
Abstract
Metformin is now the most widely prescribed oral hypoglycemic agent. This review outlines its use in the treatment of type 2 diabetes. The main mechanisms of action include reduction of appetite and of intestinal carbohydrate absorption, inhibition of hepatic gluconeogenesis, and increased glucose uptake by peripheral tissues. Metformin has been established as the drug of choice for the first-line treatment of type 2 diabetes. According to broadly accepted guidelines, it should be administered early at diagnosis of this metabolic disorder, alongside diet and exercise. This agent may also be safely and efficaciously combined with all other oral hypoglycemic agents, enabling a useful additive effect. Additionally, it may be prescribed in conjunction with insulin. This combination aims to offset insulin resistance, reduce insulin requirements and minimize weight gain. Of greater importance, metformin has been consistently shown to have a favorable effect on cardiovascular risk factors and to improve cardiovascular outcomes. Interestingly, the efficacy of metformin is accompanied by excellent safety: caution is only needed to avoid the drug in patients with obvious contraindications (mainly chronic renal failure, congestive heart failure, chronic obstructive pulmonary disease, liver disease). Moreover, the cost-effectiveness of metformin has been established. Generally, metformin is an excellent choice both in the specialized setting and in primary health care.
Introduction
During the last 20 years type 2 diabetes mellitus has become a major health issue reaching epidemic proportions.1,2 It has recently been estimated that nearly 6% of the world's adults are affected by this condition. 3 As a result, patients have a considerably increased risk of vascular disease, which may affect both large arteries (macrovascular, i.e. cerebrovascular, coronary and peripheral arterial disease), and small arteries (microvascular disease, i.e. retinopathy, neuropathy and nephropathy).4,5 Overall, these chronic vascular complications lead to increased morbidity and mortality.4,6 In an effort to optimize glycemic control and also to reduce the burden of diabetic complications, several classes of oral hypoglycemic agents have been developed.7,8 Biguanides represent one of the oldest classes of oral hypoglycemic agents used in the management of type 2 diabetes mellitus. 9 Phenformin was the first biguanide to be marketed in the 1950's, while buformin and metformin soon followed.9–11 This review outlines the use of metformin. Not only is this drug the most widely prescribed antidiabetic agent 12 in the management of type 2 diabetes, but it has also been recommended as the first line treatment of choice in patients without contraindications.7,8
Search Strategy
Article search was based on the PubMed database up to December 2008 using combinations of the following keywords: combination, diabetes mellitus, efficacy, metformin, oral hypoglycemic agents, treatment. All types of articles (randomized controlled trials, original studies, review articles, case reports) were included. Publications were studied in full, but only the abstracts were considered for studies not written in English.
Metformin: Place in Therapy
Metformin has now been on the market for more than 50 years and has been established as the first-line agent of choice for the management of type 2 diabetes. In this context, the joint guidelines issued by the American Diabetes Association and the European Association for the Study of Diabetes strongly and repeatedly suggest that this agent should be used alongside lifestyle modification at diagnosis of type 2 diabetes.7,8 In this way, metformin is anticipated to reduce insulin resistance, contribute to weight loss, and play a significant role in the improvement of cardiovascular outcomes.7,8,13,14 A further advantage is that metformin can safely and efficaciously be combined with all other oral anti-diabetic agents.7,8,13,14 Such combinations enable an additive effect of metformin and the other agents, whether these act in an insulin-secretory or insulin-sensitizing mode.7,8 Similarly, metformin may be administered in conjunction with insulin. All in all, metformin is an excellent choice both in the specialized setting and in primary health care.7,8,13,14
Pharmacokinetic Profile, Metabolism and Mechanism of Action
Like phenformin, metformin is a derivative of guanidine, the active ingredient in goat's rue, that had empirically been used as a treatment for diabetes in the middle ages.9,10 In the digestive tract, it is absorbed by the small intestine. 15 Its oral bioavailability ranges between 40% and 60%, and gastrointestinal absorption is virtually complete after 6 hours of oral administration.16–18 A negative correlation has been described between oral dose and drug absorption.16,17 Following absorption, metformin is rapidly distributed, without binding to plasma proteins. In contrast to phenformin, metformin does not undergo liver metabolism and is excreted unchanged by the kidneys.16,17 Mean plasma half-life following oral administration ranges between 4 and 8.7 hours.16,19 Plasma half-life is significantly prolonged in patients with renal impairment and shows a close relationship to creatinine clearance.16,19 Metformin has no clinically relevant interactions with other drugs, because it is not metabolized and does not inhibit the metabolism of other drugs.16,20 There are only anecdotal reports on drug interactions in healthy volunteers, indicating that metformin levels may be reduced by guar gum and α-glucosidase inhibitors, and may be increased by cimetidine. 16 However, these observations have not been confirmed in the diabetic population.16,20
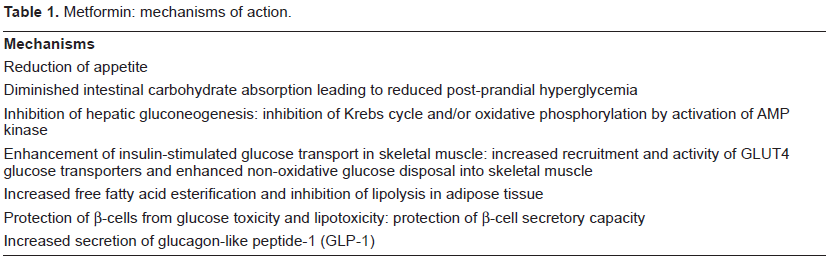
Metformin appears to have several, incompletely understood but complementing each other, modes of action (Table 1).21,22 The main mechanisms include anorexiogenesis, reduction of intestinal carbohydrate absorption, inhibition of hepatic gluconeogenesis, as well as increased glucose uptake by peripheral tissues.21–23 Reduced appetite is a useful action of metformin, contributing to weight loss, which is beneficial, given that the vast majority of patients are obese. 21 Diminished intestinal carbohydrate absorption plays a role in reducing post-prandial hyperglycemia,21,24 which is now regarded as a cardinal factor in the induction of oxidative stress leading to cardiovascular complications. 25 Evidence for this effect of metformin on the intestine comes mainly from animal and, to a lesser extent, from human studies.26,27 It appears that metformin delays intestinal glucose absorption and shifts this absorption more distally along the intestine.26,27 Additionally, it increases anaerobic glucose metabolism in the intestine, leading to reduced passage of glucose from the luminal to the serosal side of the intestine.26,27 Inhibition of hepatic gluconeogenesis and increased peripheral glucose uptake by metformin are major effects that offset insulin resistance, and their molecular basis is being increasingly studied.28–30 At the hepatocellular level, metformin acts on the mitochondria by inhibiting Krebs cycle and/or oxidative phosphorylation by activation of AMP kinase. 28 More recent experimental evidence points to a potent inhibitory effect of metformin on the phosphorylation of the transcriptional coactivator of CREB (cAMP response element-binding protein) at serine 436.29,30 This effect is mediated by an atypical protein kinase C (PKC iota/lambda), triggers the dissociation of important transcription complexes and reduces the expression of genes that promote gluconeogenesis. 30 Insulin-stimulated glucose transport in insulin-resistant human skeletal muscle is also augmented by metformin administration.31–33 Increased recruitment and activity of GLUT4 glucose transporters and enhanced non-oxidative glucose disposal into skeletal muscle have been documented.31–33 In adipose tissue, metformin promotes free fatty acid esterification and inhibits lipolysis.31–33 The increase in peripheral (muscle and adipose tissue) glucose disposal may lead to a 20%-30% reduction in glucose levels.31–33 Of note, reduction of glucose levels and of lipolysis protects β-cells from glucose toxicity and lipotoxicity, respectively.31–33 In this manner, metformin may protect β-cell secretory function.33,34 Finally, latest investigations indicate that increased secretion of glucagon-like peptide-1 (GLP-1) may be a further, hitherto unknown mechanism contributing to the efficacy of metformin. 35 Overall, the diversity and the collective efficacy of the aforementioned cellular actions of metformin justify its characterization as a “mulititasking medication”. 13
Metformin: mechanisms of action.
Efficacy: Major Clinical Studies
The efficacy of metformin, both in monotherapy and in combination therapy, has been documented by a large number of studies, the most important of which will be briefly described in this section. Overall, metformin monotherapy has been estimated to lower HbA1c by approximately 1.5%. 8 In combination, metformin can also significantly lower HbA1c, and the magnitude of the effect depends on the therapeutic combination, the follow-up of the study and the type of subjects recruited.8,19
The glucose-lowering effect of metformin is clearly dose-dependent.36–38 In a 14-week, multicenter, double-blind study, Garber et al randomized 451 patients to placebo or metformin with doses of 500, 1000, 1500, 2000, or 2500 mg daily over 11 weeks. 36 HbA1c dropped by -0.6% to -2.0% with increasing daily metformin dose (500 to 2000 mg), and differences between dosage groups were significant (p < 0.05). 36 This favorable dose-response relationship has been confirmed.37,38 Fujioka et al randomized 742 patients to metformin extended-release 500 mg once daily, 1000 mg once daily, 1500 mg once daily, 2000 mg once daily, 1000 mg twice daily or placebo for 16 weeks, demonstrating a clear dose-response relationship at daily metformin doses between 500 mg and 1500 mg. 38 In comparison with placebo, treatment differences amounted to -0.6% (500 mg once daily), -0.7% (1000 mg once daily), -1.0% (1500 mg once daily) and -1.0% (2000 mg once daily). 38 It appears that 1500 mg and 2000 mg per day represent the optimal metformin dosages for most patients.36,38
Metformin monotherapy has been assessed in a number of studies. A German trial randomized 96 patients to metformin 2 × 850 mg/day, acarbose 3 × 100 mg/day or placebo. 39 It was shown that both drugs were equally active compared with placebo (p < 0.05 for the comparisons with placebo): HbA1c dropped to 9.8% with placebo, 8.5% with acarbose, and 8.7% with metformin. 39 Similarly, a study of 205 patients with recently diagnosed type 2 diabetes, who were randomized to either 30 mg pioglitazone or 850 mg metformin daily with titrations upward to 45 mg and 2550 mg, respectively, showed that both drugs were equally active. 40 Specifically, HbA1c and fasting plasma glucose were comparable at the end of the study (pioglitazone: -1.3% reduction of HbA1c, p < 0.0001 vs. baseline; metformin: -1.5% reduction of HbA1c, p < 0.0001 vs. baseline; pioglitazone vs. metformin: p = 0.280). 40 However, pioglitazone was significantly more effective than metformin in improving sensitivity (reduction of fasting serum insulin, p = 0.003; homeostasis model assessment, p = 0.002). 40
The ADOPT (A Diabetes Outcomes Progression Trial) Study group evaluated rosiglitazone (4-8 mg), metformin (850-1700 mg), and glyburide (5-10 mg) as initial treatment for patients with newly diagnosed type 2 diabetes in a double-blind, randomized, trial of 4360 patients with a median treatment duration of 4 years. 41 The primary outcome was the time to monotherapy failure, defined as fasting plasma glucose exceeding 180 mg/dl. 41 Incidence of monotherapy failure at 5 years was 15% with rosiglitazone, 21% with metformin and 34% with glyburide. 41 Thus, rosiglitazone was associated with 32% lower failure risk as compared with metformin (p < 0.001) and 63% lower failure risk as compared with glyburide (p < 0.001). 41 However, there was no difference in the proportion of patients reaching a glycemic target of HbA1c lower than 7%. 41 Moreover, metformin-treated patients had more gastrointestinal untoward effects, but lower body weight (mean difference: 6.9 kg) than those receiving rosiglitazone. 41
A 24-week, randomized, double-blind, placebo-controlled trial allocated 1091 patients with type 2 diabetes to sitagliptin 100 mg/metformin 1000 mg, sitagliptin 100 mg/metformin 2000 mg, metformin 1000 mg, metformin 2000 mg, sitagliptin 100 mg, or placebo. 42 In monotherapy, both agents accomplished significant reductions in HbA1c, which were slightly more pronounced with metformin (-1.30% with metformin 2000 mg, -0.99% with metformin 1000 mg and -0.83% with sitagliptin 100 mg). 42 The comparison with the other dipeptidyl peptidase-4 (DPP-4) inhibitor, vildagliptin, was the aim of a double-blind, randomized, study of one-year treatment with vildagliptin (100 mg daily, n = 526) or metformin (up to 2000 mg daily, n = 254) in drug-naïve patients. 43 Once more, both agents accomplished significant reductions in HbA1c, which were slightly more pronounced with metformin (-1.4% with metformin and -1.0% with vildagliptin). 43 Thus, the statistical non-inferiority of 50 mg vildagliptin twice daily to 1000 mg metformin twice daily could not be established. 43 Of note, body weight was unchanged with vildagliptin (p = 0.17), but was lowered with metformin (p < 0.001). 43 Diarrhea, nausea and abdominal pain were twice more frequent with metformin, while hypoglycemia was similarly rare in both groups (<1%). 43
The efficacy of metformin monotherapy has been evaluated in a very comprehensive Cochrane review. 44 In this review, 29 trials with 5259 participants were included. 44 Metformin was compared with sulphonylureas (13 trials), glitazones (3 trials), meglitindes (2 trials), α-glucosidase inhibitors (2 trials), placebo (12 trials), diet (3 trials) and insulin (2 trials). 44 Metformin monotherapy was linked with a significant benefit in glycemic control, weight reduction, lipidemic profile and diastolic blood pressure. 44 In terms of glycemic control, metformin was significantly superior to placebo or diet and modestly better than sulphonylureas. 44 Serum lipids and body weight were also improved with metformin than with sulphonylureas. 44 The authors concluded that placebo, sulphonylureas, α-glucosidase inhibitors, glitazones, meglitinides, insulin and diet could not produce a more favorable effect on glycemic control, body weight, or serum lipids than metformin. 44
Metformin combination therapy has been the object of several studies. Evidence from these works documents that metformin can safely and efficaciously be combined with all types of oral hypoglycemic agents and/or insulin. The first type of combination therapy involves the addition of a sulphonylurea. In a study of 165 patients, Hermann et al found that the combination of metformin (500-1500 mg) and glibenclamide (5-10 mg) is safe and clinically useful. 45 When the two agents were combined, a significantly (p = 0.026) greater reduction of fasting plasma glucose was observed (p = 0.013). 45 In another randomized, double-blind, controlled study, 213 patients allocated to metformin (850-1500 mg) and glyburide (5-10 mg) had lower mean fasting plasma glucose concentrations (187 ± 4 vs. 261 ± 4 mg/dl, p < 0.001) and HbA1c (7.1% ± 0.1% vs. 8.7% ± 0.1%, p < 0.001) than 210 patients allocated to glyburide alone. 46
Moreover, in a French randomized, multicenter study, 372 patients were treated for 5 months with metformin (850 mg three times per day), glimepiride (starting dose 1 mg and titration up to 6 mg) or metformin and glimepiride. 47 Combination treatment produced significantly greater reductions of HbA1c (changes: +0.07% ± 1.20% for metformin, +0.27% ± 1.10% for glimepiride, -0.74% ± 0.96% for combination treatment, p < 0.001), fasting blood glucose (changes: +14.4 ± 7.2 mg/dl for metformin, +12.6 ± 55.8 mg/dl for glimepiride and -32.4 ± 39.6 mg/dl for combination treatment, p < 0.001) and post-prandial blood glucose (changes: +19.8 ± 106.2 mg/dl for metformin, +1.8 ± 91.8 mg/dl for glimepiride and -46.8 ± 70.2 mg/dl for combination treatment, p < 0.001) than either agent alone. 47 Improved efficacy was accompanied by significantly (p = 0.039) more frequent symptomatic hypoglycemia in the combination group. 47
A 4-month double-blind, multicenter trial allocated 411 patients to metformin 500 mg, glibenclamide 5 mg, metformin-glibenclamide 500 mg/2.5 mg or metformin-glibenclamide 500 mg/5 mg. 48 The reductions in HbA1c and fasting plasma glucose proved significantly (p < 0.05) more pronounced for metformin-glibenclamide 500 mg/2.5 mg (-1.20% and -47.16 mg/dl) and 500 mg/5 mg (-0.91% and -42.12 mg/dl), compared with metformin (-0.19% and -10.26 mg/dl) or glibenclamide (-0.33% and -13.14 mg/dl). 48 The glycemic endpoint of HbA1c < 7% was accomplished significantly (p = 0.001) more frequently by patients receiving metformin-glibenclamide 500 mg/2.5 mg and 500 mg/5 mg (75% and 64%, respectively) than those receiving glibenclamide (42%) and metformin (38%) alone. 48 These favorable effects were obtained with lower metformin and glibenclamide doses in the combined treatment group than in patients receiving either drug alone. 48 In a 16-week, randomized, double-blind trial, 639 patients inadequately controlled on at least half-maximal dose of sulphonylurea were assigned to glyburide 10 mg, metformin 500 mg, glyburide/ metformin 2.5 mg/500 mg, or glyburide/metformin 5 mg/500 mg. 49 Glyburide/metformin combination succeeded in reducing HbA1c by -1.7% more than glyburide alone (p < 0.001) and by -1.9% more than metformin alone (p < 0.001), ultimately leading to lower fasting plasma glucose levels than glyburide (p < 0.001) or metformin groups (p < 0.001). 49
The additive effect of glipizide/metformin combination was assessed in a randomized a multicenter, parallel-group, active-controlled trial recruiting 247 patients. 50 Patients were randomized to glipizide 30 mg, metformin 500 mg, or glipizide/ metformin 5/500 mg tablets for 18 weeks. 50 Maximum total daily doses were glipizide 30 mg, metformin 2000 mg, and glipizide/metformin 20/2000 mg. 50 Glipizide/metformin combination exerted a superior effect in terms of HbA1c reduction (p < 0.001), as well as improvement (p < 0.05) of fasting glucose levels and 3-hour postprandial glucose levels than did either drug in single therapy. 50 Four times more patients attained HbA1c < 7.0% with glipizide/metformin (36.3%) than either glipizide (8.9%) or metformin (9.9%) alone. 50 In another multicenter, double-blind, placebo-controlled study, 122 patients with type 2 diabetes inadequately controlled on a stable metformin dose of at least 1000 mg were randomized to add-on 2.5 mg glipizide GITS or add-on placebo. Overall, glipizide significantly improved glucose control. 51 In patients receiving metformin plus glipizide, HbA1c was reduced from 7.45% ± 0.1% to 6.8% ± 0.1%, compared with a change from 7.64% ± 0.1% to 7.46% ± 0.1%, in the placebo group (p < 0.0002). 51 In the metformin plus glipizide group, fasting glucose was reduced from 154 ± 4 mg/dl to 132 ± 4 mg/dl, compared with a change from 156 ± 4 mg/dl to 153 ± 5 mg/dl in the placebo group (p < 0.0002). 51
Other types of combination therapy include the addition of meglitindes, α-glucosidase inhibitors, glitazones, newer agents, or insulin. In 467 patients on high-dose metformin, add-on nateglinide led to significant reductions of HbA1c (-0.36%, p = 0.003, with nateglinide 60 mg; -0.59%, p < 0.001, with nateglinide 120 mg), linked with a modest decrease of fasting glucose levels. 52 In a more recent doubleblind randomized trial of 262 patients suboptimally controlled on maximal metformin doses, nateglinide plus metformin and gliclazide plus metformin combinations proved equally efficacious in terms of final HbA1c (-0.14% for nateglinide vs. -0.27% for gliclazide; p = 0.396) and proportion of patients (40% vs. 47.4%) achieving an endpoint HbA1c < 7%. 53 Fasting plasma glucose changed from baseline to 52 weeks by -3.6 mg/dl with nateglinide and -12.6 mg/dl with gliclazide (p = 0.096). 53
There is also considerable experience with repaglinide plus metformin combination. 54 This combined therapy may reduce fasting plasma glucose by -39.6 mg/dl and HbA1c by -1.4%. 54 The efficacy and safety of this combination render it a valuable option in the management of patients with type 2 diabetes, according to some experts.55,56 Therefore, a new repaglinide/metformin fixed-dose combination tablet for either twice or three times per day administration has now been developed. 56
In a 12-month, multicenter, randomized, doubleblind, placebo-controlled study, 354 patients were assigned to placebo or acarbose (initial dose 50 mg, titration to 100 mg, and finally to a maximum of 200 mg) in addition to their usual diet/metformin/sulfonylurea/insulin regimen. 57 Compared with placebo, acarbose significantly lowered postprandial glucose from 318.6 mg/dl to 237.6 mg/dl for the diet alone group, from 347.4 mg/dl to 284.4 mg/dl for the metformin group, from 372.6 mg/dl to 298.8 mg/dl for the sulfonylurea group, and from 331.2 mg/dl to 282.6 mg/dl for the insulin group (p < 0.01 vs. placebo). 57 Initially, mean HbA1c amounted to 6.7% ± 0.2% for the diet alone group, 7.8% ± 0.2% for the metformin group, 8.0% ± 0.2% for the sulfonylurea group, and 7.7% ± 0.2% for the insulin group. 57 At the end of the trial period, HbA1c was lower in patients receiving acarbose than in patients receiving placebo; the difference was -0.9% for the diet alone group (P = 0.005), -0.8% for the metformin group (p = 0.011), -0.9% for the sulfonylurea group (P < 0.002), and -0.4% for the insulin group (p = 0.077). 57
The efficacy of metformin plus acarbose combination has been confirmed in a more recent multicenter, randomized, double-blind, placebo-controlled trial enrolling 89 overweight patients inadequately controlled by metformin. 58 These were randomized to acarbose (titrated up to 100 mg three times daily) or placebo. 58 Metformin plus acarbose yielded a significant reduction of both mean HbA1c by -1.02% (p = 0.0001) and mean fasting glucose by -20.38 mg/dl (p = 0.0395). 58 Metformin has also been successfully combined with miglitol, a very rarely used α-glucosidase inhibitor. 59 In a multicenter, double-blind, placebo-controlled study, 324 patients were allocated to either placebo, miglitol alone (titrated to 100 mg three times a day), metformin alone (500 mg three times a day), or miglitol plus metformin for 36 weeks. 59 Metformin plus miglitol demonstrated a reduction in HbA1c of -1.78% (p = 0.002). 59 Fasting plasma glucose (-44.8 vs. -20.4 mg/dl; p = 0.0025) and postprandial glucose (-59.0 vs. -18.0 mg/dl; p = 0.0001) were also significantly improved. 59 In another work published in the same year, miglitol (titrated to 100 mg three times a day) added to metformin (1500-2250 mg/day) was compared to placebo added to metformin in 152 patients. 59 Miglitol plus metformin led to a significant reduction of HbA1c (-0.21% with miglitol vs. +0.22% with placebo, p = 0.011) and a significant reduction of post-meal glucose (final values: 248.4 mg/dl for miglitol vs. 284.4 mg/dl for placebo, p = 0.0007). 60
The combination of metformin and glitazones (rosiglitazone and pioglitazone) has been adequately investigated. A randomized, double-blind, placebo-controlled 26-week trial recruited 348 patients with a mean HbA1c of 8.8%, allocated to 2.5 g metformin plus placebo, 2.5 g metformin plus 4 mg rosiglitazone, or 2.5 g metformin plus 8 mg rosiglitazone. 61 Compared with the metformin-placebo group, HbA1c decreased by -1.0% in the 4 mg metformin-rosiglitazone group and by -1.2% in the 8 mg metformin-rosiglitazone group (p < 0.001). 61 Likewise, fasting plasma glucose decreased by -39.8 mg/dl and -52.9 mg/dl compared placebo group (p < 0.001).
In 116 Mexican patients inadequately controlled with 2.5 g/day metformin, who were randomized to add-on rosiglitazone 2 mg or 4 mg twice daily vs. placebo, HbA1c decreased significantly in the rosiglitazone 2 mg twice daily (-0.7%; p = 0.0052) and 4 mg twice daily (-1.2%; p = 0.0008) groups, but increased in the placebo group (+0.3%; p = 0.2651). 62 Fasting glucose also diminished in a dose-ordered manner compared with placebo (p ≤ 0.0019 and p = 0.0006, respectively). 62 Another work showed fixed rosiglitazone/metformin 4 mg/2 g per day combination superior to 2.5 g per day metformin in 551 patients. 63 Specifically, HbA1c was reduced from 7.4% to 7.1% as compared with 7.5% to 7.4% (p = 0.001). 63 Fasting plasma glucose was reduced from 166.2 mg/dl to 144.1 mg/dl as compared with 169.3 mg/dl to 164.0 mg/dl (p < 0.001). 63 The glycemic target of HbA1c < 7.0% was attained in 54% of patients treated with rosiglitazone/metformin and 36% in the metformin-only group (Odds Ratio: 2.42; p < 0.001). 63
In a multicenter, double-blind, randomized 24-week study, 766 subjects on a stable dose of 1000 mg/day metformin were randomized to rosiglitazone 4 mg/day or metformin 1500 mg/day for 8 weeks. 64 Rosiglitazone plus metformin treatment led to a mean reduction of HbA1c by -0.93%, and high-dose metformin (2 g per day) led to a comparable mean reduction of -0.71%. 64 Significantly (p < 0.05) more subjects arrived at an HbA1c < 7% in the rosiglitazone plus metformin group than the metformin only group (58.1% versus 48.4%). 64 Moreover, Garber et al randomized 318 patients to metformin-glibenclamide (1000/5 mg per day) or metformin 500 mg plus rosiglitazone 4 mg ((1000-2000 mg/4 mg per day) for 24 weeks. 65 Metforminglibenclamide-treated patients had significantly greater reductions of HbA1c (-1.5%) and fasting glucose (-46 mg/dl) than metformin-rosiglitazone-treated patients (-1.1%, p < 0.001; -36 mg/dl, p = 0.03). 65 At the end of the study, HbA1c was lower than 7% in more patients receiving metformin-glibenclamide than in those on metformin plus rosiglitazone (60 vs. 47%, p < 0.05). 65
An Italian study in 99 type 2 diabetic patients with metabolic syndrome compared add-on glimepiride (2 mg/day) to add-on rosiglitazone (4 mg/day) in patients on a stable metformin dose of 1500 mg/day. 66 Both treatments significantly (p < 0.05 vs. baseline) reduced BMI, HbA1c, fasting and post-prandial glucose. 66 In patients receiving metformin plus glimepiride, BMI was reduced from 26.5 ± 1.3 kg/m2 to 25.2 ± 1.4 kg/m2, HbA1c was reduced from 7.7% ± 0.5% to 7.0% ± 0.7%, fasting glucose was reduced from 164 ± 20 mg/dl to 152 ± 20 mg/dl and postprandial glucose was reduced from 185 ± 18 mg/dl to 171 ± 21 mg/dl. 66 In patients receiving metformin plus rosiglitazone, BMI was reduced from 25.9 ± 1.3 kg/m2 to 24.5 ± 1.1 kg/m2, HbA1c was reduced from 7.4% ± 0.6% to 6.8% ± 0.6%, fasting glucose was reduced from 156 ± 25 mg/dl to 139 ± 19 mg/dl and postprandial glucose was reduced from 190 ± 22 mg/dl to 170 ± 18 mg/dl. 66 In the rosiglitazone group, significant (p < 0.05 vs. baseline) improvements were also observed in fasting plasma insulin, as well as homeostasis model assessment index, but significant reductions in total cholesterol, LDL-Cholesterol and Apo B (p < 0.05) were obtained in the glimepiride group. 66
As regards pioglitazone, a 16-week, double-blind trial randomizing 328 patients to once-daily pioglitazone 30 mg + 1000 mg metformin or placebo + 1000 mg metformin showed that pioglitazone plus metformin therapy led to significant decreases in HbA1c (-0.83%) and fasting plasma glucose (-37.7 mg/dl) compared with placebo + metformin (p ≤ 0.05), which were accompanied by significant (p ≤ 0.05) improvements in triglycerides (-18.2%) and HDL-cholesterol (+8.7%). 67 A further work randomized 639 patients inadequately controlled on gliclazide to additional treatment with either pioglitazone (15-45 mg/day) or metformin (850-2550 mg/day). 68 At the end of the trial, mean reduction in HbA1c was -0.89% for pioglitazone plus gliclazide and -0.77% for metformin plus gliclazide (p = 0.200). 68 Pioglitazone improved serum lipids, but was associated with considerable increase in weight (+3.7 kg), whereas metformin led to a mean weight loss of -1.7 kg. 68
Umpierrez et al randomized 203 type 2 diabetic patients poorly controlled on metformin (>1 g/day) to 2-4 mg glimepiride or 30 mg pioglitazone. 69 Both treatments achieved comparable improvements in HbA1c (p = 0.0001) and fasting glucose (p < 0.05), but glimepiride was linked with faster glycemic control, lower total and LDL cholesterol levels and increased risk of hypoglycemia. 69
The combination of metformin with DPP-4 inhibitors (sitagliptin, vildagliptin and the newer saxagliptin) is another therapeutic option. The efficacy and safety of sitagliptin, added to metformin therapy was assessed in a French randomized placebo-controlled trial recruiting 701 patients poorly controlled on metformin ≥1500 mg per day. 70 This confirmed the superiority of add-on sitagliptin (100 mg per day) over placebo in HbA1c and fasting glucose. 70 HbA1c was reduced from 7.96% ± 0.81% to 7.26% ± 0.97% with sitagliptin and from 8.03% ± 0.82% to 7.95% ± 1.10% with placebo (p < 0.001). 70 Fasting glucose was reduced from 169.2 ± 41.4 mg/dl to 151.2 ± 39.6 mg/dl with sitagliptin and increased from 172.8 ± 41.4 mg/dl to 178.2 ± 50.4 with placebo (p < 0.001). 70 Significantly (p < 0.05) more patients arrived at an HbA1c < 7% with sitagliptin (47%) than with placebo (18.3%), and this was accomplished without any increase in hypoglycemias and other side-effects. 70 Another group conducted a randomized trial of 1172 patients inadequately controlled on metformin monotherapy (>1000 mg per day). 71 These were assigned to sitagliptin 100 mg per day or glipizide 5 mg/day (uptitrated to a potential maximum 20 mg/day). 71 It was shown that the combination of metformin plus sitagliptin was equally effective in reducing HbA1c as metformin plus glipizide. 71 An HbA1c < 7% was accomplished in 63% of patients receiving sitagliptin and 59% of those receiving glipizide. 71 Fasting plasma glucose changes from baseline were -10.0 mg/dl for sitagliptin and -7.5 mg/dl and for glipizide. 71 Brazg et al randomized 28 patients on a stable metformin dose (≥1500 mg per day) to addition of sitagliptin 100 mg twice daily vs. placebo. 72 Compared with placebo, sitagliptin plus metformin succeeded in reducing mean glucose (by -17.6 mg/dl vs. -2.7 mg/dl, p = 0.004), fasting glucose (by -23.1 mg/dl vs. -7.7 mg/dl, p < 0.001) and fructosamine (by -24.8 mmol/l vs. -6.5 mmol/l, p < 0.001). 72
There is also data to support the combination of metformin with vildagliptin or saxagliptin. A study in 780 drug-naïve patents showed that significantly (p < 0.001) more patients attain the target of HbA1c < 7% with metformin plus vildagliptin combination than with either metformin (titrated to 2000 mg daily) or vildagliptin (100 mg daily) alone. 43 In a further investigation of 107 patients, vildagliptin (50 mg daily) or placebo was added to metformin treatment (1.5-3.0 mg/day). 73 HbA1c decreased significantly with vildagliptin vs. placebo (mean between-group difference: -1.0% ± 0.2%; p < 0.001). 73 This also held true for fasting glucose (mean difference: -16.2 ± 5.4 mg/dl; p = 0.016). 73 Bosi et al conducted a doubleblind, randomized, multicenter, study in 544 patients on a stable metformin dose ≥ 1500 mg per day. 74 These were allocated to the addition of 50 mg vildagliptin, 100 mg vildagliptin, or placebo. 74 HbA1c was reduced by -0.7% ± 0.1% (p < 0.001) with 50 mgand by -1.1 ± 0.1% (p < 0.001) with 100 mg vildagliptin. 74
The newer saxagliptin may be combined with metformin as well. A randomized, double-blind, placebo-controlled study of saxagliptin (2.5, 5, or 10 mg once daily) or placebo, added to stable dose of metformin (1500 to 2500 mg) in 743 patients showed the efficacy of this combination. 75 In a dose-dependent fashion, HbA1c was reduced (-0.59%, -0.69%, and -0.58% vs. +0.13% with placebo; p < 0.0001). 75 Fasting glucose showed the same decrease (-14.31 mg/dl, -22.03 mg/dl, and -20.50 mg/dl vs. +1.24 mg/dl with placebo; p < 0.0001). 75 Therefore, DPP-4 inhibition plus metformin is now emerging as a new promising therapeutic choice in type 2 diabetes. 76
Metformin can also be safely and efficaciously combinedwithGLP-1 analogues(exenatide, liraglutide). Initially, a trial in 109 metformin-treated patients showed that exenatide can reduce HbA1c (p ≤ 0.006) over placebo. 77 At the end of the study, HbA1c < 7% was attained by 15% of exenatide-treated patients vs. 4% of those receiving placebo. 77 In another trial, 156 patients were randomized to placebo or exenatide at 2.5, 5.0, 7.5, or 10.0 μg twice daily. 78 HbA1c was dose-dependently reduced (-0.1% ± 0.1%, -0.3% ± 0.1%, -0.4% ± 0.1%, -0.5% ± 0.0%, and -0.5% ± 0.1% for placebo and 2.5, 5.0, 7.5, and 10.0 μg exenatide, respectively; p < 0.0001). 78 Fasting plasma glucose was also reduced (+6.8 ± 4.1 mg/dl, -20.1 ± 5.2 mg/dl, -21.2 ± 3.9 mg/dl, -17.7 ± 4.8 mg/dl, and -17.3 ± 4.4 mg/dl for placebo and 2.5, 5.0, 7.5, and 10.0 μg exenatide, respectively; p = 0.0006). 78 Similarly, in 150 patients poorly controlled with maximal doses of metformin, add-on exenatide resulted in a mean HbA1c reduction of 1%, which was sustained after 82 weeks. 79 At 30 weeks, 46% had within-target HbA1c below 7%, aproportion increasing to 59% at 82 weeks. 79 A triple-blind, placebo-controlled, 30-week study of 336 patients uncontrolled by maximal dose of metformin found that adding 5 or 10 μg exenatide reduced HbA1c by 0.78% ± 0.10% (10 μg) or 0.40% ± 0.11% (5 μg) (p < 0.002 vs. placebo). 80 Overall, 46% (10 μg), 32% (5 μg), and 13% (placebo) achieved HbA1c ≤ 7% (p < 0.01 vs. placebo). 80
Likewise, liraglutide plus metformin appears promising. Nauck randomized 144 type 2 diabetic subjects on metformin treatment (1000 mg twice daily) to metformin plus liraglutide (increasing dose of 0.5 to 2 mg daily), liraglutide, metformin, or metformin plus glimepiride (2-4 mg). 81 Liraglutide plus metformin combination was the most efficacious regimen, leading to a significant reduction in HbA1c by -0.8% and fasting glucose by -70.2 mg/dl. 81
Interestingly, metformin can be effectively combined with two hypoglycemic agents as part of a triple antidiabetic therapy. Four hundred and forty-one patients on high-dose metformin (≥1500 mg) and glimepiride (≥4 mg) were randomized to 100 mg once daily or placebo. 82 The triple regimen lowered HbA1c by -0.89% relative to placebo. 82 Kendall et al studied 733 patents on metformin ≥ 1,500 mg/day plus maximal doses of sulphonylurea to 5 μg or 10 μg exenatide twice daily or placebo. 83 Changes in HbA1c were -0.77% ± 0.08% (10-μg arm; p < 0.0001 vs. placebo), -0.55% ± 0.07% (5-μg arm; p < 0.0001 vs. placebo), and +0.23% ± 0.07% (placebo). 83 The favorable effect of this combination has been confirmed by other studies as well.84,85 In 222 patients on maximal doses of metformin plus sulfonylurea, the addition of 5 μg or 10 μg exenatide conferred a significant (p < 0.05) benefit over placebo. 84 Reduction in HbA1c amounted to -0.8% ± 0.1% with 5 μg and -1.0% ± 0.1% with 10 μg. 84 Heine et al randomized 551 patients on maximal doses of metformin and sulfonylurea to either insulin glargine (titrated to maintain fasting blood glucose <100 mg/dl) or 10 μg exenatide twice daily. 85 Both exenatide and insulin glargine reduced HbA1c by -1.11%. 85 Interestingly, exenatide appeared to target mainly postprandial glucose and glargine exerted its main effect on fasting glucose. 85
Finally, metformin can effectively be combined with insulin. The aim of using metformin in insulin-treated patients is to offset insulin resistance, reduce insulin requirements and minimize weight gain. A Finnish trial randomized 96 patients to bedtime intermediate-acting insulin plus glyburide and placebo, metformin and placebo, glyburide and metformin, or a second injection of intermediate-acting insulin in the morning. 86 The greatest reduction of HbA1c was accomplished in the bedtime insulin and metformin group (from 9.7% ± 0.4% to 7.2% ± 0.2%; p < 0.001, compared with baseline and p < 0.05 compared with other groups). 86 This therapeutic combination also succeeded in the lowest hypoglycemia rates (p < 0.05 compared with other groups) and in absence of weight gain (p < 0.001 compared with all other groups). 86 Another trial randomized 110 patients to bedtime insulin glargine with metformin or bedtime insulin NPH with metformin for 36 weeks. 87 Metformin was efficacious in both insulin combinations: final HbA1c was 7.14% ± 0.12% with glargine and 7.16% ± 0.14% with NPH. 87 Glargine plus metformin reduced symptomatic hypoglycemia and dinner-time hyperglycemia. 87
Not to be underestimated, metformin can be used in conjunction with various types of insulin. An international trial randomized 315 patients who were on metformin and/or a sulfonylurea with a stable dose of 0 to 2 daily insulin injections to receive insulin lispromix 50 (50% insulin lispro-protamine suspension and 50% lispro) three times daily plus metformin or bedtime insulin glargine plus metformin for 24 weeks. 88 Both combinations managed to improve metabolic control. Metformin fared better with lispromix50 than glargine in terms of HbA1c, post-prandial hyperglycemia and glycemic variability, whereas metformin plus glargine was superior in lowering fasting plasma glucose. 88
Safety
Metformin is considered one of the safest oral hypoglycemic agents.12,90 It reduces insulin resistance, but does not promote insulin secretion from β-cells, and thus it is not associated with increased risk of hypoglycemia.12,90 Minor untoward effects include nausea and diarrhea. They are usually mild and wane over the first days of treatment.12,14,89 Nonetheless, they may be dose-limiting and reduce patient compliance.12,14,89 Such side effects may be minimized by using the sustained-release metformin formulation, which has been shown to be much better tolerated.90,91
The major untoward effect is lactic acidosis.12,92–94 This condition still has a mortality up to 50%.12,92–94 However, it is now extremely rare, its incidence ranging between 0.01 and 0.15 per 1000 patient-years.13,21,93–99 More importantly, it virtually only occurs in patients with obvious contra-indications to metformin use.12,99 Contraindications are related to conditions predisposing to tissue hypoxia (congestive heart failure, chronic obstructive pulmonary disease, severe infection or gangrene), to liver disease, as well as to intrinsic or functional reduction of renal function (chronic renal failure, congestive heart failure, advanced age).12,21,100,101 This is explicable on the basis that metformin is cleared by the kidneys and that elevated serum lactic acid concentration may result either from severe tissue hypoxia or from reduced hepatic clearance owing to liver disease.12,21,100,101 Age itself is a much questioned contraindication, but most cases of lactic acidosis have been described in elderly patients, and several authors suggest avoidance of metformin in patients aged at least 80.12,102–105
Recently, the utility of the abovementioned contraindications has been debated.11,95,100,101,103,106–108 Even in patients with contra-indications, metformin-associated lactic acidosis is very rare and occurs due to a superimposed medical condition.11,103 Mortality is then closely related with the degree of hypoxia, rather than serum metformin levels, casting doubt on the causal role of metformin.11,103 More impressively, several studies have shown that a considerable proportion of patients receiving metformin have formal contraindications to its use and yet never develop lactic acidosis.11,95,100,101,103,106–108 Nevertheless, these studies have been criticized for their retrospective observational design and for the variable interpretation of contraindications.12,102 In practice, lactic acidosis remains a potentially lethal condition, and, therefore, the clinician should assess patients carefully before prescribing metformin, in order to avoid those with serious contraindications. 12 As long as contraindications and warnings are respected, metformin may be safely administered with almost no lactic acidosis.109,110
Cost-Effectiveness
Metformin has also proved cost-effective. The overall beneficial cost-effectiveness ratio has been estimated in various countries. In the UKPDS, cross-sectional surveys of non-inpatient healthcare use and quality of life revealed that the drug was cost-saving and that it increased life expectancy. 111 A further analysis estimated the costs and effectiveness of intensive blood glucose control in overweight type 2 diabetes patients in China. 112 Provided that one is willing to pay for quality-adjusted life year gained, intensive blood glucose control with metformin appears to be cost-effective. 112 The average incremental costs of 11 years of intensive treatment with metformin amounted to 16400 US$ per quality-adjusted life year gained. The incremental cost-effectiveness ratio favored metformin at 20 years (with 11700 US$) and 30 years (with 9600 US$). 112 Using the UKPDS results, modelling techniques were applied to the Swiss health system, in order to estimate the cost-effectiveness of the management type 2 diabetic patients by conventional vs. intensive control with metformin. 113 Total cost (including both diabetes therapy and management of new-onset complications) and survival were determined over an 11-year period. 113 Mean total cost per patient was 10877 Swiss Francs for conventional vs. 9950 Swiss Francs for intensive control with metformin. 113 In addition, intensive control with metformin prolonged survival by a mean of 0.43 life-years per patient. 113 A further analysis evaluated the cost-effectiveness of metformin vs. lifestyle changes for patients with impaired glucose tolerance in Australia, France, Germany, Switzerland, and the United Kingdom. 114 Both interventions were cost-effective in all countries, except for United Kingdom, where cost was slightly increased with either intervention. 114 In a similar patient sample in the USA, intensive lifestyle, metformin, and placebo were compared. 115 Compared with placebo, the cost per quality-adjusted life year gained amounted to $1100 for lifestyle intervention $31300 for metformin. 115 In terms of societal burden, the cost per quality-adjusted life year gained was $8800 dollars for lifestyle intervention and $29900 for metformin. 115 Overall, lifestyle intervention exhibited a superior cost-effectiveness over metformin. 115 Importantly, lifestyle intervention was cost-effective in all ages, whereas metformin was not sufficiently cost-effective for subjects aged older than 65. 115 Finally, in the Indian Diabetes Prevention Programme, lifestyle modification and metformin were compared. 116 Direct per subject costs over three years were $61 in the control group, $225 with lifestyle modification, $220 with metformin, and $270 with both modalities. 116 Thus, both lifestyle modification and metformin were cost-effective, the former more so than the latter. 116
Evidence for Additional Beneficial Effects beyond Glycemic Control
It is now widely accepted that metformin has a favorable effect on serum lipids, inflammation and cardiovascular disease.110,117–119 This effect is strong enough to translate into clinical benefit. The UKPDS demonstrated that metformin was the only oral agent to reduce any diabetes-related endpoint by 32% (p = 0.002), diabetes-related death by 42% (p = 0.017) and all-cause mortality by 36% (p = 0.011). 120 This reduction was sustained in the 20 year follow-up analysis, which again showed that metformin reduced any diabetes-related endpoint by 21% (p = 0.01), myocardial infarction by 33% (p = 0.005) and all-cause mortality by 27% (p = 0.002). 121 More recently, a randomized trial from Holland examined the effect of add-on metformin vs. placebo on cardiovascular morbidity in insulin-treated type 2 diabetic patients. 122 Metformin succeeded in almost 40% improvement of macrovascular disease after a median follow-up period of 4.3 years. 122
The overall vasculoprotective effect of metformin has been corroborated in a Cochrane analysis, which estimated a metformin-induced significant risk reduction for myocardial infarction (p = 0.02), diabetes-related death (p = 0.03) and all-cause mortality (p = 0.01). 44 A systematic review of cardiovascular outcomes associated with oral hypoglycemic agents also came to the conclusion that metformin could lead to a 26% risk reduction in cardiovascular mortality as compared to any other treatment or placebo. 123
Furthermore, metformin has beneficial effects on blood pressure, lipid profile and coagulation.110,119 The effect on blood pressure is rather moderate. According to a systematic review, this agent could only lower systolic blood pressure by -1.09 mm Hg (p = 0.30) and diastolic blood pressure by -0.97 mm Hg (p = 0.11). 124 As regards serum lipids, Nagi and Yudkin reported a significant beneficial effect of metformin on serum triglycerides (p = 0.034), total cholesterol (p = 0.002) and LDL-cholesterol (p = 0.002), but not on HDL-cholesterol. 125 The hypolipidemic action of metformin has also been shown in conjunction with insulin: a randomized trial found that addition of this drug resulted in significant reductions of total cholesterol (p = 0.032) and LDL-cholesterol (p = 0.028) without any effect on triglycerides and HDL-cholesterol. 126 Overall, metformin has consistently demonstrated a favorable, even though modest, effect on LDL-cholesterol, independently of glycemic control.44,124,127 In comparison with other agents, metformin succeeds in a reliable reduction of LDL-cholesterol by a mean of -10 mg/dl.44,124,127 The action on other lipidemic parameters is less documented. According to the systematic review by Wulffelé et al however, this biguanide reduced not only LDL-cholesterol (p < 0.00001), but serum triglycerides (p = 0.003) and total cholesterol (p < 0.0001) as well. 124 Metformin has been also shown to improve fibrinolysis by reducing plasminogen activator inhibitor-1 (p = 0.001). 125
The mechanisms by which metformin protects the heart and the large vessels appear to be manifold and possibly mutually interacting, but remain incompletely understood.110,119 Generally, most beneficial actions are attributable to the amelioration of insulin resistance.110,119 In addition, metformin has been proposed to harbor anti-oxidant activity, offset advanced glycation end-products, improve microcirculation and reduce inflammation.110,119
Conclusions
Metformin has a long history in the management of type 2 diabetes and is now the most widely prescribed oral hypoglycemic agent.12–14 Its main modes of action encompass anorexiogenesis, reduction of intestinal carbohydrate absorption, inhibition of hepatic gluconeogenesis, as well as increased glucose uptake by peripheral tissues.21–23 Metformin has been established as the drug of choice for the first-line treatment of type 2 diabetes, and its administration has been strongly suggested at diagnosis of this metabolic disorder, alongside diet and exercise.7,8 It may also be successfully combined with all other oral hypoglycemic agents and insulin.45,50,55,61,70,74,86 Of greater importance, this agent has been consistently shown to improve cardiovascular outcomes.119–122 This beneficial effect may be sustained several years after discontinuation of the drug. 121 The efficacy of metformin is accompanied by excellent safety: caution is only needed to avoid the drug in patients with contraindications. 12 Finally, the cost-effectiveness of metformin has been adequately established.111–113
Disclosures
The authors report no conflicts of interest.