloxacin are among the 100 most frequently prescribed drugs in North America. 9
Fluoroquinolones have been shown in vitro to have sterilizing activity against M. tuberculosis.10,11 They have been evaluated in TB patients since the mid 1980s 12 and in clinical trials of TB treatment since the early 1990s. Several of them remain viable alternatives for use as second line agents in TB treatment. Newer fluoroquinolones also are undergoing further evaluation of their potential to shorten the duration of treatment in current and future trials, especially levofloxacin, gatifloxacin, and moxifloxacin.13,14 Low minimal inhibitory concentrations and experience with safety and tolerability have encouraged widespread evaluation and use of these antibiotics worldwide for TB treatment.
Mechanism of Action
Quinolone antibiotics work by inhibiting bacterial cell division and gene expression.15,16 Bacterial deoxyribonucleic acid (DNA) fits within the cell through a process of twisting and counter-twisting into a compact super-coil. This process is enabled by the enzyme, topoisomerase II, also called DNA gyrase, which is found in all bacteria. DNA gyrase catalyzes a breakage and reunion cycle that compresses DNA into the super-coil. Quinolone antibiotics bind together with the topoisomerase and the strand of DNA and interfere with this process. Efforts are ongoing to describe the activity of fluoroquinolones more completely and to adjust their design to find more potent and better tolerated agents.9,17
Metabolism, Pharmacokinetics and Pharmacodynamics
Elimination of fluoroquinolones can be primarily renal (ofloxacin, levofloxacin and gatifloxacin),18,19 mixed renal and hepatic (ciprofloxacin and moxifloxacin),20,21 or primarily hepatic (trovafloxacin, grepafloxacin). 21 Protein binding is also variable (e.g. gatifloxacin 20%, levoflxacin 40%, moxifloxacin 50%). 19
In general, fluoroquinolones possess good to excellent bioavailability (70%–90% for most). 18 Divalent and trivalent cations, including Ca++, Mg++, Fe++ and Al+3 that are often found in antacids and other medications, can greatly decrease fluoroquinolone absorption, while food usually has a minimal effect.18,20,21 Commonly used drugs that frequently interact with other medications, such as theophylline, warfarin and ranitidine, appear to have minimal effect on fluoroquinolones that undergo even moderate hepatic metabolism, such as moxifloxacin. 20 These drugs are predominantly metabolized via the cytochrome P450 system, which is not involved in moxifloxacin metabolism. However, the most effective TB drug in current widespread use, rifampin, up-regulates the glucuronidation pathway involved in hepatic metabolism of moxifloxacin. Not surprisingly, therefore, co-administration of rifampin with moxifloxacin has been found to result in decreased blood levels of moxifloxacin as manifested by decreased area under the concentration-time curve (AUC).22,23 However, this interaction may not be clinically relevant when the recommended doses of rifampin and moxifloxacin are used.
Human pharmacokinetic and M. tuberculosis minimal inhibitory concentration (MIC) data for selected fluoroquinolones most often used in TB treatment are shown in Table 1. The newer fluoroquinolones (moxifloxacin, gatifloxacin) have longer half-lives allowing less frequent dosing. Moxifloxacin and gatifloxacin also have the best in vitro activity against M. tuberculosis with MICs of 0.12 to 0.5 μg/ml.24,25
Pharmacokinetic properties and minimal inhibitory concentrations of selected fluoroquinolones (based on references 18, 19, 24, 25, 27–29).
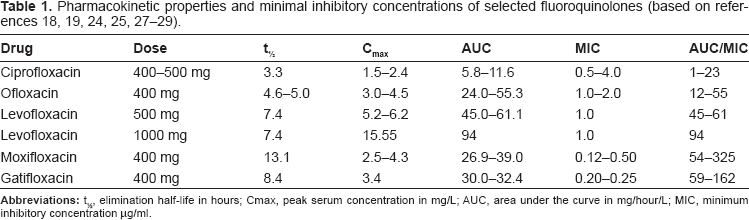
For non-mycobacterial infections, the ratio of AUC to MIC has been used to describe the efficacy of antibiotics with concentration-dependent killing, 19 and a mouse model suggests that this may be the case for fluoroquinolones in the treatment of TB. 26 Applying the AUC/MIC ratio, of the fluoroquinolones commonly used in TB treatment, moxifloxacin and gatifloxacin have the best ratios at 78 and 60, followed by levofloxacin at 45, and ofloxacin and ciprofloxacin at 12.25,27 By increasing the dose of levofloxacin to 1000 mg, an AUC/MIC ratio comparable to that for moxifloxacin and gatifloxacin can be achieved. 28 These calculated AUC/MIC ratios are derived from pharmacokinetic measurements made in healthy volunteers with frequent blood draws after a single dose of medication. 29 A recent study performed in patients with TB who had received five doses of medication found similar results with the best free AUC/MIC ratio being achieved in patients receiving 1000 mg of free levofloxacin (median 93.84), followed by 400 mg of gatifloxacin (median 66.18) and 400 mg of moxifloxacin (median 59.35). 28
Safety and Tolerability
Levofloxacin, gatifloxacin, and moxifloxacin have been well tolerated in clinical trials in adults. The numbers of adverse events and serious adverse events in these trials have not been statistically significantly greater in the fluoroquinolone arms than in the control arms.13,14,30 Severe dysglycemias, however, have been a greater problem for patients on gatifloxacin than for patients treated with other antibiotics.31,32 Levofloxacin also has been reported to have a small increased risk for dysglycemias, but other fluoroquinolones have not. A retrospective comparison between levofloxacin containing regimens and conventional first-line therapy found no difference in adverse event rates. 33 Pediatric data are very limited, so these drugs remain relatively contraindicated in children.
Tendonitis and Achilles tendon rupture have been associated with fluoroquinolone use, 19 although not in the published phase 2 trials of extended use for TB.14,30 Other potential adverse effects include prolongation of the QTc interval, central nervous system toxicity (e.g. headache, dizziness, confusion, seizures), gastrointestinal upset (e.g. nausea, vomiting, diarrhea) and dermatologic conditions (e.g. rash, photosensitivity). 19 Cardiac events attributable to QTc prolongation have not been reported in the published phase 2 trials of extended use for TB.14,30 Although hepatitis has been reported to occur with fluoroquinolones, moxifloxacin and levofloxacin have been shown to be well-tolerated by patients with hepatitis induced by first-line anti-TB drugs. 34 Finally, TB patients treated with fluoroquinolones also have been evaluated for Clostridium difficile-associated diarrhea, because of the association found in non-TB patients. A large retrospective study in Hong Kong among hospitalized patients on TB treatment found no statistically significant association with fluoroquinolone use in multivariable analysis. 35
Current Uses of Fluoroquinolones for TB
Treatment of drug-resistant TB
Fluoroquinolones are among the most commonly used medications for the treatment of drug-resistant TB, especially multidrug-resistant (MDR) TB–-defined as TB caused by a strain of M. tuberculosis that is resistant to at least isoniazid and rifampin. Table 2 shows current recommendations for incorporation of fluoroquinolones into drug-resistant TB treatment regimens.6,36 Treatment of drug-resistant TB, especially MDR TB, is complex because many of the drugs used are less effective and less well tolerated than first-line agents. Therefore, treatment of drug-resistant TB should be performed by or in consultation with a TB expert. Fluoroquinolones often are not recommended for the treatment of extensively drug-resistant (XDR) TB as by definition this form of TB is caused by isolates of M. tuberculosis resistant to a fluoroquinolone. Nevertheless, the World Health Organization (WHO) has recently recommended the use of “a later generation fluoroquinolone such as moxifloxacin” for patients with documented, or almost certain, XDR-TB. 37
Use of fluoroquinolones in the treatment of drug-resistant tuberculosis disease (based on recommendations from references 6 and 36).
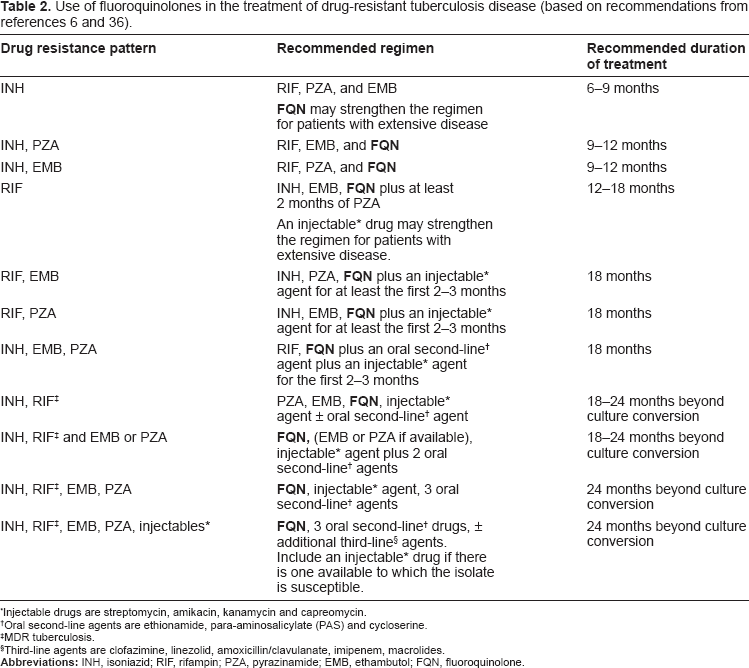
Injectable drugs are streptomycin, amikacin, kanamycin and capreomycin.
Oral second-line agents are ethionamide, para-aminosalicylate (PAS) and cycloserine.
MDR tuberculosis.
Third-line agents are clofazimine, linezolid, amoxicillin/clavulanate, imipenem, macrolides.
The clinical evidence supporting the use of fluoroquinolones in the treatment of drug-resistant TB is predominantly based on cohort studies and case series. For MDR TB, three observational studies have found improved outcomes associated with use of fluoroquinolones. In a cohort of 205 patients treated at a specialty hospital in Denver, Colorado, United States, from 1984 through 1998, the investigators evaluated the effect of fluoroquinolones on microbiological response, defined as “favorable” for patients with at least three consecutive negative sputum cultures over at least three months on treatment. 38 Among patients with sufficient data, 88% (116/132) of patients receiving fluoroquinolones had a favorable response compared to 70% (21/30) of those not receiving fluoroquinolones (odds ratio (OR) 3.11, 95% confidence interval (CI) 1.21–7.95). In Kaplan-Meier estimates of survival from all causes of death, fluoroquinolone use was associated with significantly improved survival (p = 0.01). Investigators of a multi-institutional MDR TB outbreak in New York City from 1990 to 1993 evaluated survival among 179 HIV-infected patients. 39 One hundred and nineteen patients treated with ciprofloxacin or ofloxacin < = 12 weeks survived a median of 5 weeks while 60 patients treated with ciprofloxacin or ofloxacin >12 weeks survived a median of 57 weeks (OR 3.5, CI 2.0–6.3 in multivariate analysis). Two hundred and ninety nine patients with MDR pulmonary TB diagnosed from 1992 to 1996 were evaluated in Taipei, Taiwan. 40 Cure was defined as “culture negative and documented to remain culture negative > = 1 month later and never documented to become positive again up to 18 months after commencing treatment.” Patients who received ofloxacin (125, 42%) were more likely to be cured (p = 0.002) and were less likely to die or fail in comparison with other patients.
Four other studies provide additional indirect evidence of the potential value of fluoroquinolones in MDR TB therapy by evaluating the impact of fluoroquinolone resistance or of previous treatment with fluoroquinolones on outcomes. Among 63 MDR TB patients admitted to Grantham hospital in Hong Kong from 1990 to 1997, 53 were treated with ofloxacin and 10 with levofloxacin. 41 Ofloxacin resistance, present in 13 patients (21%), was found in 14% (7/51) of patients with successful treatment and 50% (6/12) of patients with treatment failure or death and was independently associated with adverse outcomes in multivariate analysis (OR 13.5, CI 2.2–83.1). In an investigation of 204 MDR TB patients who began treatment in Latvia in 2000, resistance to ofloxacin was found to be a predictor of death or treatment failure (OR 2.6, CI 1.2–5.4). 42 In a Turkish study of 158 patients with MDR TB treated between 1992 and 1999, the absence of previous treatment with ofloxacin (which would be an indicator of likely current susceptibility to ofloxacin) was associated with a cure (negative smears and cultures throughout treatment for at least 18 months or 24 months in the absence of first-line drugs) or probable cure (negative smears and cultures throughout treatment for at least 6 months) (p = 0.005). 43 A European group evaluated the impact of fluoroquinolone resistance on outcomes of treatment for MDR TB in Estonia, Germany, Italy and the Russian Federation. 44 They found that fluoroquinolone resistance, compared to an absence of fluoroquinolone resistance, among MDR TB patients was associated with a higher proportion of deaths, 20% (17/87) vs. 12% (40/338) (relative risk 1.86, CI 1.11–3.11), and a higher proportion of treatment failures, 15% (13/87) vs. 9% (31/338) (relative risk 1.84, CI 1.05–3.23).
Despite favorable findings from retrospective investigations, the two systematic reviews have highlighted the lack of randomized, controlled trials of fluoroquinolone use in MDR-TB therapy.14,30
M. tuberculosis susceptibility to fluoroquinolones has mostly been found to be a class-characteristic. 24 Resistance to one fluoroquinolone implies resistance to others, although published data from clinical specimens are limited. Laboratories that test clinical isolates for second line drug susceptibility often test for ofloxacin to represent susceptibility or resistance to the fluoroquinolone class of antibiotics. 45 One recent study of 41 clinical isolates found full cross-resistance between ofloxacin, moxifloxacin, and gatifloxacin among 25 M. tuberculosis strains, and one strain which was resistant to moxifloxacin and gatifloxacin but susceptible to ofloxacin. 46 Earlier studies, however, show susceptibility to later generation fluoroquinolones in some M. tuberculosis isolates that are resistant to earlier generation fluoroquinolones.47–49 Cross resistance and the use of genetic markers to represent fluoroquinolone resistance require further study.
There is limited evidence upon which to base the choice of fluoroquinolone in MDR TB treatment. If one extrapolates from experience with non-mycobacterial respiratory infections, the AUC/MIC ratio predicts that moxifloxacin, gatifloxacin and levofloxacin (especially at the higher dose of 1000 mg/day) have the best potential efficacy. Little is known, however, about tolerability of higher doses. The problem of dysglycemia associated with gatifloxacin has complicated the use of this medication, requiring close screening and monitoring. Hepatotoxicity can potentially complicate the use of moxifloxacin, especially in regimens containing other drugs that are hepatotoxic. This is much less of a concern than it is for isoniazid and pyrazinamide. However, in MDR TB, these issues may not be as important because isoniazid and rifampin, and often pyrazinamide, will not be included in the medication regimen. Some experts recommend levofloxacin as the preferred fluoroquinolone in MDR TB therapy, largely because of its generally favorable safety and tolerability and because of the relatively extensive clinical experience with this drug in the treatment of MDR TB compared to moxifloxacin. 6 Some institutions are treating hospitalized MDR patients with 800 mg moxifloxacin daily. Some patients treated at this dose describe a feeling of agitation similar to that caused by caffeine (David Ashkin, personal communication). Data on pharmacokinetics and tolerability of this dose are needed.
Drug Intolerance
Another potential use for fluoroquinolones is as a substitute for first-line TB medications to which a patient is intolerant. Three retrospective studies examined the use of older fluoroquinolones (ciprofloxacin and ofloxacin with the lowest in vitro activity against Mycobacterium tuberculosis) in this setting.50–52 Two investigations studied patients with liver dysfunction in whom ciprofloxacin or ofloxacin and other non-hepatotoxic medications were substituted for standard first-line therapy.50,51 In the third investigation, ciprofloxacin was used in patients with either drug resistance or drug intolerance, but the analysis was not stratified. 52 In all three studies, the fluoroquinolones were well tolerated and most patients had significant clinical improvement with the fluoroquinolone-containing regimens. Levofloxacin, mostly administered to patients intolerant to one of the first-line TB anti-TB drugs, was found to be safe and effective in a retrospective Canadian study. 33 A prospective study in Taiwan found levofloxacin and moxifloxacin not to cause additional hepatotoxicity when administered to patients with hepatitis induced by first-line anti-TB drugs. 34
MDR LTBI
Treatment of latent TB infection (LTBI) is generally recommended for persons who have been recently infected in close contact to a patient with infectious TB. 53 No treatment has been demonstrated to be efficacious for the treatment of LTBI caused by M. tuberculosis resistant to isoniazid and rifampin (i.e. MDR) so recommendations for treatment are based on expert opinion.36,54 As potential regimens for treatment of MDR LTBI, CDC initially recommended either ethambutol and pyrazinamide or pyrazinamide and a fluoroquinolone if compatible with drug-susceptibility test results from the source case isolate of M. tuberculosis. 54
Studies on safety and tolerability of fluoroquinolones for LTBI treatment are very limited. A report of 48 solid organ transplant recipients who were receiving levofloxacin and pyrazinamide for presumed MDR LTBI revealed that 32 (67%) discontinued therapy prematurely because of adverse events. 55 Gastrointestinal intolerance accounted for more than half of the adverse events. In a case series of 17 persons in Ontario, Canada with suspected MDR LTBI who were treated with levofloxacin and pyrazinamide, all 17 discontinued treatment because of a variety of adverse effects including musculoskeletal, central nervous system, gastrointestinal and dermatologic. 56 A report of a series of high school students and teachers treated with ofloxacin and pyrazinamide after exposure to an infectious patient with MDR TB noted similar issues with frequent adverse effects. 57 Of 22 persons started on a 12-month course of therapy, only nine completed the course of medication. Hepatotoxicity was common, both symptomatic and asymptomatic. In reviewing these reports, it is difficult to discern how many of the adverse effects were due to each individual drug versus the combination of the two. Regardless, the combination of a fluoroquinolone and pyrazinamide for MDR LTBI does not appear to be well tolerated and results in low completion rates. This has led to the suggestion that perhaps fluoroquinolone monotherapy or a fluoroquinolone in combination with ethambutol may be better tolerated and increase the likelihood of completion. 36
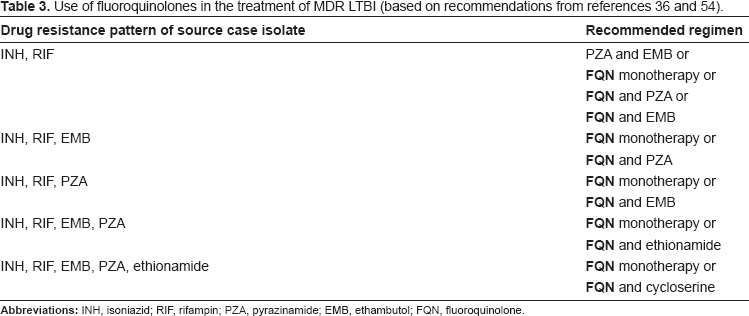
Recently, the Francis J. Curry National Tuberculosis Center (San Francisco, CA, United States) published updated recommendations for potential treatment regimens. 36 Table 3 shows regimens that incorporate fluoroquinolones based on drug-susceptibility test results from the source case isolate of M. tuberculosis. Of note, these recommendations introduce the use of monotherapy with a fluoroquinolone and designate levofloxacin or moxifloxacin as the fluoroquinolones of choice. 36 The recommended duration for all MDR LTBI treatment regimens is 6–12 months.36,54
Use of fluoroquinolones in the treatment of MDR LTBI (based on recommendations from references 36 and 54).
Active TB needs to be assiduously excluded before starting any LTBI treatment regimen, especially monotherapy, because of the risk of causing more drug resistance. Clinical monitoring through two years after exposure is indicated for close contacts of infectious MDR TB patients, whether they are treated or not.36,37,53
Acquisition of Fluoroquinolone Resistance and the Treatment of Community Acquired Pneumonia
The need for multidrug therapy to prevent the development of drug resistance is a cardinal and defining feature of TB treatment. This characteristic, less typical of most other infectious diseases, has lead to concerns that TB, when misdiagnosed as community acquired pneumonia and treated with fluoroquinolone mono-therapy, could acquire fluoroquinolone-resistance.
Studies examining the potential for fluoroquinolone treatment of mistakenly presumed community acquired bacterial pneumonia, which is in fact TB, have yielded varied results. An investigation in Baltimore, MD, United States found that two of 55 (4%) of patients had fluoroquinolone resistance prior to initiation of TB therapy, and that both patients had prior fluoroquinolone exposure during treatment for presumed respiratory and non-respiratory non-mycobacterial infections. 58 A study from Taiwan revealed that fluoroquinolone resistance was limited to MDR TB strains and not found in other isolates leading the authors to conclude that fluoroquinolone resistance resulted from their use in treatment of MDR TB and not from use for other purposes in the general community. 59 Investigators examining data from two provinces in Canada and from Tennessee reported that fluoroquinolone resistance occurred only in TB patients who had received multiple prior prescriptions for a fluoroquinolone, but not those who received a single prescription.45,60 Clinicians should consider the possibility of TB before empirically diagnosing community acquired pneumonia, in particular when prescribing a fluoroquinolone for treatment.61,62
In addition to enabling emergence of drug resistance, the antimycobacterial activity of fluoroquinolones during monotherapy of suspected non-tuberculous conditions poses other risks. By temporarily suppressing M. tuberculosis, and by giving the impression that the patient's disease is being treated, fluoroquinolone therapy also can mask a tuberculous etiology and cause delays in diagnosis, as shown in two retrospective studies63,64 and a recent randomized controlled trial. 65
Ironically, fluoroquinolone use for treatment of MDR TB in children has been associated with emergence of invasive pneumococcal disease caused by fluoroquinolone-resistant Streptococcus pneumoniae. 66 As its widespread use for non-mycobacterial infections is associated with increasing prevalence of resistant M. tuberculosis, its increasing use for TB appears to be associated with increasingly common resistance in non-mycobacterial infections. Emerging drug-resistance, both for tuberculosis and for non-tuberculous infections, may negate the benefits of new classes of drugs. 67
Clinical Trials for Use of Fluoroquinolones to Shorten Duration of TB Treatment
As described above, moxifloxacin has been proposed as a safe and effective second line treatment for TB. This drug also has the potential to shorten the necessary duration of current first-line TB treatment regimens. Experimental data on M. tuberculosis suggest that moxifloxacin has the lowest minimum inhibitory concentration (MIC) of the available fluoroquinolones.68,69 Animal studies indicate that moxifloxacin, more than the other fluoroquinolones tested, has potent sterilizing activity and an additive effect with isoniazid.70–73
Several phase 2 clinical trials have been completed recently that help to answer these questions. The surrogate marker of cure that has been best investigated for use in phase 2 clinical trials is the culture result of sputum collected at 2 months of treatment, 74 even though its value is limited in comparison to the gold standard of determination of relapse following completion of treatment as the measure of cure.75,76 Clinical trials adding rifampin to treatment regimens during the 1970's found 15% to 20% advantages in 2-month culture conversion rates with 9-month rifampin-containing regimens and cure rates comparable to the then-standard 18 month regimens. 2 Trials of pyrazinamide that resulted in shortening standard treatment from 9 months to 6 months, with comparable cure rates, showed 2-month culture conversion advantages averaging 13% when pyrazinamide was added to the regimens.77–81 Similarly large advantages from adding another drug to the regimen would support undertaking phase 3 trials. Other criteria for progressing to phase 3 trials have also been proposed. 82
An Indian study of 3-, 4-, and 5-month regimens substituting ofloxacin for ethambutol, with rifampin isoniazid, and pyrazinamide showed 92% to 98% 2-month culture conversion rates and rates of relapse during 2 years of follow-up as low as 2% and 3%. 83 However, no concurrent control regimen of standard treatment was included and 36% of enrolled patients were not evaluable for relapse.
Encouraged that fluoroquinolones could potentially help to shorten treatment of drug-susceptible disease, and with evidence that moxifloxacin has the lowest MICs among currently available fluoroquinolones, phase 2 trials were undertaken to evaluate moxifloxacin for ethambutol substitutions during intensive phase treatment of AFB smear-positive TB in humans. Later mouse data showed that substituting moxifloxacin for isoniazid resulted in an even larger reduction in CFU counts, 84 which helped to guide the design of subsequent clinical trials.
Tuberculosis Trials Consortium (TBTC) Study 27 was a phase 2 randomized placebo-controlled trial with a factorial design, comparing moxifloxacin to ethambutol, both regimens in combination with isoniazid, rifampin and pyrazinamide. 85 It also compared 5-day per week treatment with 3-day per week treatment. The main endpoint was culture-negativity at 2 months, combining results from liquid and solid media. When complete, no difference was found between treatment arms, and no statistically significant difference was found between treatment frequencies. Sputum collected every two weeks, however, showed more subjects in the moxifloxacin group than in the ethambutol group having culture negative sputum at 4 and 6 weeks. This difference was no longer present by 8 weeks.
A similar phase 2 trial was undertaken in Brazil, evaluating a moxifloxacin substitution for ethambutol during intensive phase treatment, with the 8-week culture comparison on a single solid medium, Lowenstein-Jensen (LJ), as the primary endpoint. 86 This trial found moxifloxacin to have higher rates of culture negativity on weekly comparisons with the ethambutol regimen and to have an almost 20% higher rate of culture negativity at 2 months.
A third ethambutol substitution study was performed in Durban, South Africa, testing ofloxacin, gatifloxacin, and moxifloxacin during otherwise standard intensive phase treatment. 87 This trial used both standard and intensive microbiology techniques, on liquid and solid media. The intensive technique employed quantitative culturing of numerous overnight sputum collections, with serial sputum colony counts (SSCC), and regression modeling of the SSCC data. None of the experimental regimens showed a statistically significant advantage in proportion with negative culture at the end of two months of treatment, although moxifloxacin showed the largest simple proportion negative among the drugs tested. Regression modeling, however, showed statistically significantly faster and greater development of culture negativity with gatifloxacin and moxifloxacin, compared to the control and ofloxacin regimens.
TBTC Study 28 evaluated a moxifloxacin substitution for isoniazid and also compared 2-month culture results as the primary endpoint. 88 A secondary evaluation was of time to conversion, measuring sputum collections every two weeks. The study found 5% more culture negativity at 2 months for the moxifloxacin group, which was not statistically significant. No statistically significant difference was found in time to conversion between the two regimens. As in the Durban study, 87 this study also found higher rates of 2-month culture negativity on solid media than on liquid media.
The conflicting results between these studies raise questions about the microbiological methods used in phase 2 studies and have prompted discussion about the applicability of murine models to human tuberculosis. 89 Previous trials have employed mostly solid media, most of which were LJ, 2 but liquid media are becoming increasingly common in TB control programs worldwide, making an understanding of the differences in findings between these media increasingly important for the design and interpretation of clinical trials. Single-site comparisons of culture results on different media during the course of standard treatment and evaluation for relapse during follow-up after treatment completion will help to establish methodology for future trials of new treatment regimens.
Phase 3 treatment shortening studies with moxifloxacin and gatifloxacin have been started, 82 despite the mixed results from phase 2 studies. These randomized controlled trials, with long enough follow-up periods to compare relapse and cure rates, also will help to refine methodologies for future clinical trials, including the approach to differences between solid and liquid media.
Although the question of whether 3- or 4-month moxifloxacin-containing regimens will be effective remains open, the phase 2 studies reported to date do support the safety and effectiveness of moxifloxacin as a second-line agent to use in TB treatment. One major caution to keep in mind is the risk of drug resistance emerging as a result of the current very widespread use of fluoroquinolone antibiotics.62,90,91
Conclusion
Fluoroquinolones appear to be safe and effective second-line agents for treatment of pulmonary TB. They are under investigation as first-line agents in treatment regimens that are shorter than those recommended in current national and international guidelines.
While confirmation of the efficacy of fluoroquinolones in the treatment of MDR TB is desirable, there are relatively few drugs available for MDR TB. No second-line medications have been validated for MDR TB treatment through randomized, controlled trials14,30 and, in general, other second-line drugs are more toxic and have less in vitro activity against M. tuberculosis than fluoroquinolones. Under these circumstances, the incorporation of fluoroquinolones in MDR-TB therapy, as indicated in Table 2, is warranted.
As for MDR TB, despite the relative paucity of data, use of fluoroquinolones as a substitute for first-line drugs in the setting of drug intolerance is reasonable, especially in comparison to other second-line medications.
Moxifloxacin and levofloxacin are the most promising fluoroquinolones currently available for use in TB treatment, although the optimal dosages of both have not been determined. Fluoroquinolone treatment of children with TB and LTBI also has not been addressed in clinical trials. Future clinical trials will help to determine additional potential contributions of fluoroquinolones to TB treatment.8,92
Meanwhile, fluoroquinolones can only be recommended as second-line agents for TB treatment and their injudicious use, in the absence of careful and accurate diagnosis, places the whole class of drugs at risk for becoming irrelevant due to drug resistance.
Disclaimer
The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention.
Disclosures
This manuscript has been read and approved by all authors. This paper is unique and is not under consideration by any other publication and has not been published elsewhere. The authors report no conflicts of interest.