
Abstract
Imiquimod (trade name Aldara™) is a small molecule of the imidazoquinoline family, a group of nucleoside analogs that were first synthesized as potential antiviral agents. It has since been discovered to activate both innate and adaptive immunity, as well as apoptosis. Clinically, it has been approved for three indications thus far: external genital warts, actinic keratosis, and superficial basal cell carcinoma. In addition to these applications, a number of off-label uses have been reported in the literature. In this review, we summarize and discuss the literature describing imiquimod's mechanism of action, its approved and off-label clinical uses, and its safety and tolerability.
Introduction
Imiquimod(1-(2-methylpropyl)-1H-imidazo[4,5-c] quinolin-4-amine) (trade name Aldara™) is a small molecule of the imidazoquinoline family, a group of nucleoside analogs that were first synthesized as potential antiviral agents.1–4 Although no direct antiviral activity was initially found in vitro, imiquimod has since been shown to stimulate both innate and adaptive immunity, as well as induce apoptosis.
This novel biological activity has piqued clinical interest and led to multiple trials testing imiquimod's efficacy and safety across a range of skin pathologies.5–8 Currently, it is approved for external anogenital warts, actinic keratosis (AK), and superficial basal cell carcinoma (sBCC). In addition, its use has been investigated in non-genital cutaneous warts, genital herpes, molluscum contagiosum, squamous cell carcinoma in situ (SCCIS), squamous cell carcinoma (SCC), nodular BCC (nBCC), lentigo maligna, metastatic melanoma, vulvar and vaginal intraepithelial neoplasia (VIN/VAIN), mycosis fungoides, Kaposi's sarcoma, infantile hemangioma, pyogenic granuloma, leishmaniasis, scars/keloids, and in immunosuppressed patients.
In this review, we will describe imiquimod's molecular and cellular mechanism of action, as well as its pharmacokinetic profile. Next, we will report salient clinical trials that have characterized its efficacy and safety for specific skin diseases. We conclude this review with an overview of imiquimod's role in therapy, a survey of the gaps in the current research literature, and a look towards possible applications in the future.
Mechanism of Action
Shortly after imiquimod was found to have no direct in vitro effect against viruses, several lines of in vivo data demonstrated that it did still harbor indirect antiviral activity. In guinea pigs, the drug acted both prophylactically and therapeutically against primary herpes simplex virus (HSV) infection when administered orally, parenterally, intravaginally, or topically.2,9 In addition to activity against HSV, imiquimod reduced cytomegalovirus (CMV) viremia when given to guinea pigs 24 hours before virus inoculation. 10 In 1992, Sidky et al demonstrated for the first time that imiquimod possessed anti-tumor activity as well. 11
This effect was inhibited by concurrent administration of anti-interferon-α (IFN-α) serum.
Imiquimod was thus shown to have an antiviral effect, although it was not through a direct mechanism as originally predicted. In addition, it was shown to have unanticipated anti-tumor activity. Subsequent studies delineated cellular and molecular mechanisms that might account for these biological effects. In the most established of these models, imiquimod induces the release of inflammatory cytokines, thereby triggering the innate immune system. Imiquimod stimulates adaptive immunity as well, most likely indirectly by acting on antigen-presenting cells (APCs). In addition to its effects on innate and adaptive immunity, more recent data has shown that imiquimod induces apoptosis as well.
Imiquimod in innate immunity
Vertebrates possess immune systems that can be divided into two components: innate and adaptive immunity. 12 Cells of the innate response consist of macrophages, neutrophils, basophils, mast cells, eosinophils, and natural killer (NK) cells; these cells coordinate the initial, rapid response to pathogens. This response is marked by its relative nonspecificity. Rather than target highly unique antigens, the cells of this system scan for broadly conserved pathogen associated molecular patterns (PAMPs). Cytokines released during innate immune responses include tumor necrosis factor (TNF)-α, interleukin (IL)-1, IL-6, IL-10, IL-12, IL-15, IL-18, type I interferons such as IFN-α, and chemokines.
A number of studies have demonstrated imiquimod's ability to induce cytokines of the innate immune system, both in vitro and in vivo. In cultured mouse spleen cells, imiquimod induced IFN-α, IL-6, and TNF-α. 13 In mouse macrophage cells, imiquimod stimulated TNF-α, as well as 2'5‘-oligoadenylate synthase (2-5-OAS), an enzyme regulated by IFN-α/β. 14 In cultured monkey peripheral blood monocytes (PBMCs), imiquimod induced IFN-α, IL-1β, IL-6 and IL-8. 15 In addition, messenger RNA (mRNA) levels of IFN-α, IL-1α, IL-1, and the IFN-inducible gene MxA were increased with imiquimod.
In human PBMCs, increases were reported in serum protein concentrations of IFN-α, TNF-α, IL-1, IL-1RA, IL-6, IL-8, IL-10, IL-12 p40, granulocyte colony stimulating factor (G-CSF), macrophage inflammatory proteins 1-α and 1-β, and macrophage chemotactic protein.16,17 In addition to protein induction, imiquimod caused increases in mRNA levels of IFN-α, IFN-β, IL-6, IL-8, and TNF-α in human PBMCs. 18 In human keratinocytes and epidermal cancer cells, Kono et al observed mRNA induction for IL-6 and IL-8, but not for IL-1α. 19
These in vitro data have been corroborated by in vivo studies. In guinea pigs, imiquimod increased serum levels of IFN-α when given orally, intravaginally, topically, or parenterally. 20 When given orally or parenterally to mice, the drug induced IFN-α, TNF-α, and IL-6. 13 Imbertson et al applied imiquimod to the flanks of hairless mice and rats and found increased IFN-α mRNA and protein and TNF-α protein. 21 In cynomolgus monkeys, oral imiquimod increased serum levels of IFN-α and IL-1RA. 15 Tyring et al treated genital warts with topical 5% imiquimod and analyzed the skin biopsy for human papilloma virus (HPV) DNA and cytokine mRNA. Polymerase chain reaction (PCR) revealed that imiquimod-treated lesions were significantly reduced in viral DNA, and reverse transcriptase (RT)-PCR revealed increased mRNA expression of IFN-α and TNF-α. 22
How does imiquimod initiate this cytokine response on a molecular level? One possibility is through the Toll-like receptor (TLR), a cell surface transmembrane receptor homologous to the Toll protein found in Drosophila melanogaster.23–25 Like D. melanogaster Toll, human TLRs can activate nuclear factor-κB (NF-κB) signaling, as well as induce downstream expression of IL-1, IL-6, and IL-8. 26 Interestingly, overexpressed TLR also induced the costimulatory B7 protein, indicating that TLRs can activate adaptive immunity. A total of 10 human TLRs have been discovered, and they are now established as a critical type of pattern recognition protein (PRP) on the surface of innate immune cells that can recognize PAMPs on invading pathogens.27,28
The link between imidazoquinolines and TLRs was made when Hemmi et al reported that mice deficient in TLR7 showed a muted immune response to resiquimod (R-848), a derivative of imiquimod. 29 Furthermore, mice deficient in MyD88, an adaptor protein in TLR signaling, showed a similarly inhibited immune response. Jurk et al provided in vitro evidence that R-848 can activate both TLR7 and TLR8 to stimulate NF-κB in a dose dependent manner. 30 These data suggested that imiquimod's immunologic activity is mediated, at least in part, by activation of TLR7 and/or TLR8, leading to activation of NF-κB and subsequent gene expression of its proinflammatory cytokine targets.
In support of these data, Megyeri et al identified increased levels of NF-κB-DNA complexes after imiquimod application to human PBMCs. 18 In addition, they found increased complexes of a second transcription factor, α4F1. A third transcription factor, signal transducer and activator of transcription 1 (STAT-1), also seems to be a critical downstream transcription factor, as mice deficient in this protein show a blunted response to imiquimod. 31 Together, these studies identify STAT-1, NF-κB, and a4F1 as important downstream signaling components of the imiquimod response.
Imiquimod in adaptive immunity
The ability of TLRs to stimulate both innate and adaptive immunity raised the possibility that imiquimod might also regulate both arms of the immune system. Unlike innate immunity, adaptive immunity is hallmarked by the specificity of its response to unique antigens. 12 The adaptive immune system consists of B and T-lymphocytes, as well as the APCs that are necessary to activate them within lymphoid tissue. T-helper (Th) cells are among the major releasers of cytokines within the adaptive immune system, and they are divided into two classes based on the cytokines they release. Th1 cells generally activate cellular responses to pathogens, including macrophages and cytotoxic T cells (Tc cells); this cytokine profile consists of IFN-γ, lymphotoxin, and TNF-β. Th2 cells activate a humoral response by stimulating B cells; cytokines of this subtype include IL-4, IL-5, and IL-13.
Although imiquimod has not been shown to directly stimulate lymphocyte proliferation or cytokine release, it has been reported to induce adaptive immunity in the presence of APCs. In 1999, Wagner et al reported that imiquimod could induce release of the Th1 cytokine IFN-γ in both murine and human cell cultures. 15 The cytokines IL-12 and IFN-α were necessary for IFN-γ induction. In addition to inducing IFN-γ, imiquimod has been shown to have a broader stimulatory effect on antigen presentation. In mice, topical imiquimod led to a reduced number of Langerhans cells (LCs) in the epidermis, and the remaining epidermal LCs were morphologically activated. 32 In addition, imiquimod enhanced LC migration from skin to draining lymph nodes following antigen challenge. Consistent with these murine data, studies in cultured human LCs showed that imiquimod-treated LCs could induce 30-300-fold greater T-cell proliferation relative to untreated control LCs.33,34 Furthermore, imiquimod-treated LCs showed expression of several cell-surface co-stimulatory proteins, including CD1a, HLA-DR, HLA-DP, HLA-DQ, CD40, CD86, and CD80.
Several studies have also reported imiquimodmediated activation of B-cells. In purified B-cells from mice and humans, imiquimod stimulated proliferation and secretion of immunoglobulins in the absence of other immunocytes. 35 These data suggest that unlike T-cells, B-cells may be directly activated by imiquimod. Bishop et al suggested that this effect may be through binding and activation of CD40, a B-cell surface receptor. This group reported that R-848 can induce signaling mechanisms and cellular changes similar to those activated by CD40 binding.36,37
Imiquimod in apoptosis
In addition to its wide-ranging activation of the immune system, imiquimod has also been shown by more recent data to possess pro-apoptotic activity. In human basal cell carcinoma (BCC), topical application induces increased expression of the pro-apoptosis death receptor CD95 (Fas). 38 In addition, several groups have reported decreases in the pro-survival protein Bcl-2, and transfection of Bcl-2 into tumor cells blunts imiquimod's pro-apoptotic effect.39,40 Finally, downstream of these signaling events, inhibition of caspases reduces imiquimod-induced apoptosis, indicating that this proteolytic cascade is a necessary part of the mechanism. 40
Pharmacokinetics
Several studies have investigated the pharmacokinetics of imiquimod in the context of specific skin diseases. Harrison et al reported a study of 58 adult patients with 5-20 AK lesions divided into three groups. 41 The first group (12 males/11 females) applied 12.5 mg of imiquimod to facial lesions. The second group (11 males) applied 25 mg to bald areas of the scalp. The third group (12 males/12 females) applied 75 mg to their hands and forearms bilaterally. All groups applied their specified dosages three times a week for up to 16 weeks. Pharmacokinetic data were taken biweekly, and after the first and last dose.
Serum concentrations of imiquimod after first and last doses were low, reflecting minimal dermal absorption. 41 After the first dose of imiquimod, peak serum concentration (Cmax) was 0.09, 0.14, and 0.78 ng/mL for the face, scalp, and hand/arm groups, respectively. After the final dose, Cmax values were 0.12, 0.21, and 1.35 ng/mL for the three groups. Area under the serum concentration-time curve (AUC) also increased with multiple dosing. After the first dose, AUC was 1.99, 3.32, and 23.6 ng/h/mL for the face, scalp, and hand/arm groups, respectively. After the last dose, AUC was 2.06, 4.89, and 29.1 ng/h/mL. Metabolite levels were undetectable in any of the three groups after the first dose and were transiently detected only in the face and hand/arm groups after the last dose. The calculated half-life (t1/2) after the last dose of imiquimod was 23, 21, and 27 hours for the face, scalp, and hand/arm groups, respectively. Urinary excretion of imiquimod or any of its five metabolites was minimal, ranging from 0.05% to 0.24% of the total dose among the three groups.
Another study by Myhre et al studied imiquimod pharmacokinetics in 22 children (ages 2-12 years) with molluscum contagiosum. 42 All children had ≥10% of their total body surface area affected by molluscum contagiosum and were assigned to between 12.5-37.5 mg of imiquimod per dose. Each patient applied their assigned dose three times per week for a total of 4 weeks. As in the Harrison et al study, serum concentrations of imiquimod were low after both first and last dose, regardless of the size of individual dose. Cmax values ranged from 0.1 to 0.6 ng/mL after the first dose, and from 0.2-2.2 ng/mL after the last dose. AUC ranged from 0.1-3.0 ng/h/ml after the first dose and from 1.4-10.8 ng/h/mL after the last dose. Both Cmax and AUC values rose proportionally with dose normalized for body weight (p < 0.05 for both Cmax and AUC). After the first dose, 5 out of 22 children had detectable metabolites, all at a serum concentration ≤0.1 ng/mL. After the last dose, 8 out of 22 children had measurable metabolites, with a maximum value of 0.23 ng/mL.
Clinical Applications
In addition to its three approved indications for external anogenital warts, actinic keratosis, and superficial basal cell carcinoma, imiquimod's efficacy has been tested in a number of other dermatologic diseases. We present the data behind the approved indications first, with the other studies to follow.
External anogenital warts
External anogenital warts were the first approved indication for imiquimod (1997). There have been a number of randomized, double-blinded, vehicle-controlled trials testing topical imiquimod for this indication (Table 1).43–46 Summing these four trials, a total of 743 patients were studied. Three of the 4 studies tested 1% or 5% imiquimod given 3 times per week.43,45,46 The fourth study by Beutner et al tested 1% or 5% imiquimod given daily. 44 Total treatment duration was 8-16 weeks. Complete clearance rates ranged from 37%-70% for 5% imiquimod, 14%-21% for 1% imiquimod, and 0%-11% for vehicle (p-values for individual trials listed in Table 1). Recurrence rates at 10-12 week post-treatment follow-up ranged from 13%-19% for 5% imiquimod, 0%-17% for 1% imiquimod, and 0%-10% for vehicle. Arican et al conducted a longer, 6-month post-treatment follow- up and found that 6 of 6 patients, treated with 5% imiquimod three times per week for 12 weeks, experienced recurrence. 45
Efficacy of imiquimod on external genital warts.
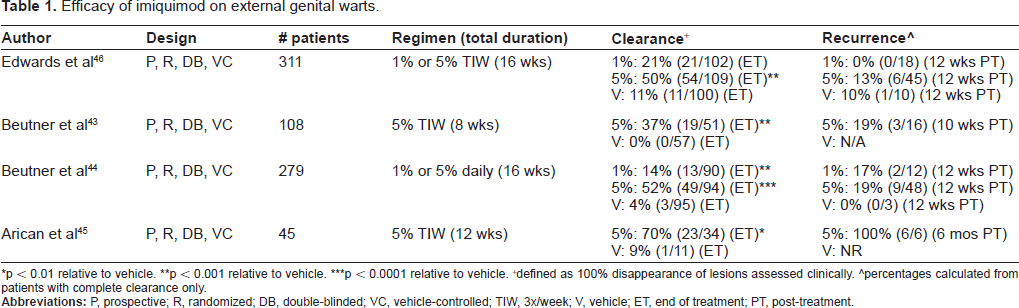
p < 0.01 relative to vehicle.
p < 0.001 relative to vehicle.
p < 0.0001 relative to vehicle.
defined as 100% disappearance of lesions assessed clinically.
percentages calculated from patients with complete clearance only.
There are relatively few clinical trials comparing imiquimod against other therapies used for external anogenital warts. In a 2001 abstract, Romero-Sanchez et al reported results of a prospective, randomized, double-blinded trial with a total of 110 men. 47 Half the men were assigned to 5% imiquimod applied three times per week for 16 weeks, and the other half were assigned to 1% 5-fluorouracil (5-FU) applied three times per week for 16 weeks. Fifty-eight percent of the imiquimod group experienced complete clearance after a mean of 12 weeks, compared to 36% of the 5-FU group after a mean of 13 weeks (p > 0.05). At 12 weeks post-treatment follow-up, sustained clearance rates were 56% in the imiquimod group and 36% in the 5-FU group.
In 2006, Schofer et al reported a prospective, randomized, open-label trial comparing imiquimod versus ablative therapy for external anogenital warts. 48 Three hundred and fifty-eight patients were randomized to one of three arms: ablation alone, 5% imiquimod cream three times a week for up to 16 weeks, or combined therapy with ablation and 5% imiquimod cream (applied for 12 weeks after wound healing). Ablative techniques included electrocautery, laser therapy, liquid nitrogen, and surgical excision. At the end of the treatment phase, patients undergoing ablation alone had a 92% complete clearance rate, compared to 65% in the imiquimod only group and 73% in the combination therapy group (statistical significance not reported). Patients with complete clearance were followed up for a total of 6 months. At the 3 month follow-up, 14 of 87 patients (16%) in the ablation only group reported recurrence, compared to 6 of 96 patients (6%) in the imiquimod monotherapy group and 6 of 72 patients (8%) in the combination group (p < 0.03 for ablation only vs. imiquimod only; p = 0.142 for ablation only vs.combination). By the 6 month follow-up, a total of 23 of 87 patients (26%) in the ablation only group had reported recurrence. This was compared with 6 of 95 patients (6%) in the imiquimod monotherapy group and 6 of 71 patients (8%) in the combination group (p < 0.004 comparing ablation only group to either imiquimod group). Thus, imiquimod, either alone or in combination with ablative therapy, appears to have lower initial clearance rates than ablation alone, but leads to a statistically significant lower recurrence rate at 6 months.
Actinic keratosis
Imiquimod 5% was approved for treatment of actinic keratosis (AK) in 2004. Four randomized, double-blinded, vehicle-controlled trials addressing this indication are summarized in Table 2.49–52 A total of 1433 patients with AK of the face and balding scalp were included in these trials. Two of the trials designed treatment regimens divided into two 4-week courses of 5% imiquimod three times a week, separated by a 4-week rest period.49,50 Total treatment duration ranged from 4 to 16 weeks. Complete clearance rates ranged from 45%-55% for 5% imiquimod and 2%-15% for vehicle (p-values for individual trials listed in Table 2). Jorizzo et al conducted a 1-year post-treatment follow-up and found recurrence rates of 39% in the 5% imiquimod group and 57% in the vehicle group. 50
Efficacy of imiquimod on facial and balding scalp actinic keratoses.
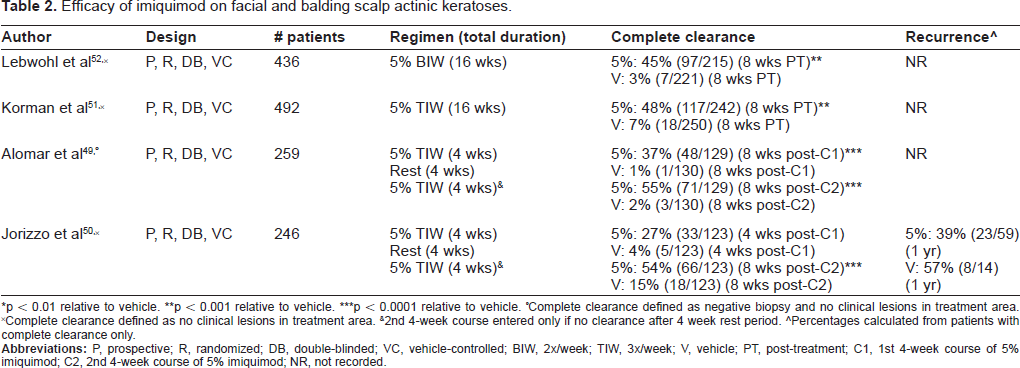
p < 0.01 relative to vehicle.
p < 0.001 relative to vehicle.
p < 0.0001 relative to vehicle.
Complete clearance defined as negative biopsy and no clinical lesions in treatment area.
Complete clearance defined as no clinical lesions in treatment area. &2nd 4-week course entered only if no clearance after 4 week rest period.
Percentages calculated from patients with complete clearance only.
A study by Tanghetti and Werschler compared 5% imiquimod with 5% 5-FU in a prospective, randomized trial of 36 patients with AK lesions on face or balding scalp. 53 Patients received either 5% 5-FU cream twice daily for 2-4 weeks or 5% imiquimod cream twice weekly for 16 weeks. At week 24, 84% of patients in the 5-FU group experienced complete clearance, compared with 24% of imiquimod-treated patients (p < 0.01).
In another comparative study, Krawtchenko et al also found that 5-FU was more efficacious initially than imiquimod, but in addition, they showed higher sustained clearance rates with imiquimod than 5-FU. 54 In this study, patients were randomized to one or two courses of cryosurgery (20-40 seconds per lesion), 5% 5-FU (twice daily for 4 weeks), or one or two courses of 5% imiquimod (three times per week for four weeks each). 17 of 25 patients (68%) in the cryosurgery group, 23 of 24 patients (96%) in the 5-FU group, and 22 of 26 patients (85%) in the imiquimod group experienced initial clearance (p < 0.05). At 12-month follow-up, 1 of 25 patients (4%) in the cryosurgery group, 8 of 24 patients (33%) in the 5-FU group, and 19 of 26 patients (73%) in the imiquimod group had sustained clearance of the total treatment field (p < 0.01). These data suggest that imiquimod has more long-term efficacy against AK lesions than either cryosurgery or topical 5% 5-FU.
Basal cell carcinoma
Superficial basal cell carcinoma (sBCC) is the third and most recently approved indication for imiquimod (2005). A number of prospective, randomized, double-blinded, placebo-controlled trials have shown 5% imiquimod to be superior to the natural course of the disease (Table 3).55–58 Twelve hundred total patients were included in these trials. Treatment regimens included 3 times per week, 5 times per week, once daily, and twice daily. Treatment duration ranged from 6-12 weeks. Complete clearance rates, defined histologically or clinically, ranged from 52%-100% for 5% imiquimod-treated patients and 3%-19% for the vehicle group (p-values for individual trials listed in Table 3). The 100% clearance rate occurred in 10 patients receiving 5% imiquimod twice daily. 56 Gollnick et al performed a 5-year post-treatment follow-up and found a recurrence rate of 11%. 57
Efficacy of imiquimod on superficial basal cell carcinoma.
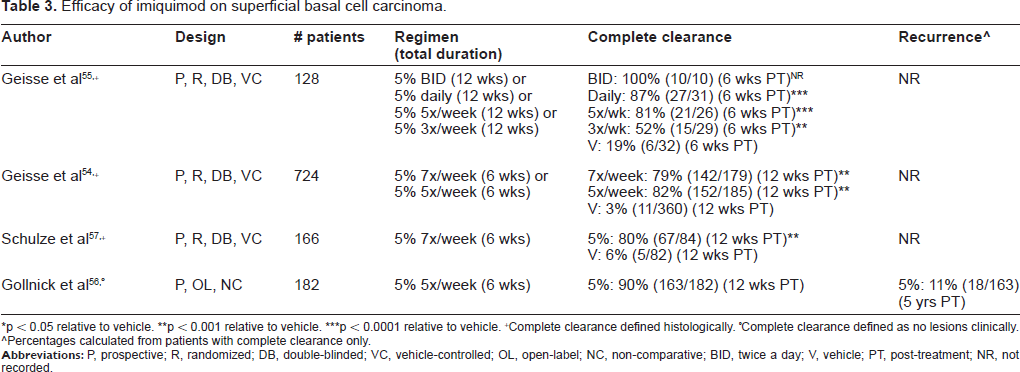
p < 0.05 relative to vehicle.
p < 0.001 relative to vehicle.
p < 0.0001 relative to vehicle.
Complete clearance defined histologically.
Complete clearance defined as no lesions clinically.
Percentages calculated from patients with complete clearance only.
In 2002, Shumack et al evaluated imiquimod's efficacy in the treatment of nodular BCC (nBCC). 59 They performed two trials, the first of which was a prospective, open-label, non-controlled study of 99 patients. This trial assigned patients to one of four dosing regimens: once daily for 3 or 7 days per week, or twice daily for 3 or 7 days per week. The total duration of treatment was 6 weeks. The second trial was a prospective, randomized, double-blinded, vehicle-controlled trial of 92 patients. Patients in this trial applied either 5% imiquimod or vehicle once daily for 3, 5, or 7 days per week, or twice daily for 7 days per week. Unlike the first trial, total treatment duration during this trial was 12 weeks. In both of these trials, 5% imiquimod once daily for 7 days per week was the most efficacious regimen, with 25 of 35 patients (71%) in the 6-week trial and 16 of 21 patients (76%) in the 12-week trial showing complete clearance of tumor on this regimen (p < 0.001 for 5% imiquimod once daily vs. vehicle in 12-week trial). Enrollment into the twice daily, 7 days per week regimen was halted shortly after study initiation because of severe local skin reactions. Therefore, only a small number of patients were randomized to this group (1 patient in the 6-week trial, and 4 patients in the 12-week trial). The single patient in the 6-week trial failed to respond completely to imiquimod, and 3 of 4 patients in the 12-week trial were complete responders.
Several studies in the literature address the role of imiquimod as adjunct therapy in the treatment of BCC. In 2006, Spencer et al reported a randomized, prospective, double-blind, vehicle-controlled study of 20 patients with nBCC. 60 These patients were randomized to three cycles of curettage and electrodessication (C&D), followed by either 5% imiquimod or vehicle cream once daily for 1 month. At 8 weeks post-treatment follow-up, 10% of the adjunct imiquimod group experienced recurrent tumor, compared to 40% of the placebo group (statistical significance not reported). Rigel et al performed a prospective, non-controlled study of 57 patients with nBCC or sBCC. 61 These patients were treated initially with curettage alone, followed by 5% imiquimod 5 times per week for 6 weeks. At 1 year follow-up, none of the patients demonstrated residual BCC.
Non-genital, cutaneous warts
Several trials have explored imiquimod's efficacy in non-genital warts. In 2000, Hengge et al reported a prospective, open-label, non-comparative trial of 50 patients with cutaneous warts resistant to previous therapies, including salicylic acid, local surgery, cryotherapy, laser vaporization, electrodessication, trichloroacetic acid (TCA), intralesional interferon, and X-ray treatment. 62 Of the 50 patients, 20 had warts on their hands, 16 on their feet, 10 on their face, and 4 were disseminated. Imiquimod 5% was applied five days per week for up to 16 weeks or complete clearance. Fifteen of 50 patients (30%) experienced complete clearance, while 13 patients (26%) experienced a >50% reduction in wart area after a mean treatment period of 9.2 weeks. Stratification by lesion site revealed that response rates (partial and complete combined) were higher on the trunk, face, and hands (75%, 70%, and 60%, respectively) than on the feet (37.5%).
In 2002, Grussendorf-Conen et al reported a prospective, open-label, non-comparative trial of 37 patients with resistant cutaneous warts (mean duration 6.3 years). 63 Warts were located on the hands and/ or feet of 36 of 37 patients; the last patient had warts on the knee. Imiquimod 5% was self-applied twice daily for 24 weeks or complete clearance. 10 of 37 patients (27%) cleared completely, 18 patients (49%) showed a >50% reduction in wart area, and 5 patients (14%) showed a >50% reduction.
Herpes simplex virus
In a prospective, randomized, double-blinded, placebo-controlled trial, Schacker et al investigated whether imiquimod could alter the natural history of HSV-1 and/or 2 infections. 64 This study included 124 patients with genital herpes (both HSV-1 and HSV-2 subtypes included) who had at least 6 recurrences per year. Patients in the midst of a recurrence applied either 5% imiquimod or vehicle once, twice, or three times weekly for a total of 3 weeks. A 16-week observation period followed the treatment period. The primary endpoint was median time to next recurrence after treatment. Median time to recurrence was 53, 54, 60, and 64 days for placebo, imiquimod once, twice, and three times per week, respectively (no statistical significance between groups). Despite a slight trend towards increased time to recurrence, 5% imiquimod appears to have no clear effect on HSV recurrence when dosed and applied in this manner.
Molluscum contagiosum
Several randomized, prospective, double-blinded, placebo-controlled trials have tested topical imiquimod in children (ages 1-12) with molluscum contagiosum.8,65,66 Imiquimod 5% was applied three times per week for up to 12 weeks in the Theos et al trial or 16 weeks in the other two trials, conducted by 3M. Theos et al found that 4 of 12 imiquimod-treated patients (33%) completely cleared versus 1 of 11 (9%) in the placebo group at the end of the 12-week treatment period (statistical significance not reported). The two 3M-conducted trials, though larger in scope (n = 323 and 379, respectively), found no statistically significant difference between imiquimod and placebo (clearance in 24% of imiquimod group and 26%-28% of placebo group).
Squamous cell carcinoma in situ
Squamous cell carcinoma in situ (SCCIS) has been identified as a possible therapeutic target for imiquimod. In 2006, Patel et al conducted a randomized, prospective, double-blinded, placebo-controlled study of 31 patients with biopsy-proven SCCIS. 67 Patients applied either 5% imiquimod or vehicle cream daily for up to 16 weeks and were assessed at 28 weeks. Eleven of 15 patients (73%) in the imiquimod group achieved complete clearance, compared with 0% of the placebo group (p < 0.001). In addition, at 9 month follow-up, none of the eligible patients showed recurrence of their disease.
Squamous cell carcinoma
In a 2005 abstract, Li et al reported a prospective, non-controlled trial of 20 patients with invasive SCCs receiving a combination of 5% imiquimod, tretinoin, calcipotriene, diclofenac, and hydrocortisone valerate as part of a protocol called OLCAT-005. This protocol was initiated at two times per week and increased to at least three times per week for 12 weeks. Dose schedule per lesion was optimized by an Individualized Maximally Tolerated Dose (IMTD) regimen. 68 At 12-week post-treatment follow-up, 33 of 35 lesions (94%) showed complete histologic clearance, and none of the cleared lesions showed recurrence at 5 years.
Melanoma
A few prospective, non-controlled trials have investigated a role for imiquimod in lentigo maligna. Naylor et al assigned 30 patients with lentigo maligna to 5% imiquimod once daily for 3 months. 69 At the 1 month post-treatment follow-up, 26 of 28 evaluable patients (93%) had complete histological clearance. Over 80% of the complete responders showed no recurrence after 1 year. In smaller studies, Powell et al used 5% imiquimod three times per week for 6 weeks, Fleming et al used 5% imiquimod daily for 6 weeks, and Wolf et al used 5% imiquimod daily for up to 13 weeks. Powell et al reported complete clearance in 10 of 12 patients (83%), Fleming et al in 4 of 6 patients (67%), and Wolf et al in 5 of 5 patients (100%).70–72
In 2007, Green et al reported a prospective, non-controlled trial of 10 patients with subcutaneous and cutaneous melanoma metastases. 73 Imiquimod 5% was applied daily to the lesions for 4 weeks, followed by 5% imiquimod daily plus intralesional IL-2 injections (0.36 million international units) three times per week every two weeks for 4 weeks. This was followed by imiquimod every other day for 4 weeks after lesion disappearance, plus IL-2 three times per week every 4 weeks. A total of 182 lesions were treated, and complete response to this regimen was observed in 74 lesions (40.7%). Ninety-one percent of the completely responding lesions were cutaneous.
Contrary to the moderate success reported by Green et al Kowalzick and Eickenscheidt reported the case of a 68-year old man with primary malignant melanoma of the temple in whom topical imiquimod was ineffective. Following excision of his primary tumor, multiple cutaneous and subcutaneous metastases arose, and his disease progressed fatally despite irradiation, chemotherapy, and topical imiquimod three times a week. No intralesional therapy, however, was given in this case. 74
Vulvar and vaginal intraepithelial neoplasia
Several prospective, non-controlled studies have been performed to investigate the efficacy of imiquimod in vulvar intraepithelial neoplasia (VIN) (grade 2/3) and vaginal intraepithelial neoplasia (VAIN). Marchitelli et al assigned patients to 5% imiquimod three times a week for up to 16 weeks and reported the highest efficacy rates among these studies: 6 of 8 patients (75%) had complete clearance assessed by colposcopy, and 2 of 8 patients (25%) had partial clearance (defined as >50% decrease in lesion area). 75 In addition, post-treatment histopathology showed no evidence of VIN in 7 of 8 patients (88%). Le et al reported that a 16 week course of therapy led to complete histological response in 9 of 17 patients (53%) and partial response in 5 of 17 (29%). 76 Todd et al reported a lower rate of response, with 4 of 15 patients (27%) showing clinical improvement after 16 weeks of therapy. 77 Wendling et al reported a trial of 12 patients, in which 3 of 12 (25%) achieved complete clearance and 4 of 12 (33%) partial response (defined as >75% decrease in lesion size). 78
In 2003, Buck and Guth reported a prospective, non-controlled study in 56 women (42 available for follow-up) with primarily low-grade VAIN. 79 Of the 14 women lost to follow-up, one of them reported vulvar excoriation as the reason for discontinuation; the other 13 discontinued for either unknown or non-drug related reasons. These patients applied 0.25 g of cream into the vagina once a week for 3 weeks. Thirty-six of 42 patients (86%) showed complete clearance by colposcopy at 1 week or later after conclusion of treatment. Five patients cleared after an additional cycle of therapy (total 2 cycles), and the last patient cleared after 2 additional cycles (total 3 cycles). Therefore, all women available for follow-up eventually showed clearance of their VAIN after 1-3 cycles of imiquimod topical therapy.
Mycosis fungoides
A small prospective, randomized, double-blinded, vehicle-controlled trial by Chong et al studied imiquimod's effects in mycosis fungoides. 80 This trial included only 4 patients with mycosis fungoides; 3 were assigned to imiquimod once daily for 16 weeks, and the remaining patient was assigned to vehicle. In the imiquimod cohort, mean surface area decreased by 9% on imiquimod-treated lesions and increased by 40% on untreated control lesions (statistical significance not reported). Within the placebo group, mean lesion surface area increased by 40%.
Kaposi's sarcoma
Celestin-Schartz et al conducted a prospective, open-label, non-comparative trial of 17 human immunodeficiency virus (HIV)-negative patients (14 males, 3 females) with classic or endemic Kaposi's sarcoma. 81 Patients applied 5% imiquimod cream under occlusion three times a week for 24 weeks. At 36 weeks, 2 of 17 patients (12%) had a complete response and 6 of 17 (35%) had a partial response. Six of 17 patients (35%) experienced tumor progression.
Infantile hemangioma
McCuaig et al conducted a prospective, open-label, non-comparative trial of 16 infants (mean age 4.1 months) with previously untreated, non-ulcerated superficial or mixed infantile hemangioma. 82 Imiquimod 5% was applied 3 to 7 times per week for 16 weeks. Lesions were assessed at the end of the 16 week treatment as well as at 16 weeks post-treatment. No changes in mean lesion area, volume, depth, or elevation were observed at either timepoint. Erythema was significantly improved at the 16-week post-treatment timepoint compared to baseline (p < 0.01).
In a prospective, non-comparative trial, Welsh et al treated 10 infants with infantile hemangiomas with 5% imiquimod 5 days per week for up to 16 weeks. 83 Four of the 10 infants (40%) had complete resolution of their lesions, another 4 infants (40%) experienced partial resolution, 1 infant did not respond to therapy (10%), and the remaining infant discontinued at 3 weeks in order to receive microembolizaton. A recent case series of 5 infants by Barry et al reported similar results. 84 Two of the 5 infants (40%) had a complete response, 2 (40%) had a partial response and 1 had no response to treatment.
Pyogenic granuloma
A number of case reports describe imiquimod's efficacy for pyogenic granuloma. The largest of these reports describes 5 children (ages 6 months to 4 years) treated with 5% imiquimod cream. 85 Three of the children were treated daily; one was treated daily for 1 week and then every other day for 4 more applications; the fifth child was treated three times a week. The duration of treatment ranged from 2-4 weeks, and all 5 children experienced full resolution of their pyogenic granuloma during this period.
Adults with pyogenic granuloma appear to benefit from imiquimod as well. A report by Georgiou et al described an 82-year old man with recurrent pyogenic granuloma on his hand that was treated with 5% imiquimod twice daily for 3 weeks. At 8 month follow- up, he had no evidence of recurrence. 86
Skin diseases in immunosuppressed patients
Because imiquimod is thought to work primarily by stimulating innate and adaptive immunity, its efficacy in immunosuppressed patients has been an interesting point of study. In 1999, Gilson et al reported a prospective, randomized, double-blinded, vehicle-controlled study of 100 HIV-positive patients (97 men and 3 women) with external anogenital warts across 13 institutions in the United Kingdom and United States. 87 These patients were randomized to either 5% imiquimod or vehicle cream, three times per week for up to 16 weeks. Inclusion criteria were age ≥18 years, CD4 count ≥100 cells/μL, and Karnofsky score ≥70. Eleven percent of imiquimod treated patients demonstrated complete clearance of their warts, compared to 6% of placebo patients (p = 0.488). Although complete clearance was not significantly different for the imiquimod group, imiquimod-treated patients did demonstrate a higher rate of partial clearance (≥50% reduction in wart area) than placebo patients (38% vs. 14% respectively; p < 0.05). Overall, these results support the model that imiquimod is less effective in the context of HIV.
Transplant patients represent another cohort in which immunosuppression could hinder imiquimod's effects. A randomized, prospective, double-blinded, vehicle-controlled study by Ulrich et al investigated the safety of imiquimod in 43 transplant patients (kidney, heart, or liver) with AK on the face or balding scalp. Patients applied 5% imiquimod or vehicle cream three times a week for 16 weeks, regardless of lesion clearance. At 8 weeks post-treatment follow-up, 18 of 29 patients (62%) treated with imiquimod experienced complete clearance, compared to 0 of 14 patients treated with vehicle (statistical significance not reported). 88
In another prospective, randomized, double-blinded, placebo-controlled trial, Brown et al studied imiquimod in 20 renal transplant patients at high risk of skin cancer, as predicted by skin type, previous sun exposure, and time since transplantation. 89 Patients were required to have equivalent areas of viral warts, actinic keratoses, or other premalignant skin lesions (assessed clinically) on both dorsal forearms or hands. The patients applied either 5% imiquimod or vehicle cream to lesions on one dorsal forearm/hand three times per week for up to 16 weeks. The other forearm/hand served as an untreated internal control. At week 16, 5 of 14 imiquimod-treated patients (36%) showed reduced histologic dysplasia at the treatment site relative to the untreated contralateral side. One of 6 patients (17%) in the vehicle group showed reduced histologic dysplasia (p = 0.32 for imiquimod vs. vehicle groups). In addition, 7 of 14 imiquimod-treated patients (50%) had reduced non-genital warts, compared with 0 of 6 placebo patients (p < 0.05). Imiquimod still seems to be effective in transplant patients.
Leishmaniasis
Several studies have examined the efficacy of imiquimod for leishmaniasis infection. Firooz et al performed a prospective, randomized, assessor-blind, vehicle-controlled trial of 119 patients across 2 primary health clinics. 90 All patients were treated daily with 20 mg/kg of meglumine antimoniate, given intramuscularly for 14 days. In addition, patients were randomized to receive either 5% imiquimod or placebo cream 3 times per week for 4 weeks. At four weeks after the end of treatment, 26 of 59 imiquimod-treated patients (44.1%) and 29 of 60 placebo patients (48.3%) showed clinical cure, revealing no therapeutic benefit of imiquimod over meglumine antimoniate alone (p = 0.64).
In contrast, another randomized, prospective, double-blind, placebo-controlled trial did show a benefit with imiquimod. Miranda-Verastegui et al assigned 40 patients to meglumine antimoniate (20 mg/kg) daily for 20 days plus either 5% imiquimod or vehicle cream every other day for 20 days. 91 At 1 month post-treatment follow-up, 50% of the imiquimod group achieved cure, compared to 15% of the vehicle group (p < 0.02). At 3 months post-treatment, 72% of the imiquimod group and 35% of the vehicle group had achieved cure (p < 0.02).
Keloids/scars
Based on its ability to induce IFN-α, several small studies have examined imiquimod use in the prevention of keloid recurrence. Berman and Kaufman performed a non-comparative pilot study of 12 patients with 13 keloids (12 on the earlobe, 1 on the back). 92 The patients’ keloids were excised, and starting the night of excision, imiquimod 5% cream was applied daily for 8 weeks. At 16 weeks post-treatment, 11 of 11 assessed keloids had not recurred. In contrast, Cação et al examined 9 patients with keloids on the trunk who were treated with surgical excision and application of imiquimod 5% cream daily for 8 weeks. 93 One patient was lost to follow-up, and all 8 of the remaining patients experienced recurrence by 20 weeks post-excision. Larger scale studies are required, and the varied success rates may reflect differences in resection location.
Regarding imiquimod's potential role in scar reduction and cosmesis, Berman et al conducted a prospective, randomized, double-blinded, vehicle-controlled trial of 18 patients, each with two skin lesions diagnosed as melanocytic nevi in a similar anatomic area of skin. 94 Each patient underwent surgical excision of both lesions; one lesion was treated with 5% imiquimod daily for 4 weeks, and the other was treated with vehicle. At week 8, investigators rated the wounds on overall cosmesis, erythema, induration, and pigmentary alteration. Vehicle-treated wounds received significantly better cosmesis and erythema scores than imiquimod-treated lesions (p < 0.01). Vehicle-treated lesions also scored more favorably for induration and pigmentary alteration, but to a lesser degree (p = 0.065 and 0.021, respectively).
Safety and Tolerability
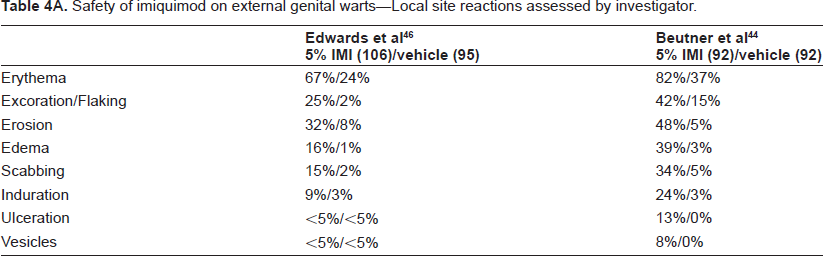
Several large studies of imiquimod's local and systemic tolerability exist for its approved indications (external genital warts, actinic keratosis, superficial basal cell carcinoma). The results of these safety studies are summarized in Tables 4, 5, and 6.
Safety of imiquimod on external genital warts–-Local site reactions assessed by investigator.
Safety of imiquimod on external genital warts–-Local site reactions reported by patient.
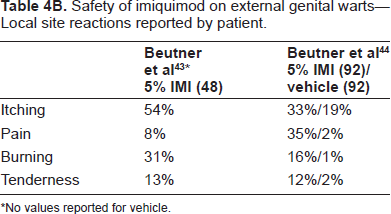
No values reported for vehicle.
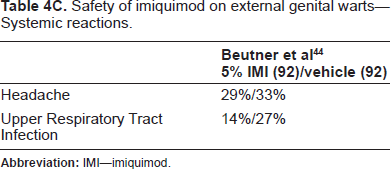
Safety of imiquimod on external genital warts–-Systemic reactions.
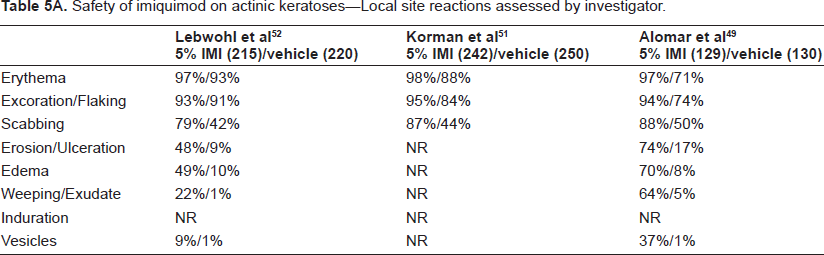
Safety of imiquimod on actinic keratoses–-Local site reactions assessed by investigator.
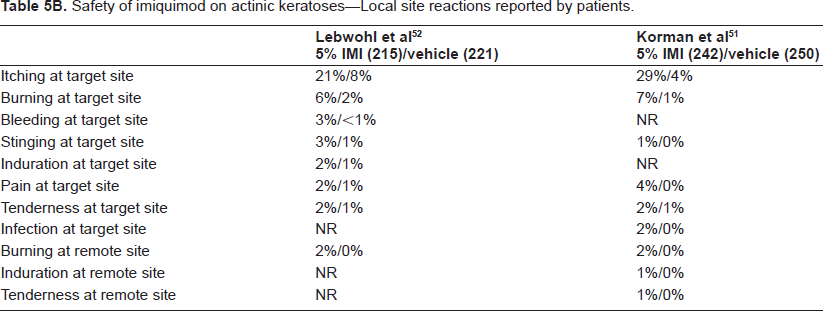
Safety of imiquimod on actinic keratoses–-Local site reactions reported by patients.
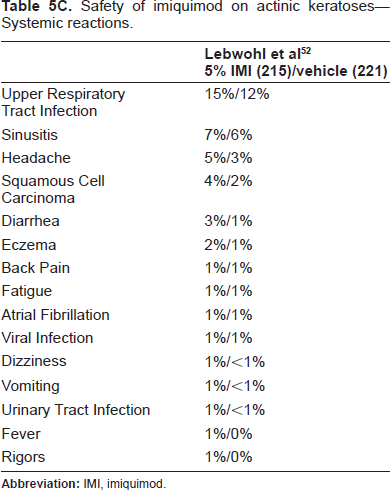
Safety of imiquimod on actinic keratoses–-Systemic reactions.
Safety of imiquimod on superficial basal cell carcinoma–-Local site reactions assessed by investigator.
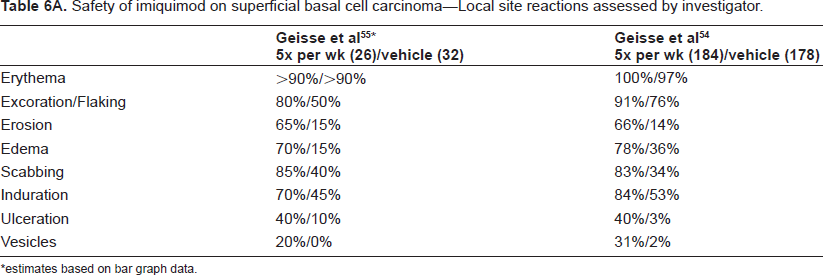
estimates based on bar graph data.
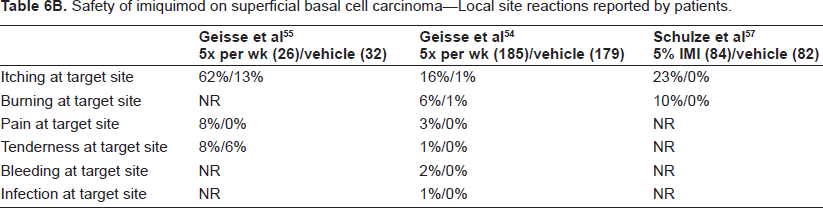
Safety of imiquimod on superficial basal cell carcinoma–-Local site reactions reported by patients.
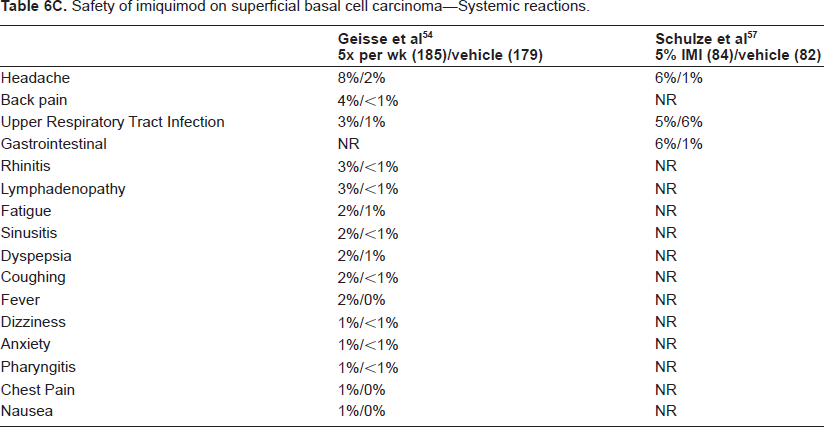
Safety of imiquimod on superficial basal cell carcinoma–-Systemic reactions.
Summary of safety trials
Across indications, the most common local skin reaction (LSR) assessed by investigators was erythema. Sixty seven to 82% of patients with external genital warts, 97%-98% of patients with AK, and 90%-100% of patients with sBCC experienced this reaction.43,44,46,49–52,55,56,58 Other commonly-experienced LSRs included excoriation/flaking, erosion/ulceration, edema, scabbing, and induration. Vesicles were less common than the other reactions, ranging from <5% of patients with external genital warts in one study to 37% of patients with AK in another study.46,49
Interestingly, there was a greater rate of certain LSRs in patients with AK or sBCC relative to those with external genital warts. Among AK patients, the rates of erythema, excoriation/flaking, and scabbing were 97%-98%, 93%-95%, and 79%-88%, respectively. Among sBCC patients, the analogous rates were 90%-100%, 80%-91%, and 83%-85%. Among patients with external genital warts, these rates were substantially lower: 67%-82% for erythema, 25%-42% for excoriation/flaking, and 15%-34% for scabbing. It is difficult to attribute this difference to application frequency, as part of the data for external genital warts came from a study which used 5% imiquimod daily for 16 weeks. 44 Other possible causes of this difference include anatomic site, nature of the skin lesion, and demographic differences between the study populations.
Regarding patient-reported adverse events, the most common local adverse event was application site reaction. In particular, itching was most commonly reported, with 16%-62% of all imiquimod-treated patients reporting this symptom at some time. In addition, pain, burning, and bleeding at the target site were reported to a lesser degree.
Systemic adverse events (SAEs), including flu-like symptoms, were minimal. In their trial, Beutner et al reported the most common SAE to be headache (29%) and upper respiratory tract infection (14%). 44 Consistent with this, Geisse et al also reported headache as the most common SAE (8%), followed by back pain (4%), upper respiratory tract infection (3%), rhinitis (3%), and lymphadenopathy (3%). 55 Lebwohl et al reported upper respiratory tract infection in 15%, sinusitis in 7%, and headache in 5%. 52 This group also described changes in hemoglobin and platelet levels but did not specify how many patients this affected or the degree of change. Jorizzo et al qualitatively reported one patient with a transient fall in leukocytes and absolute neutrophil count (ANC). 50
Safety in immunosuppressed patients
The previously cited study by Ulrich et al investigated the safety of imiquimod in 43 transplant patients (kidney, heart, or liver) with AK on the face or balding scalp. Patients applied 5% imiquimod or vehicle cream three times a week for 16 weeks, regardless of lesion clearance. No graft rejections or laboratory abnormalities were found in the imiquimod group throughout the 16-week course of therapy. Though skin reactions were evaluated at 8 weeks post-treatment, no mention was made of graft evaluation at this timepoint. 88
Another retrospective study of 24 transplant patients (18 kidney, 4 kidney-pancreas, and 2 heart) tested the safety of imiquimod in treating warts, AK, and bowenoid papulosis. 95 Imiquimod 5% was applied three times a week over a median of 9 weeks. All measures of graft function were normal.
Reportable adverse reactions
Several case reports describe imiquimod-induced exacerbations of previously controlled skin diseases. In one report, Yang et al described a 67-year old man who developed fever, myalgias, fatigue, and exacerbation of pityriasis rubra pilaris (PRP) after a 2-week application of imiquimod three times per week to focal areas on the scalp and right cheek. 96
Similar exacerbations of psoriasis have been reported in the literature. Gilliet et al reported a 58-year old man who received 5% imiquimod daily for a single psoriatic plaque on his back. 97 Over the next 10 weeks, his lesion increased 4-fold in size and was associated with new smaller plaques on his back and legs. Rajan et al described a 64-year old woman with long-standing, well-controlled psoriasis who began treating sBCC lesions on her trunk with 5% imiquimod daily. 98 By the fifth week, she had developed psoriatic plaques both at the treatment site as well as distantly on her legs. Interestingly, both Gilliet et al and Rajan et al describe psoriatic eruptions at sites distant from imiquimod application.
Three case reports describe the appearance of pemphigus-like lesions with imiquimod use.99–101 The first patient treated two sBCCs on her back and shoulder with 5% imiquimod 5 days per week and within two weeks developed vesicles and crusts at the treatment site as well as on her neckline and lips; biopsy of the neckline showed an intraepidermal acantholytic blister consistent with pemphigus vulgaris. 99 The second patient used imiquimod for high grade VIN and experienced blistering of her vulva; biopsy of her vulva revealed an intraepidermal blister with suprabasal separation. 100 The third patient applied 5% imiquimod daily to a suspected sBCC on her face and discontinued after 2 months because of redness and pain. 6 months after starting treatment, a biopsy revealed pemphigus foliaceus. 101
Conclusions: Current and Future Roles of Imiquimod
To date, the FDA has approved three indications for imiquimod: clinically typical, nonhyperkeratotic actinic keratoses on the face or scalp of immunocompetent adults; biopsy-confirmed, primary superficial basal cell carcinoma in immunocompetent adults with a maximum tumor diameter of 2.0 cm on the trunk, neck, or extremities (excluding hands and feet), only when surgical methods are less appropriate and follow-up can be assured; and external genital and perianal warts in patients 12 years and older.
The approved therapeutic regimen for each of these indications is as follows: AK - 5% cream 2 times per week for 16 weeks; sBCC - 5% cream 5 times per week for 6 weeks; external genital warts - 5% cream 3 times per week until total clearance or up to 16 weeks.
The superiority of imiquimod over placebo has been well established for each of these indications. Regarding AK, the trial using the approved regimen (2 times per week for 16 weeks) reported complete clearance rates of 45% in imiquimod-treated patients compared to 3% in the placebo group at 8-week post-treatment follow-up. 52 A three times per week regimen for 16 weeks resulted in similar clearance rates (48% imiquimod vs. 7% placebo). 51 Two studies using three times per week dosing for two 4-week courses separated by a 4-week rest period cited 54%-55% overall clearance in imiquimod groups compared to 2%-15% in placebo groups.49,50 For sBCC, the approved regimen (5 times per week/6 weeks) resulted in clearance rates of 82%-90% for the imiquimod groups versus 3% for the placebo groups.55,57 A maximum clearance rate of 100% was achieved with twice per day dosing over 12 weeks. 56 For external genital warts, the approved regimen (3 times per week for up to 16 weeks) achieved a clearance rate of 50% in the imiquimod group compared to 11% in the vehicle group. 46 In a second study, treating at the same frequency for only 8 weeks led to a lower clearance rate (37%), while a third study reported a 70% clearance rate with three times per week dosing for a total of 12 weeks.43,45 A fourth study suggested that daily dosing did not add significant benefit, with a complete clearance rate of 52%. 44
For all these indications, the next vital piece of information is how imiquimod directly compares to other standard therapies with regard to long-term clinical efficacy, financial cost, ease of use, and side effect profile. Unfortunately, the literature addressing this question is scarce. One study compared 5% imiquimod with 5% 5-FU in 36 patients with AK and found that complete clearance rates were much higher in the 5-FU group (84% vs. 24%). 53 However, Krawtchenko et al showed that 5% imiquimod has significantly higher sustained clearance rates at 12-month follow-up than 5% 5-FU (73% vs. 33%). 54 Another study concerning external anogenital warts compared 5% imiquimod with 1% 5-FU and found no statistically significant difference, although there was a trend towards increased clearance rates in the imiquimod group (56% sustained clearance in imiquimod group vs. 36% in 5-FU group at 12 week follow-up). 47
In short, the current literature firmly supports imiquimod's treatment success compared to the natural evolution of AK, sBCC, and external anogenital warts, but does not offer much help to clinicians in deciding between imiquimod and concurrent therapies. In theory, imiquimod seems an attractive choice, with substantive clearance rates, ease of patient use, avoidance of invasive techniques, and relatively benign toxicity profile. In order to make this a more quantitative decision, however, head-to-head, randomized, prospective, double-blinded trials are necessary.
In addition to the three current indications for imiquimod, it seems reasonable to assume that further therapeutic targets could be approved in the future. In several of the skin disorders mentioned previously, off-label use of imiquimod for non-genital warts, SCCIS, SCC, VIN/VAIN, melanoma, and pyogenic granulomas may be useful. Other creative applications for imiquimod have started to emerge in the literature as well. For example, its potential use as a vaccine adjuvant for infectious pathogens and tumors makes theoretical sense and has been supported by several preclinical studies.102,103 As the first commercially available TLR agonist, imiquimod has vividly demonstrated the broad applicability of this novel class of agents. It should continue to advance disease therapy, both by its own efficacy as well as by serving as a molecular blueprint upon which to create further derivatives. Resiquimod, one such derivative that is available orally as well as topically, has already shown promise with its own distinct molecular and therapeutic profile.
Disclosures
The authors report no conflicts of interest.