
Abstract
Osteoarthritis is a major cause for pain worldwide and is increasingly so as the number of elderly people continues to grow. Finding treatments that are effective and safe for this pain has been challenging primarily because gastrointestinal risks increase with aging as well. One step in the direction of improvement was the development of selective COX-2 inhibitors, which as a group have lower gastrointestinal adverse reaction rates than traditional non-steroidal anti-inflammatory drugs. However, increases in cardiovascular adverse events with some of these have dampened initial enthusiasm for this approach. One of these inhibitors, celecoxib remains available in most areas of the world for use in pain associated with osteoarthritis. This review illustrates how best to consider it's role in the current treatment of pain associated with arthritis with an emphasis on osteoarthritis.
Keywords
Introduction
It is often useful to classify arthritis as belonging primarily to one of two forms: inflammatory and non-inflammatory based on the extent to which, redness, swelling, warmth and pain are associated with the process. We know that the inflammatory cascade is actually involved in both forms, but the extent and nature of this involvement are so different that the utility of this construct is maintained. Osteoarthritis (OA) is the archetype of non-inflammatory arthritis and recommendations for treatment span a large spectrum and include patient-initiated approaches (e.g. exercise to strengthen muscles and weight reduction), use of appliances (splints, braces, and other assistive devices), medications, and ultimately, surgical procedures.1,2 Pharmacologic approaches have generally been disappointing, as their associated benefits are small and their lifelong risks are significant. It has been estimated that only 15%–20% of patients continue on the same medication even just one year later because of loss of efficacy or development of toxicity. 3 Mortality attributed to use of non-steroidal anti-inflammatory drugs (NSAIDs) has been reported to exceed that of melanoma and asthma. 4 Because much of the mortality is related to gastrointestinal (GI) bleeding, it was anticipated that selective inhibition of COX-2 would reduce toxicity. Celecoxib was designed to take advantage of this hypothesis. This review will consider the extent to which celecoxib has fulfilled that promise and what its current role in non-inflammatory arthritis should be.
Pharmacology
Mechanism of action
The enzyme cyclo-oxygenase (COX) exists as at least two isoforms, known as COX-1 and COX-2. While COX-1 synthesizes prostaglandins that are involved in the regulation of normal cell activities, COX-2 appears to produce prostaglandins principally involved in inflammation. 5 COX-1 is present at highest concentrations in the gastric mucosa, kidney and platelets, whereas COX-2 is constitutively expressed in the CNS, the juxtaglomerular apparatus of the kidney and in the placenta during late gestation. Both isoforms contribute to the inflammatory process, but COX-2 is induced during acute and chronic inflammation. When used at conventional dosages, traditional non-steroidal anti-inflammatory drugs (NSAIDs) inhibit both isoforms to a similar extent unlike the selective inhibition caused by celecoxib. 6
Disruption of COX-1 enzymatic activity by NSAIDs interferes with platelet function and intrinsic gastroprotection, predisposing a patient to GI bleeding, ulceration and perforation. The development of COX-2-selective inhibitors, including celecoxib, was driven by the desire to to relieve pain and other symptoms caused by inflammation, while reducing the risk of severe GI complications. 7 However, other complications of NSAID use, such as worsened congestive heart failure or renal dysfunction occur at the same rate with selective agents as with traditional NSAIDs. 6
While the principal mechanism of celecoxib is to selectively inhibit COX-2, other mechanisms may contribute to the drug's actions as well. Thus far, increased synovial fibroblast apoptosis, 8 regulation of transcription factors, 9 increased matrix production of hyaluronic acid and proteoglycans,10,11 and inhibition of p38 MAP kinase9,12 have all been demonstrated in association with the action of celecoxib in model systems. The extent to which these additional mechanisms may be involved when treating the pain of OA remains unknown.
Metabolism
Celecoxib, which is given orally, results in peak plasma drug concentration within 2 to 4 hours. It is extensively protein bound, especially by albumin, and has an apparent volume of distribution of about 450 L. The area under the plasma concentration-time curve (AUC) of celecoxib increases in proportion to ingested dose for dosages between 100 and 800 mg. Celecoxib is metabolized primarily by the cytochrome P450 (CYP) 2C9 isoenzyme and has an elimination half-life of about 11 hours. It is transformed to carboxylic acid and glucuronide metabolites that are subsequently excreted in urine and feces. 13 Less than 2% of celecoxib is eliminated unchanged in the urine. Plasma concentrations (AUC) of celecoxib are 43% lower in patients with chronic renal insufficiency (glomerular filtration rate 2.1 to 3.6 L/h (35 to 60 ml/min)) as compared to individuals with healthy renal function. 14 Steady-state AUC is increased by approximately 40% and180% in patients with mild and moderate hepatic impairment, respectively. 15
Celecoxib does not appear to interact significantly with warfarin, ketoconazole or methotrexate, but clinically significant drug interactions with fluconazole and lithium have been documented and attention is recommended during the co-administration of other substrates or inhibitors of the CYP 2C9 system including the commonly used medications losartan, glipizide, sildenofil, and sertraline. 15
Safety
General
Celecoxib has shown good safety with minor adverse drug reactions (ADRs) such as headache, dyspepsia and diarrhea most commonly observed (Table 1). Hypertension, worsening of congestive heart failure and allergic reactions are also seen as referenced. 16 Serious events such as gastrointestinal bleeding, thrombosis and renal insufficiency are uncommon, 17 but have resulted in a black boxed warning in the US Physicians Desk Reference (PDR) and will be discussed in more detail below.
Safety of celecoxib.
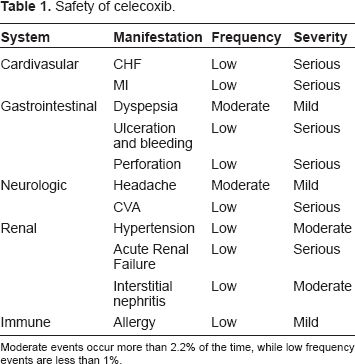
Moderate events occur more than 2.2% of the time, while low frequency events are less than 1%.
Gastrointestinal
Digestive tract adverse effects appear in 20% to 40% of the patients after a few weeks of treatment using anti-inflammatory doses of standard NSAIDs. Symptomatic gastroduodenal ulcers, bleeding, and perforations are the most serious, and the annual risk of death is estimated at 0.2%. 4 This can be reduced by use of selective COX-2 inhibitors including celecoxib. 18 This has been perhaps most convincingly shown in a very large 12 week trial of 13,274 osteoarthritis patients from 39 countries randomly assigned to double-blind treatment with celecoxib 100 or 200 mg BID, diclofenac 50 mg BID, or naproxen 500 mg BID. The nonselective NSAID group had more ulcers (0.8/100 patient-years) compared with the celecoxib group (0.1/100 patient-years) (odds ratio = 7.02; 95% confidence interval [CI], 1.46 to 33.80; P = 0.008) and there were fewer ulcer complications in the celecoxib group, both in patients taking aspirin and those not taking aspirin. It is important to note that the difference between the group taking celecoxib and those taking traditional NSAIDs reached statistical significance only when concomitant aspirin was not taken. 19 Other approaches to protect patients from GI complications using traditional NSAIDs in combination with misoprostil, H2-receptor blockade, or proton pump inhibitors (PPIs) are also effective.20,21
Renal
Both COX-1 and COX-2 are expressed in adult kidney tissues 22 and inhibition of these enzymes by NSAIDs is well-known to affect sodium and water handling, and to reduce glomerular filtration rate (GFR). This is also true for celecoxib. The GFR appears to be most sensitive to COX-1 inhibition; as in one report, elderly patients without co morbidities were able to take celecoxib with little effect on their GFR.23,24 Certainly, monitoring of kidney function and blood pressure appears prudent. Risk factors for renal complications including pre-existing renal disease, dehydration, diuretic or ACE use, and congestive heart failure 25 may raise the risk to as high to as high as 20% of patients being adversely affected. 26
Cardiovascular
Prior to the launch of selective COX-2 inhibitors, there were theoretic concerns about disrupting the balance of thrombosis and fibrinolysis by altering the ratio of prostacyclin to thromboxane. 27 The first reports of COX-2 associated thrombosis were in connective tissue disease patients 28 who arguably had additional risk factors. Although no specific mechanism of predisposition has been conclusively identified, thrombotic events as a consequence of this association ultimately resulted in the removal of medications from the US market in 2005. Some of the largest number of patients treated for OA with celecoxib and analyzed for these events are those in the Therapeutic Arthritis Research and Gastrointestinal Even trial (TARGET) and in the Glucosamine and chondroitin sulfate in Arthritis Intervention Trial (GAIT), each of which followed celecoxib treated patients from 6 months to 2 years. In each of these populations, no increase in cardiovascular outcomes was observed.29,30 Another recent report also examines cardiovascular outcomes in patients treated with naproxen or celecoxib for Alzheimer's disease. This study stopped enrollment secondary to the reported issues in the APC trial. Interestingly, the hazard ratio was 1.10 for vascular endpoints as compared to 1.63 for naproxen. 31
Black Box warning discussion
The US Physicians Desk Reference lists black box warnings for celecoxib in two areas. First is cardiovascular outcomes which may include increased risk for serious or fatal myocardial infarcts and other thrombotic events that may increase with duration of therapy. Usage in coronary artery bypass graft (CABG) peri-operative pain is contra-indicated. A second warning relates to gastrointestinal bleeding with bleeding, ulceration and perforation specifically listed as well as an increased risk to the elderly. 32
Guidelines
In 2007, the Osteoarthritis Research Society International (OARSI) Treatment Guidelines Committee undertook a critical appraisal of published guidelines for the treatment of OA. Agreement (%) was estimated and the best level of evidence to support each recommendation was extracted.
To date, 23 guidelines have been developed for the treatment of hip and/or knee OA, based on available evidence, author opinion, or both. Twenty (of 51) therapeutic modalities were universally recommended by these guidelines. As a group, NSAIDs were considered effective, though with a modest summary effect size (ES 0.32, 95% CI 0.24–0.39). 2 Specific ES for pain of OA treated with celecoxib were not discussed.
Studies of Clinical Efficacy in Osteoarthritis
Vs acetaminophen
Acetaminophen (paracetamol) is universally recommended as the initial pharmacological treatment for knee or hip osteoarthritis.1,2,33 Two randomized, double blind, placebo controlled, crossover multicenter clinical trials reported in 2004, the “Patient Preference for Placebo, Acetaminophen or Celecoxib Efficacy Studies”(PACES) showed that celecoxib was more efficacious than either placebo or acetaminophen. 34
Vs NSAID
In 2001, several studies were published in which celecoxib was compared to other NSAIDs. First, in a trial involving patients with osteoarthritis of the knee, celecoxib, at doses of either 100 or 200 mg once daily were shown to be as effective as naproxen 500 mg twice daily, considering both pain relief and improvement in physical function as outcome measures. These benefits were observed for up 24 weeks. 35 Second, in another study involving patients with knee osteoarthritis, celecoxib 100 mg BID was compared to diclofenac 50 mg TID or placebo for 6 weeks in a multicenter, randomized controlled trial. Celecoxib was found to be as effective as diclofenac. 36 Third, in an additional multicenter, randomized trial comparing the efficacy and safety of celecoxib, naproxen, and placebo in patients with OA of the hip, celecoxib 200 mg daily was as effective as naproxen 500 mg bid in reducing pain associated with OA of the hip. 37 Finally, an examination of the data from the subset of 768 elderly patients (70 years of age or older) who had participated in one of these three studies was also published in 2001; this report addressed functional status and health-related quality of life (HRQOL), as measured using the Short Form-36. In this analysis celecoxib and naproxen both improved functional status and HRQOL significantly and to a comparable degree. 38
Dosage interval
In 2000, a multicenter randomized parallel trial involving 686 patients compared the efficacy of celecoxib 200 mg once daily with 100 mg twice daily. 39 Arthritis assessments were performed at baseline and at weeks 2 and 6, or at early termination. In all measurements of efficacy, at all assessments, results were statistically indistinguishable between these two dosing schedules; no differences in safety were reported either. The authors concluded that either regimen would be an appropriate option for patients and physicians to consider using.
Radiographic progression
In addition to patient-centered outcome measures (e.g. decreased pain, improved function), radiographic data are increasingly used as endpoints to support claims of safety and efficacy. One such study was reported in 2002, in which radiographs of the hip or the knee obtained from patients with OA were reviewed. These patients had participated in trials in which they had received celecoxib at doses ranging from 200–400 mg daily; radiographs taken before exposure to the drug were compared with those taken 12 months later. No radiographic evidence of disease progression that could be attributed to celecoxib exposure was observed, leading the authors to conclude that long-term therapy with celecoxib does not accelerate OA progression in these joints. 40 This was shown to be true for the knee as well by GAIT. 41
Cost Effectiveness
A 2003 Canadian study of cost effectiveness used a 5-year Markov model to compare celecoxib with ibuprofen and diclofenac (34). Incremental cost-effectiveness ratios were calculated for cases considered to be at average risk of upper gastrointestinal (UGI) events and also for those at high-risk–-defined as those with a prior history of a UGI event. Subjects were cases with OA or rheumatoid arthritis (RA) where a decision had been made to treat with NSAIDs but who did not require therapy with low-dose aspirin. Main endpoints were the proportion of cases predicted to experience clinical or complicated UGI events, quality-adjusted life expectancy (QALY), and life expectancy. For cases of average risk for adverse events, diclofenac was more cost-effective than celecoxib. However, for high-risk cases celecoxib was more cost-effective than diclofenac, and using a threshold of can $50,000 per QALY gained, celecoxib would be cost-effective in patients over the age of 81, provided that no additional risk factors, for bleeding including the use of low-dose aspirin, were present. Co-prescription of proton-pump inhibitors with COX-2 NSAIDs is not cost-effective for patients at high risk. 42
Another study involving economic outcomes was reported in 2007 (35). This project used modeling informed by societal perspectives over patients’ lifetimes, to compare the cost-effectiveness of celecoxib with traditional NSAIDs for the treatment of OA beginning at age 60, in patients with an an average risk for developing UGI complications. At baseline, the model predicted an incremental cost-effectiveness ratio (ICER) of $31,000 per QALY for celecoxib versus traditional NSAIDs; this improved to $19,300 per QALY when the model was adjusted to consider the increased risk of UGI complications associated with with advancing age, and increased further to $17,100 in sensitivity analyses in which serious cardiovascular and cerebrovascular events, also associated with increasing age, were included.
Role in Patients with Concurrent Need for Anticoagulaton
One of the patient groups most challenging to treat are those with OA and a need for chronic anti-coagulation. There are several mechanisms by which NSAIDs increase the risk for UGI bleeding; the anti-platelet effects of NSAIDs compound these, and in the setting of chronic anticoagulation by factor inhibition (e.g. with warfarin) can create a “perfect storm” for severe, UGI complications. Because selective inhibitors such as celecoxib do not have a significant anti-platelet activity, they offer less risk for patients who are anticoagulated, though this is not to say that there is consensus that celecoxib is safe in this setting. Reports have noted interaction of celecoxib with warfarin as dose changes are made. 43
Patient Preference
Patient preference in treating the pain of OA is difficult to systematize. Most people prefer a lower frequency of medication use or application, most want oral medications instead of injections or topical application. Celecoxib is given as a daily oral medication, is well tolerated and has sustained effects making it a good match for most patients. Taking the above data together, celecoxib should be considered to have equivalent efficacy for OA to traditional NSAIDs. It should also have an improved GI safety profile and a caution regarding cardiovascular events. Balancing these small differences is the mutual job of the provider and patient together. One possible approach to considering options is presented in Figure 1; this can also serve as a pathway to discussions with the patient. In a way, a consideration of the possible risks and benefits of therapy can be broken down from what initially may seem overwhelming into smaller steps that may invite patients to ask further questions, or to help us better understand their priorities. While reaching agreement on a therapeutic strategy through shared decision-making is important; ultimately, providers bear the responsibility for prescribing.
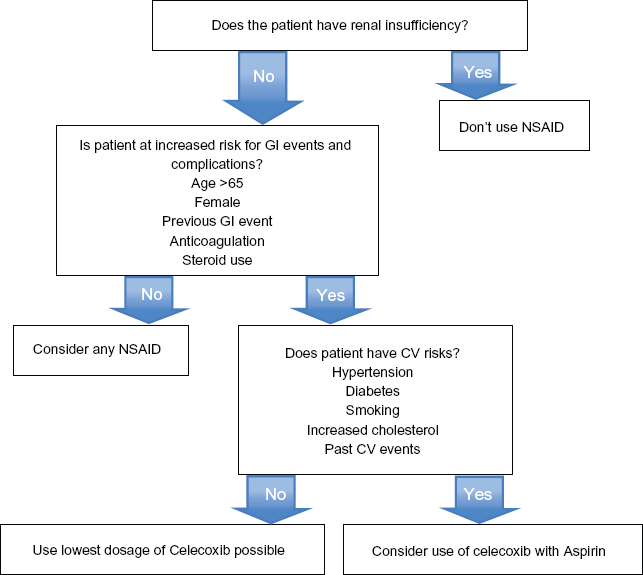
An approach to guide risk assessment prior to prescribing celecoxib for arthritis pain.
Conclusions
As with any other therapeutic decision, the choice to use celecoxib (or any other NSAID) for symptom-management is fundamentally a risk-management assessment. Both risk and benefit can be envisioned, and to some degree, quantified, from clinical studies and post-marketing data. However, accurately predicting the experience of an individual patient remains challenging. For this reason, interventions that present essentially no risk (for example, patient education regarding self-management strategies) are attractive even if their benefit may be small. Reasonable management of arthritis symptoms involves multiple concurrent efforts, addressing lifestyle factors (e.g. effectively communicating the importance of a healthy diet, regular exercise, optimal weight management, psychosocial well-being, etc.), the use of non-pharmacologic (physical therapy, assistive devices), and–-for some patients–-medications and eventually, joint replacement surgery. Hard and fast rules are of limited use because of the multiple factors involved. Ultimately, education regarding the expected benefits and risks of each approach is the responsibility of the provider.
Compared with the benefits of disease-modifying anti-rheumatic drugs for patients with RA, medications have not been shown to be nearly as effective in altering the course of OA. Nevertheless, despite the potential for toxicity, NSAIDs are often used because they can offer clinically important improvements in the quality of patients’ lives, in their ability to function, and in the degree of pain they experience.
For patients in whom NSAID therapy is planned, the risk of GI toxicity needs be considered. For patients who are elderly, have a history of NSAID-related dyspepsia, gastritis, esophagitis, or ulcers, or who are anticoagulated, celecoxib may be preferred. In addition, if patients have NSAID-sensitive asthma, selective COX-2 inhibitors such as celecoxib can be considered, as these have not been shown to cause exacerbations. In contrast, celecoxib is not recommended for women desiring pregnancy, especially because the risk of a teratogenic effect has not been excluded and selective COX-2 inhibitors are not currently approved for children or as therapy for ENT disease. 44
Disclosures
This manuscript has been read and approved by all authors. This paper is unique and is not under consideration by any other publication and has not been published elsewhere. The authors report no conflicts of interest.