
Abstract
Antiplatelet therapy is the cornerstone in the modern therapy of patients with acute coronary syndromes (ACS), because of the unique role of platelets in coronary thrombosis. Clopidogrel in combination with aspirin is the current “gold standard” for reducing cardiovascular events in such patients, providing a synergistic platelet inhibition through different platelet activation pathways. Clopidogrel is a thienopyridine which inhibits ADP-induced platelet aggregation, with no direct effects on the metabolism of arachidonic acid. Due to a better safety profile with a similar antiplatelet effectiveness, it is preferred to ticlopidine. In patients with ACS without ST segment elevation (NSTEMI), clopidogrel plus aspirin is able to reduce the relative risk of adverse cardiovascular events by 20%, compared with aspirin alone. Clopidogrel plays a key role also in patients undergoing coronary stenting, in order to prevent stent thrombosis. Pretreatment and long-term treatment with clopidogrel reduces by about one-third the risk of cardiovascular death or myocardial infarction in NSTEMI ACS patients undergoing percutaneous coronary angioplasty (PCI). However, a long-term dual antiplatelet therapy is associated with a higher rate of bleeding events. Clinical practice guidelines currently recommend long-term dual antiplatelet therapy with aspirin and clopidogrel in patients with ACS and a pre-treatment with clopidogrel in every patient scheduled for PCI. The concept of clopidogrel resistance and the need for a pretreatment in patients undergoing coronary stent implantation led to the concept that an improved antiplatelet regimen with novel drugs is desirable.
Introduction
Acute coronary syndromes (ACS) represent a life-threatening manifestation of atherosclerosis. It is usually precipitated by acute thrombosis, induced by a ruptured or eroded atherosclerotic plaque, with or without concomitant vasoconstriction, causing a critical reduction in coronary blood flow. 1
The plaque prone to instability are those with a large lipidic core, a high concentration of inflammatory cells, a low density of smooth muscle cells, and a thin fibrous cap. 2 Thrombosis plays a key role in the development of ACS. This has been widely demonstrated by autoptic data and angiographic detection of thrombi at the site of the culprit lesion.3–5 In both plaque rupture and erosion, the lipid-rich core exposed is highly thrombogenic and has a high concentration of tissue factor. 6 In the case of erosion, the thrombus adheres to the surface of the plaque, whereas when rupture occurs, the thrombus involves the deeper layers down to the lipid core. As a consequence, the plaque has a rapid growth and progression, if the thrombus is not accommodated by a positive remodelling, thus leading to a sudden change in the severity of the stenosis. 1
The thrombus is fibrin-rich and totally occlusive in patients with ST elevation myocardial infarction (STEMI), whereas it is platelet-rich and partially or intermittent occlusive in patients with non-ST elevation myocardial infarction (NSTEMI). 1 Thus, platelet activation and aggregation which are crucial in the transformation of a stable atherosclerotic plaque to an unstable lesion, play a key role in the setting of ACS.
Antiplatelet therapy is essential to the treatment of patients with ACS and aspirin still represents a cornerstone in the modern therapy of these patients. 7 Because of the unique role of platelets in coronary thrombosis, the need for inhibition of other platelet activation pathways has led to the development of various other antiplatelet drugs, such as clopidogrel. 8 Clopidogrel in combination with aspirin is the current “gold standard” for reducing cardiovascular events in such patients. 9
Mechanism of Action, Metabolism and Pharmacokinetic Profile of Clopidogrel and Ticlopidine
Clopidogrel and ticlopidine are structurally related thienopyridines with platelet inhibitory properties. Both drugs inhibit ADP-induced platelet aggregation, with no direct effects on the metabolism of arachidonic acid. 10 Clopidogrel and ticlopidine also can inhibit platelet aggregation induced by collagen and thrombin, but these inhibitory effects likely reflect blockade of ADP-mediated amplification of the response to other antagonists. It has been demonstrated that in vivo hepatic transformation to an active metabolite is necessary for their antiplatelet effects and a short-lived, active metabolite of clopidogrel has been characterized.
Clopidogrel induces irreversible modifications of the platelet ADP receptor PY12 mediating inhibition of stimulated adenylyl cyclase activity by ADP. 11 The permanent alteration of the ADP receptors is consistent with time-dependent, cumulative inhibition of ADP-induced platelet aggregation on repeated daily dosing and with slow recovery of platelet function on drug withdrawal. 12
Experimental studies on healthy volunteers showed an ADP-induced platelet aggregation by clopidogrel ranging from 40% to 60%. This steady state is reached in 4 or 7 days with repeated daily dosing of 50 to 100 mg. 10 Ticlopidine induces a similar maximal inhibition at a dosage of 500 mg daily, but has a slower onset of antiplatelet effect compared with clopidogrel. Clopidogrel pharmacodynamic pattern is quite similar to that of aspirin, with a cumulative platelet inhibition on repeated daily low-dose administration and a normalization of platelet function after 7 days from the last dose. 12
Comparison between Clopidogrel and Ticlopidine
The majority of the trials and registries of comparison between clopidogrel and ticlopidine found a reduction in the 30-day rate of major adverse cardiac events (MACE), as defined by each trial, with clopidogrel versus ticlopidine. Overall, the pooled data from 13955 patients showed an odd ratio (OR) of 0.51 in favor of clopidogrel (95% CI 0.42 to 0.63). 13 This 50% risk reduction in the MACE rate in those patients receiving clopidogrel plus aspirin versus ticlopidine plus aspirin (2.10% vs. 4.04%) was statistically significant (p = 0.001). The reduction in the MACE rate was seen in both the randomized clinical trial and the registry data, but was only substantial and statistically significant in the registries. The OR in favor of clopidogrel in the randomized clinical trials was 0.90 (95% CI 0.57 to 1.44). The OR in favor of clopidogrel in the larger numbers of patients in the registries was 0.45 (95% CI 0.36 to 0.57, p = 0.001).
However, the use of ticlopidine was sometimes limited to only two weeks after coronary artery stenting, whereas clopidogrel was often used for four weeks, perhaps providing further protection against ischemic events.
Moreover, the beneficial effect of clopidogrel observed in this analysis may be due to the more rapid onset of an antiplatelet effect seen with the loading dose of clopidogrel used in most of these studies, or to better patient compliance with clopidogrel therapy. Based on this data set of almost 14000 patients, it can be reasonably concluded that clopidogrel plus aspirin is at least as effective as ticlopidine plus aspirin in reducing adverse ischemic events, and, in fact, in addition to its known better safety profile, clopidogrel appears to be more efficacious than ticlopidine. 13
Due to a better safety profile, clopidogrel has almost displaced ticlopidine in the daily clinical practice.
Clinical use in ACS
Antiplatelet therapy with aspirin was shown to safely reduce adverse cardiovascular events in high-risk patients.14,15 However, there was still a substantial risk of death from cardiovascular events, reinfarction and ischaemia in ACS patients routinely treated with aspirin, in both the short and long term follow-up. 16
Synergistic platelet inhibition through different platelet activation pathways, by clopidogrel and aspirin, represents a key strategy in current ACS treatment. 17
The rationale for the use of clopidogrel in ACS has been assessed in several trials (Table 1). The CAPRIE trial was the first randomised, blinded, international trial designed to assess the relative efficacy of clopidogrel (75 mg once daily) and aspirin (325 mg once daily) in reducing the risk of a composite outcome cluster of ischaemic stroke, myocardial infarction, or vascular death. 18 Their relative safety was also assessed. The population studied (19185 patients) comprised subgroups of patients with atherosclerotic vascular disease manifested as either recent ischaemic stroke, recent myocardial infarction, or symptomatic peripheral arterial disease. Patients were followed for 1 to 3 years. Compared with aspirin, clopidogrel was shown to provide a relative risk reduction of 8.7% [absolute risk reduction,0.5% (NNT (number needed to treat) = 200); p = 0.043]. This benefit extended beyond the 25% relative risk reduction provided by aspirin, and was associated with fewer bleeding complications during a follow-up period of 1.91 years. 18 The efficacy results from CAPRIE were consistent with the previous findings with ticlopidine and indicated that thienopyridines are at least as effective as aspirin in patients with atherothrombotic disease, confirming the importance of the ADP pathway, compared with the thromboxane pathway, in this disease.
Clopidogrel trials.
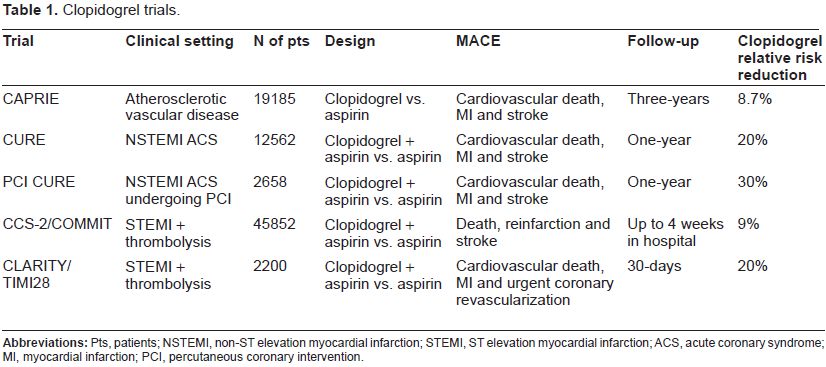
The CURE trial addressed the efficacy of dual antiplatelet therapy with aspirin and clopidogrel in 12562 patients with ACS without ST segment elevation. 19 Early and intermediate-term (9 months–1 year) use of clopidogrel (300 mg loading dose, then 75 mg/day for a mean duration of 9 months) plus aspirin was shown being able to reduce the relative risk of death from cardiovascular causes, non-fatal myocardial infarction or stroke by 20% (p < 0.001) compared with aspirin alone, the first primary outcome, a composite end-point, occurring in 9.3 percent of the patients in the clopidogrel group and 11.4 percent of the patients in the placebo group. 19 However, although the individual end points of death, myocardial infarction and stroke all showed numerical improvement with clopidogrel, the differences were not statistically significant for death and stroke. 20 The reduction in the primary end point was driven by a 1.5% absolute reduction in the rate of subsequent nonfatal myocardial infarction. 19 CURE used a definition of myocardial infarction, which included patients with only elevated serum troponin levels. Therefore, an elevation of serum troponin even in the absence of an elevation in creatinine kinase levels was considered sufficient to meet the myocardial infarction end point. This was in direct contrast with other ACS trials, which used more restrictive definitions requiring elevations in creatinine kinase or its MB isoform.21–25
Although several studies had demonstrated the efficacy of clopidogrel in reducing ischaemic events in a number of settings, its role in STEMI patients remained undefined until the results of the COMMIT and CLARITY-TIMI 28 trials were published in 2005.26,27
The Clopidogrel and Metoprolol in Myocardial Infarction Trial/Second Chinese Cardiac Study (COMMIT/CCS-2) was a highly powered, randomised, double-blind, placebo-controlled trial of 45852 patients with acute myocardial infarction. 26 The objectives of the antiplatelet arm of the trial were to investigate whether adding clopidogrel (75 mg/day) to aspirin and standard fibrinolytic and anticoagulant therapy would further reduce the composite risk of death, recurrent myocardial infarction or stroke, or improve mortality, compared with placebo. 26 About 55% of patients received fibrinolytic drugs (typically urokinase), which may not be comparable with the rate of thrombolysis in other Western countries. The average time from symptom onset to presentation was just over 10 hours, and the mean treatment duration was 15 days. The COMMIT study results showed that the addition of clopidogrel to aspirin significantly reduced the relative risk of in-hospital death by 7% [absolute risk reduction,0.6% (NNT = 167); p = 0.03] and the risk of composite cardiovascular events (death, reinfarction or stroke) by about 10% [absolute risk reduction,0.9% (NNT = 111); p = 0.002]. No loading dose was given to patients in the COMMIT study because of concerns about potential bleeding complications. 26
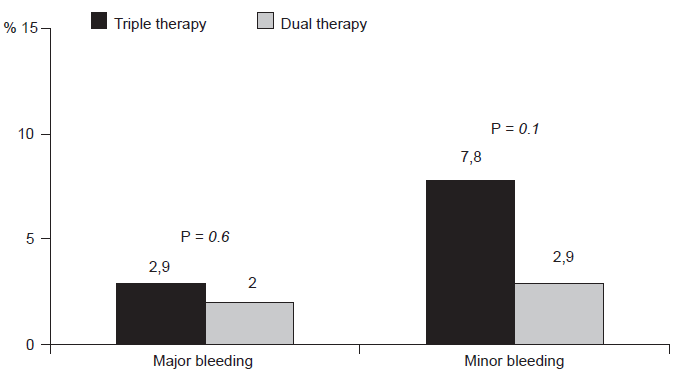
Major and minor bleeds at 18-month follow-up in patients on dual antiplatelet therapy vs. patients on triple therapy with aspirin, clopidogrel and oral anticoagulation. Bleeding events are defined according to TIMI classification.
Clopidogrel as Adjunctive Reperfusion Therapy-Thrombolysis in Myocardial Infarction (CLARITY-TIMI 28) assessed whether the addition of clopidogrel was beneficial in STEMI patients who received a standard fibrinolytic regimen, including aspirin.27,28 Patients (n = 3491) were randomised to receive either clopidogrel (300 mg loading dose followed by 75 mg once daily) or placebo in a doubleblind setting. Treatment with clopidogrel resulted in a 36% relative reduction [absolute risk reduction,6.7% (NNT = 15); p < 0.001] in the composite odds of an occluded infarct-related artery on the predischarge angiogram or death or recurrent MI by the time of angiography. This benefit was consistent across a broad range of subgroups. At 30 days, clopidogrel therapy led to a significant 20% relative reduction in the odds of death from cardiovascular causes, recurrent myocardial infarction or ischaemia leading to the need for urgent revascularisation (p = 0.03). In a subgroup analysis, pretreatment with clopidogrel for 2-8 days (with an average of 3 days) significantly reduced the odds of cardiovascular death, reinfarction or stroke by 46% before and within 30 days following PCI, irrespective of the timing of PCI relative to randomisation.
Clinical practice guidelines currently endorse the use of clopidogrel in all non-ST elevation ACS patients irrespective of whether they undergo an early invasive or early conservative strategy, and in all ST-elevation myocardial infarction patients regardless of the mode of reperfusion therapy.29–31 It is not clear to what extent these evidence-based recommendations are followed in the “real-world” management of ACS. 32
Clopidogrel and PCI
Mechanical coronary reperfusion with PCI is the gold standard in the therapy of ACS. Dual antiplatelet therapy with aspirin and a thienopyridine is mandatory after stent implantation, in order to prevent stent thrombosis. 32 After the implantation of a bare metal stent, 4 weeks of dual antiplatelet therapy is necessary, whereas for drug eluting stents such therapy has to be prolonged up to one year. 32 Indeed, clopidogrel plus aspirin treatment (4 weeks) has become standard care for preventing stent thrombosis in patients who received stents implantation.33–36 The PCI-CURE trial results demonstrated that extending clopidogrel use to include pretreatment and long-term treatment (mean 8 months) in NSTEMI ACS patients (n = 2658) undergoing PCI reduced the risk of cardiovascular death or myocardial infarction by about one-third. 37
The beneficial effects of pretreatment with a thienopyridine before PCI have been reported in several studies, although none were randomized comparisons.38,39 In the PCI-CURE analysis, all patients in the aspirin and clopidogrel arm had been pretreated with clopidogrel for a median of 10 days, whereas the majority of patients in the aspirin and placebo arm received no pretreatment, although 25% did receive an open-label thienopyridine before PCI. 37 The frequency of death or MI in the 30 days after PCI was significantly less among patients who had been pretreated than in those who had not (4.4% versus 2.8%, a relative risk reduction of 34%; P = 0.04). 40 These findings corroborated the results of the prospective, randomised, placebo-controlled Clopidogrel for the Reduction of Events During Observation trial (CREDO), which examined the duration of pre-treatment with clopidogrel as a continuous variable to identify the optimal duration of pre-treatment in 1762 patients undergoing PCI. 41 The difference in outcomes between placebo and clopidogrel pre-treated patients was not significant until ≥15 h pre-treatment, with a 58.8% (p = 0.028) reduction in the primary end point in patients pre-treated with clopidogrel ≥15 h compared with placebo. Longer durations of clopidogrel pre-treatment were associated with improved outcomes. The event rates diverged maximally at 24 hrs (optimal duration). Whether or not a patient received a GP IIb/IIIa blockers did not significantly influence the benefit of clopidogrel pre-treatment for >15 hrs.
Another study demonstrated that a pre-treatment with a 600-mg loading dose of clopidogrel 4 to 8 hours before PCI is safe, and significantly reduced periprocedural myocardial infarction as compared with the conventional 300-mg dose. 42
A recent extension of the CLARITY-TIMI 28 study has shown that it is feasible to treat patients with ST elevation myocardial infarction with fibrinolytic agents, heparin, aspirin and clopidogrel in medically-equipped ambulances without an increase in major bleeding complications. 43 Preliminary results indicate that prehospital administration of clopidogrel significantly reduced the risk of an occluded infarct artery (TIMI flow grade 0/1), death and reinfarction prior to angiography. 16 The benefit of clopidogrel pretreatment in the PCI-CLARITY study was consistently maintained across pretreatment periods ranging from 6 h to 8 days, suggesting that even brief periods of pretreatment with clopidogrel before PCI improved patient outcomes. 16 The event curves for the study and control groups continued to diverge following PCI, suggesting that the benefit of clopidogrel pretreatment may extend beyond the prevention of platelet aggregation during the procedure. 16
Clinical practice guidelines currently recommend pre-treatment with clopidogrel in every patient scheduled for PCI, regardless of whether stent implantation is intended or not. A pre-treatment with 300 mg within 2.5 h, however, may not be sufficient. To ensure full antiplatelet activity, clopidogrel should be initiated at least 6 h prior to the procedure with a loading dose of 300 mg, ideally administered the day before a planned PCI. If this is not possible, a loading dose of 600 mg should be administrated at least 2 h before PCI. Patients unable to be pre-treated with clopidogrel should receive the (possibly higher) loading dose immediately following the procedure. 44
In patients with unstable angina or non ST elevation ACS today's preference for an early invasive strategy combined with stent and GP IIb/IIIa inhibitors lowers the likelihood of urgent bypass surgery for the majority of these high risk patients. On the basis of the very early positive effect of clopidogrel the guidelines of the European Society of Cardiology recommend initiating clopidogrel administration as soon as possible, if clinically justifiable. 44
With primary PCI and stenting in patients with ST elevation myocardial infarction, clopidogrel should be administered in these patients, preferentially with a loading dose of 600 mg. Regarding the duration of clopidogrel prescription, the results from non ST elevation ACS may be extrapolated to ST elevation ACS, but this has yet to be scientifically proven. 44
Bleeding Complications
Dual antiplatelet therapy is associated with a higher risk of bleeding. Moreover, a bleeding event is even more difficult to manage, due to the impossibility to neutralize the clopidogrel effect. A bleeding event can dramatically condition patient prognosis. In a meta-analysis of the OASIS and CURE randomised trials (N = 34,146), mortality rates at 30 days were significantly higher in ACS patients who had a major bleeding event compared with those who did not. 45
In the CURE trial, major bleeding was significantly more common in the clopidogrel group (3.7 percent in the clopidogrel group as compared with 2.7 percent in the placebo group; relative risk, 1.38; 95 percent confidence interval, 1.13 to 1.67; P = 0.001). There were 135 patients with life-threatening bleeding episodes in the clopidogrel group (2.2 percent) as compared with 112 in the placebo group (1.8 percent; relative risk, 1.21; 95 percent confidence interval, 0.95 to 1.56). There was no excess rate of fatal bleeding, bleeding requiring surgical intervention, or hemorrhagic stroke. The excess of major bleeding episodes were gastrointestinal hemorrhages and bleeding at the sites of arterial punctures. 19
Although CURE showed no significant excess of major bleeding after coronary artery bypass grafting (CABG), patients had clopidogrel withheld for a median of five days before surgery. 21 Among patients in the CURE trial who stopped clopidogrel less than five days before CABG, the incidence of major bleeding increased by an absolute rate of 3.3%.
Overall, the risk of minor bleeding was significantly higher in the clopidogrel group than in the placebo group (322 [5.1 percent] vs. 153 [2.4 percent]; P < 0.001). 19
In the COMMIT trial, no apparent increase in major bleeding emerged, even when clopidogrel was administered with fibrinolytic agents or to older patients. However, no loading dose was given to patients. 26
Also in the CLARITY-TIMI 28 trial treatment with clopidogrel was not associated with an increased rate of major bleeding or intracranial haemorrhage.
However, only a subgroup of patients was pretreated with a loading dose.16,27
The potential for developing bleeding complications is further enhanced in patients also requiring oral anticoagulant treatment (“triple therapy”). A recent study assessed long-term outcomes associated with the use of triple-therapy in patients undergoing coronary stenting and evaluated how these could be affected by targeting international normalized ratio (INR) values to the lower therapeutic range. 46 One hundred and two consecutive patients undergoing coronary stenting treated with dual antiplatelet therapy with aspirin and clopidogrel also requiring oral anticoagulation were studied. Most patients (78.4%) undergoing PCI presented with an ACS. INR was targeted to the lower therapeutic range (2.0-2.5). Patients were followed for 18 months and bleeding, with a mean duration of triple therapy of 157 ± 134 days. Outcomes were compared with a control group (n = 102) treated only with dual antiplatelet therapy, who did not require oral anticoagulant therapy. At 18-months, a non-significant increase in bleeding was observed in the triple versus dual therapy group (10.8% vs. 4.9%; p = 0.1; Fig. 1). INR values were higher in patients with bleeding (2.8 ± 1.1 vs. 2.3 ± 0.2; p = 0.0001). In patients with INR values within the recommended target (79.4%), the risk of bleeding was significantly lower compared to patients who did not (4.9 vs. 33%; p = 0.00019) and comparable to that observed in the control group (4.9%). An INR > 2.6 was the only independent predictor of bleeding. There were no significant differences in MACE between groups (5.8% vs. 4.9%; p = 0.7). 46
Safety
The overall tolerability of clopidogrel in CAPRIE trial was similar to that of aspirin regardless of age, gender and race, with an approximately equal incidence (13%) of patients withdrawing from treatment because of adverse reactions. 18 The frequency of severe rash was higher with clopidogrel than with aspirin (p = 0.017) as was the frequency of severe diarrhea (p = 0.080). More frequent with aspirin were severe upper gastrointestinal discomfort (p = 0.096), intracranial hemorrhage (p = 0.23), and gastrointestinal hemorrhage (p = 0.05). 18
Clopidogrel has been evaluated for safety in more than 17500 patients, including over 9000 patients treated for 1 year or more and showed a significantly better safety profile than ticlopidine.
Severe neutropenia (less than 450 neutrophils/mcL) has occurred in approximately 4/10000 patients, whereas ticlopidine is associated with a 0.8% rate of severe neutropenia. 18
Although the risk of myelosuppression appears to be quite low, it is recommended in cases of fever or other signs of infection that possible neutropenia be evaluated. 18
Few cases of thrombotic thrombocytopenic purpura (TTP) developed during or soon after treatment with clopidogrel have been reported, not emerging from clinical trials, whereas ticlopidine has an estimated incidence of TTP of 1 case per 1600 to 5000 patients treated.47–50
TTP is a life-threatening, multisystem disease, characterized by intravascular aggregation, thrombocytopenia, hemolytic anemia, fever, neurologic changes and renal abnormalities, fatal in 10% to 50% of patients depending on how rapidly plasmapheresis is initiated.
The development of cardiac or neurologic changes after the initiation of clopidogrel therapy may be mistakenly attributed to the underlying condition for which it was prescribed. Physicians should be aware of the possibility of thrombotic thrombocytopenic purpura among patients who are receiving clopidogrel. 51
Clopidogrel Resistance
The emergence of the phenomenon of clopidogrel non-responsiveness, the so-called situations of ‘clopidogrel resistance’, has received the concerns of clinicians.52–55 Decreased responsiveness to the antiplatelet effects of clopidogrel has been reported. Five to 10% of patients treated with clopidogrel are resistant to its effects as assessed by standard platelet assays, and as many as 25% are only partially responsive. 56 Marked inter-individual response to clopidogrel administration exists regardless of the loading dose. However increasing the loading dose to 600 mg shortens the time and increases the magnitude of maximal inhibition compared to the approved 300-mg loading dose. 57
The phenomena of such antiplatelet therapy ‘resistance’ are of great clinical significance. In the CURE trial, although dual antiplatelet therapy conferred a sizable additional benefit over aspirin alone, 9%-10% of patients continued to experience ischemic events during the follow-up period. 19 Variability in individual responsiveness to oral antiplatelet therapy, including “resistance,” has been attributed to the occurrence of these events. 9 Previous studies demonstrated that laboratory clopidogrel nonresponsiveness could be found in approximately 20% of patients undergoing PCI and is associated with an increased risks of worsened cardiovascular outcomes. 58 Rapid and accurate diagnosis of antiplatelet resistance also remains an issue as new bedside tests are developed. Despite the variety of tests available, no consensus exists regarding the reference standard for measuring platelet activation, and definitions of aspirin and clopidogrel resistance differ, depending on which test is used. In addition laboratory threshold values for unsatisfactory platelet inhibition are often arbitrary determined. A recent prospective trial demonstrated that a low response to clopidogrel assessed with multiple electrode platelet aggregometry is significantly associated with an increased risk of stent thrombosis in patients undergoing drug-eluting stent implantation. 59
The precise cause(s) of such resistance is largely unknown, and various clinical, cellular and genetic factors can contribute to these phenomena. 8 Clopidogrel resistance can be attributable to various, biological, genetic and clinical factors, such as non-compliance or drug interactions. More recently, the CYP2C19*2 genetic variant was reported as a major determinant of prognosis in young patients receiving clopidogrel treatment after myocardial infarction, in a study of 259 young patients (aged < 45 years) who were exposed to clopidogrel treatment for at least a month. 60 Clinical factors indeed have a major role in variable response profiles to clopidogrel. 9 As with aspirin, failure to prescribe and poor compliance play a pivotal role. Certain clinical scenarios, such as diabetes, ACS, and elevated bodymass index, are also associated with reduced clopidogrel responsiveness. This may explain why such patients have a greater likelihood of developing recurrent thrombotic complications despite clopidogrel use. 9 The fraction of immature platelets is increased in acute coronary syndromes, especially in the acute phase of STEMI and can contribute to coronary thrombus formation. 61
Drug-drug interactions, including lipophilic statins and omeprazole, may also interfere with the pharmacodynamic effects of clopidogrel. 62 Some indirect evidence suggests that higher drug doses can be helpful in the management of clopidogrel resistance, but more information on the value of such an approach is required. 63 An ongoing trial is evaluating the efficacy and safety of a higher loading and initial maintenance dose of clopidogrel compared with the standard-dose regimen and high-dose of aspirin compared with low-dose of aspirin in patients with ST or non-ST-segment-elevation ACS managed with an early invasive strategy. 64 Another ongoing trial is also testing whether the rate of iscaemic events can be further reduced by tailoring the specific antithrombotic dose to individual patients by use of laboratory or point-of-cre testing. 65
Finally clinical trials are needed to define whether hyporespoders to clopidogrel are at increased risk for thrombotic events and whether hyper- responders are at increased risk for bleeding.
Novel P2Y12 Antagonists
Despite the widespread use of clopidogrel in patients undergoing PCI with currently available thienopyridines, several important issues remain.59,66 Data from the CREDO trial suggest that most of the acute effect seen in reducing periprocedural events with clopidogrel was limited to patients who received the drug at least 6 hours, and perhaps as many as 15 hours, before the procedure.42,67 In addition, a significant variability in the response to clopidogrel among healthy subjects and patients undergoing PCI has been observed, with some individuals having minimal inhibition of ADP-induced platelet aggregation.59,68,69 This concept of clopidogrel resistance led to the concern that some patients may not be adequately protected from the intense platelet activation and aggregation that occur with PCI and are therefore at increased risk for thrombotic events.59,70 Because of these issues, an improved antiplatelet regimen to support PCI is desirable.
Prasugrel (CS-747, LY640315) is a novel thienopyridine antiplatelet agent that has been shown in preclinical studies to be more potent and to have a more rapid onset of action than clopidogrel. Phase 1 studies in healthy human subjects not taking aspirin showed inhibition of platelet aggregation to be greater with a single 60-mg dose of prasugrel than a single 300-mg dose of clopidogrel and that repeated dosing with 10 mg prasugrel showed higher inhibition of platelet aggregation than 75 mg clopdogrel. Furthermore, there is evidence in healthy volunteers that thienopyridine resistance may be less frequent with a loading dose of 60 mg prasugrel than with 300 mg clopidogrel. 71 These features stimulated interest in the evaluation of prasugrel for the prevention of thrombotic events after PCI.
The JUMBO TIMI 26 trial was designed to evaluate ranges of both loading and maintenance doses of prasugrel compared with standard therapy with clopidogrel. In aggregate, these data showed that treatment with prasugrel resulted in acceptable levels of bleeding with contemporary PCI practices; there were low rates of major bleeding, significant (major plus minor) bleeding, and transfusions. 72
The Trial to Assess Improvement in Therapeutic Outcomes by Optimizing Platelet Inhibition with Prasugrel (TRITON-TIMI 38) was a large-scale multinational, randomized, phase 3 trial in which prasugrel was compared with clopidogrel in moderate- to high-risk patients with ACS who were already receiving aspirin. 73 The study goals were to test the hypothesis that higher and less variable inhibition of platelet aggregation would result in fewer clinical ischemic events and to evaluate the safety of a regimen that produced a higher inhibition of platelet aggregation. The protocol for TRITON-TIMI 38 adopted the standard 300-mg/75-mg/day dosing regimen for clopidogrel, and the 60-mg/10-mg/day regimen for prasugrel. A total of 13608 patients on an intent-to-treat basis who were scheduled for PCI were assigned to receive prasugrel or clopidogrel for up to 15 months. The primary end point of cardiovascular death, nonfatal myocardial infarction, or stroke was reached by 781 patients (12.1%) in the clopidogrel group and 643 patients (9.9%) in the prasugrel group (hazard ratio [HR], 0.81; 95% confidence interval [CI], 0.73-0.90; p = 0.0004), demonstrating a 19% relative risk reduction in favor of prasugrel.
Reduction in myocardial infarction was the principal factor in the difference in primary end points between the groups. Although the overall mortality did not differ significantly between the treatment groups, there were significant differences in the rate of bleeding events. Major bleeding occurred in 2.4% of prasugrel patients compared with 1.8% of patients in the clopidogrel group (HR, 1.32; 95% CI, 1.03-1.68; p = 0.03). There were significant differences in the rates of life-threatening bleeding (1.4% vs. 0.9%, p = 0.01) and fatal bleeding (0.4% vs. 0.1%, p = 0.002) and a trend in the rate of life-threatening but nonfatal bleeding (1.1% vs. 0.9%, p = not significant). 73
Ticagrelor (AZD6140) is the first oral, direct-acting, reversible P2Y12 inhibitor and has greater antiplatelet efficacy than clopidogrel. Phase 2 studies indicate that ticagrelor has a safety profile similar to that of clopidogrel. However, the prevalence of dyspnea and ventricular pauses was higher during ticagrelor therapy. In the DISPERSE-2 study, the prevalence of myocardial infarction was lower during therapy with ticagrelor than with clopidogrel, but the study was not powered to demonstrate superiority with respect to the occurrence of ischemic events. 74 The phase 3 PLATO trial will evaluate the clinical efficacy of ticagrelor compared with clopidogrel in patients with ACS. 75
Cangrelor is a potent intravenous direct platelet P2Y12 antagonist. Its onset of effect occurs in seconds, assuming a bolus dose is given, and it can inhibit up to 100% of ADP receptors. It has a predictable steady-state dose-effect relation, which, in the healthy human populations in which it has been studied, appears to be desirable. The drug has a short plasma half-life, clearance that is independent of renal or hepatic function with complete platelet recovery within one hour, and clinical effects similar to those of an intravenous glycoprotein IIb/IIIa inhibitor but with the potential for greater convenience and less bleeding. Recently, phase 3 trials in ACS patients (CHAMPION PCI and PLATFORM) have been prematurely stopped, since an interim analysis showed no superiority of cangrelor over standard therapy with clopidogrel.76,77
Conclusions
Clopidogrel in combination with aspirin is the cornerstone in the modern therapy of patients with ACS. A careful evaluation of the patient's bleeding risk is warranted due to the higher risk of bleeding complications.
The concept of clopidogrel resistance and the need for a pretreatment in patients undergoing coronary stent implantation lead to the concern that an improved antiplatelet regimen with novel drugs is desirable.
Disclosure
The authors report no conflicts of interest.