
Abstract
Background
Medical termination of pregnancy [TOP] during the early first trimester is commonly used. However, treatment failure which warrants surgical intervention occurs in small proportion of patients. Our
Methods
Women who opted for medical TOP where treated by single dose of RU486 followed by a single dose of misoprostol. Endometrial thickness was evaluated by transvaginal U.S. at 14 days after misoprostol tretament. The data was collected prospectively for this cohort study which includes all the women undergoing medical abortion in the first seven weeks of gestation.
Results
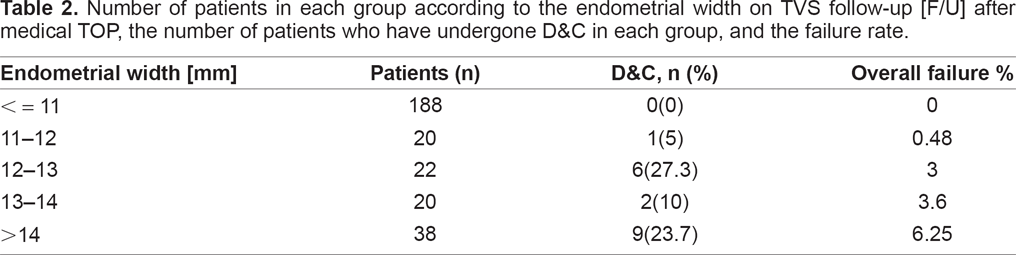
In 34.7% of the patients the endometrial width was > 11 mm on the follow-up visit. Surgical intervention was performed in 18% of these patients, for a failure rate of the medical termination of pregnancy [TOP] of 6.25%, as compared with no failure rate in those with endometrium < 11 mm, P < 0.001. In the patients where the endometrium was 11-12 mm on follow-up, the failure rate was 5%, and if > 12 mm the failure was 5.9%. In cases where the endometrium was 12-13 mm the failure rate was 27.3%, and if >13 mm the failure was 18.9%. When the endometrium was 13-14 mm the failure rate was 10%, and when >14 mm the failure was 23.7%. Half of the 18 patients who had undergone dilatation and curettage [D&C] for completion of the TOP, had endometrium > 14 mm, one to two weeks after the medical abortion.
Conclusion
Measurement of endometrial width after medical TOP is beneficial in segregating patient to low or high risk for surgical treatment of retained product of conception [POC]. Using a cutoff of 11 mm during the follow-up visit after medical TOP, 18% of the patients may need dilatation and curettage to complete the pregnancy termination, and if it is >14 mm, half of them may need surgical intervention. There is no difference between 11 and 14 mm regarding the risk of surgical intervention after medical TOP.
Introduction
Several medications have been put forward, either alone or in combination, for the non invasive termination of early gestation, also known as medical abortion, using a progesterone antagonist, such as RU486 (mifepristone), combined with prostaglandins, or methotrexate (1-4). Medical abortion in early pregnancy was found to be safe and effective, the most effective combination is that of mifepristone and misoprostol (a prostaglandin analogue) (1-4).
Treatment with a combination of mifepristone (RU 486, Mifegyne; Exelgyn, Paris, France) and the prostaglandin analogue misoprostol (Cytotec; Searle, High Wycombe, England), both administered orally within 48 hours of each other, has been shown to be an effective method for medical termination of pregnancy up to 49 days' gestation.(4-11).
This combination results in complete abortion in more than 96% of cases and the rate of continuing pregnancies is less than 1% in gestations up to 63 days' amenorrhea (12-14). Failure of treatment which is defined as the need for surgical intervention to complete the abortion occurs in 2% to 8% (15-18 http://www.sciencedirect.com/science).
There is no consensus regarding the follow-up or the indications for surgical intervention (19). Reasons for early curettage usually have included retained POC, intractable pain, or massive bleeding. Late failures are generally noticed after the 2- to 4-week follow-up visit and are defined as retained POC, commonly presenting with prolonged vaginal bleeding.
The diagnosis of failed medical abortion leads to surgical intervention often performed under general anesthesia. To avoid unnecessary interventions, the positive predictive value of such an applied test must be high. The specificity should be more than 95%, which is the approximate chance of a successful course using this medical abortion regimen (15).
It is important for both, the women who undergo medical abortion, and the physician, to confirm that the pregnancy has been completely terminated. If expulsion of the products of conception was confirmed by an experienced physician in the hours after administration of the prostaglandin, further follow-up is probably not necessary (20). Otherwise, a follow-up visit should be arranged about two weeks after the administration of mifepristone. At the follow-up visit, complete abortion should be confirmed clinically, either by bimanual pelvic examination or, preferable, by pelvic ultrasound. If serial measurements of human chorionic gonadotrophin (hCG) in blood or urine are used, it should be remembered that in some cases low hCG levels can be detected for up to four weeks after successful expulsion (4-8). Patients, who continue to have symptoms of pregnancy or experience uterine bleeding are likely to have retained POC (20).
For the evaluation of the various possible outcomes of treatment, i.e. complete abortion, incomplete abortion, missed abortion or continuing pregnancy, various methods are used. Besides clinical complaints and a gynecological examination, measurement of serum hCG and transvaginal sonography [TVS] are performed at the follow-up visit, within 1-3 weeks following treatment (21, 22).
Generally, bleeding after medical abortion lasts longer than after vacuum evacuation of an early gestation. If the patient is in good general condition, neither prolonged bleeding nor the presence of tissue in the uterus (as detected by ultrasound) is an unequivocal indication for surgical intervention. In most cases residual products of conception will be expelled during subsequent vaginal bleeding (11, 23-25). Surgical evacuation of the uterus may be carried out on the patient's request or if the bleeding is heavy or prolonged, causes anemia, or in evidence of infection. In the latter case, antibiotic treatment should be initiated (11, 26, 27).
However, there is no general agreement about the best means to evaluate the treatment outcome.
Creinin et al. (28) suggested that after complete abortion the β-hCG concentrations should decrease at least 48% within 24 hours. However, this decline does not guarantee that the abortion is complete. These investigators, (28), concluded that a patient with a declining serum β-hCG level of less than 50% over 24 hours is unlikely to have a complete abortion. Fiala et al. found that measuring serum β-hCG before treatment and at follow-up was more effective than ultrasound to confirm a successful abortion. They used 20% of the initial value as cut-off at follow-up and it allowed correct diagnosis in 98.5% of the patients with successful expulsion (11).
Rorbye et al. (19) found that absolute and relative β-hCG values as well as endometrial thickness were significantly higher in late failures than in successes after medical abortion, but none of these parameters was clinically useful as a diagnostic test in predicting late failure after medical abortion.
Follow-up ultrasound, may show thickened endometrium, sometimes with a heterogeneous structure even when the abortion was complete (11). The ultrasound findings may be equivocal, difficult to interpret and may possibly lead to unnecessary surgical interventions. Conservative management, i.e. waiting for the menstruation or a withdrawal bleeding proved, in many cases, to be safe (11).
Fiala et al. (11) concluded that the reliability of ultrasound examination in diagnosing successful expulsion was 89.8%.
The TVS follow-up included an evaluation of the uterine cavity contents and endometrial thickness. A well-defined endometrial line, with a maximum thickness of <15 mm, combined with absence of vaginal bleeding, were considered as complete abortion according to guidelines from the Royal College of Obstetricians and Gynecologists for spontaneous abortions (29). However, these cut-off values have never been prospectively validated (30).
Other authors concluded that most of the women regained normal menses without further surgical intervention, suggesting that remnants of trophoblastic tissue were spontaneously evacuated from the uterine cavity. (11, 31).
The objective of this study was to examine the effectiveness and predictive value of sonographic measurement of endometrial thickness during a follow up visit after medical abortion as an accurate predictor of the necessity of curettage for completion of pregnancy termination.
Material and Methods
The study was performed in the outpatient clinic of a tertiary public hospital- Rambam Medical Center. Data were prospectively collected from a cohort of women who had undergone medical TOP during the first seven weeks of gestation between January 2000 and December 2003. Four-hundred and one women who had TOP up to 49 days of amenorrhea, requesting medical abortion participated in this study.
A pretreatment transvaginal sonogram [TVS] was performed to confirm pregnancy and gestational age in all the participants. A crown-rump length (CRL) of 10 mm which is compatible with 49 days gestation was used as the upper limit for inclusion, (31-32). All patients signed an informed consent.
At the first visit, each patient received 600 mg mifepristone orally at the hospital. Patients returned 48 h later to receive one dose of orally administered, 400 μcg misoprostol, and was looked after at the hospital day care outpatient clinic for 6 hours. If no excessive bleeding or serious side effects occurred, the patient was released for home rest for the next two days, and returned for follow-up examination after 10-14 days. The TVS follow-up included an evaluation of the uterine cavity contents and measurement of endometrial thickness. Failures were generally noticed after the 2-week follow-up visit and defined by retained products of gestation, commonly presented with prolonged vaginal bleeding. Measurement of the endometrial thickness by ultra-sonography was performed before the surgical intervention. In the absence of any clinical complaint, patients were not invited for further follow-up.
Statistical analysis was done using chi square and t tests where appropriate.
Results
Four-hundred and one women requesting medical abortion up to 49 days of amenorrhea were included. 288 of the 401 patients (71.8%) completed the treatment and returned for follow-up and are included in the study. Patients who did not return to follow-up at the hospital outpatient clinic were defined as lost to follow-up (113/401) 28.2% (Table 1). Most of them were examined by their own gynecologist and were probably asymptomatic since they were not referred for surgical intervention.
Number of patients who have undergone TVS follow-up [F/U] after medical TOP [evaluable patients] vs. those who did not return for F/U.

Each patient has undergone a transvaginal sonography (TVS) 10-14 days after the misoprostol administration. Treatment was successful without the need for surgical intervention in 91.3% of the evaluated patients, (263/288). A total of twenty five (25/288) 8.7%, vacuum aspirations [D&E] had to be performed for retained POC and/or for hemorrhage. In 18 of these 25 patients, [72%] measurement of the endometrial thickness by ultrasonography was performed before the surgical interventions. In the absence of any clinical complaint, these patients were not invited for further follow-up.
Retained products of conception were histo-logically confirmed in 100% (18/.18) of the patients who had a D&E, indicating that the surgical interventions were appropriate.
All patients with measured endometrial width less than 11 mm (188 of 288, 65.3%), were considered to have had a successful medical procedure and no surgical intervention was performed. However, in 100 of 288 patients (34.7%) the measured endometrial width was > 11 mm, and in 18 of these 100 patients (18%), surgical intervention was performed. Thus, the failure of the medical TOP was 18/288 (6.25%) overall, 18% in patients with endometrium wider than 11 mm at the follow-up visit, vs. no failure at all, in those with endome-trium <11 mm, P < 0.001 (Tables 2, 3).
Number of patients in each group according to the endometrial width on TVS follow-up [F/U] after medical TOP, the number of patients who have undergone D&C in each group, and the failure rate.
Number of patients in each group according to the endometrial width on TVS follow-up [F/U] after medical TOP, the number of patients who have undergone D&C in each group, and the failure rate.

In 208 patients the endometrial width on the F/U visit was <12 mm. In 20 of these 208 patients (9.6%), the endometrial width was above 11 and below 12 mm; only one of these patients had undergone D&E 1/20 (5%). Thus, in 208 of 288 patients (72.2%) where the endometrial width was < 12 mm, the failure of medical TOP was 1/208 (0.48%). In 80/288 patients (27.8%) the endometrial width was >12 mm and in 17 ofthese 80 patients (21.3%) a surgical intervention had to be performed, for a calculated failure of the medical TOP of 17/288 (5.9%) (Tables 2, 3).
In 230 patients the endometrial width on the F/U visit was < 13 mm. In 22 of these 230 patients (9.5%) where the endometrial width was between 12 and 13 mm, surgical intervention was performed in 6/22 (27.3%) patients. In 230 of 288 patients (79.9%) where the endometrial width was < 13 mm, the failure of the medical TOP was 3% (6/230). In 58 of 288 patients (20.1%) the endometrial width was > 13 mm, for a calculated failure rate of the medical TOP of 18.9% (11/58) (Tables 2, 3).
In 250 patients the endometrial width on the F/U visit was < 14 mm. In 20 of these 250 (8%) the endometrial width was 13 to 14 mm, and surgical intervention was performed in two of them, (10%). In 250 of 288 patients (86.8%) with endometrial width < 14 mm, the failure of the medical TOP was 3.6% (9/250). In 38 of 288 patients (13.2%), the endometrium was >14 mm, and the failure rate of medical TOP in this group was 9/38 (23.7%). Thus, in 9 of the 18 patients (50%) who had undergone surgical intervention, the endometrium was > 14 mm on follow up examination 10-14 days after the medical abortion (Tables 2, 3).
Discussion
The diagnosis of a failed medical abortion usually leads to surgical intervention. Medical TOP is considered successful whenever complete abortion occurs without a need for surgical intervention, and no serious side effects occur. The need for surgical intervention due to sonographic findings after medical TOP is not clearly defined in the present literature.
We found in this study that in cases where on F/U TVS examination, an endometrial width of less than 11 mm is measured, there is no need of any surgical intervention to complete the medical abortion and conservative waiting to the next menstruation is recommended, unless the rare occasion of a symptomatic patient (massive or prolonged vaginal bleeding). Whenever the endometrium is wider than 11 mm on the follow-up visit after medical TOP, 18% of the patients may need D&E to complete the procedure. This risk is stable up to an endometrial thickness of 14 mm. Patients with endometrial thickness above 14 mm have 50% risk of surgical intervention for completion of the procedure.
In recent years, several modalities for follow-up patients after medical TOP have been suggested. Rorbye et al. (15) concluded that the clinical presentation is more accurate than sonographic measurement of the endometrial thickness for defining failure of medical TOP, 14-30 days after treatment. Extended follow-up, in this study (15), was linked to higher rate of surgical intervention. Cowett et al. (27) found that the range of endometrial thickness after medical TOP was wide, with a significant overlap between the groups and they recommended that clinicians intervene not only when a persistent gestational sac is seen on TVS, but also on the basis of compelling clinical indications. Fiala et al. (11) suggested that the sonographic findings on follow-up were sometimes difficult to interpret and may lead to unnecessary surgical intervention, and found that serum βHCG was more effective in the follow-up after medical abortion. Creinin et al. (33) found no relationship between increased endometrial thickness and the need for surgical intervention in women treated with misoprostol for early pregnancy failure and concluded that a thickened endometrial lining after miscarriage is a normal finding, and suggested that only clinical signs and symptoms rather than endometrial thickness should guide treatment decisions.
There is no consensus regarding the criteria for follow-up and success, and the indications for surgical intervention are equivocal (19). Reasons for curettage usually have included retained intrauterine pregnancy, or massive bleeding. Failures are generally diagnosed after the 2-week follow-up visit and are defined by retained products of gestation, commonly presenting with prolonged vaginal bleeding. In the absence of any clinical complaint, these patients were not invited for further follow-up (15).
It is expected that the intrauterine debris presented after medical abortion will be expelled in the next menstruation (24).
Luise et al. (29) concluded that in the absence of vaginal bleeding, the sonographic criteria could confirm complete abortion when endometrial thickness was <15 mm. Ultrasonography can be used to advise patients on the likelihood that their miscarriage will complete spontaneously within a given time.
The cut-off values have never been prospectively validated (15). A wide variation in endometrial thickness is seen after expulsion of the gestational sac, and that the thickness generally decreases with time.
Machtinger et al. (24) found that the TVS criteria had 100% sensitivity and 98.7% specificity for the recognition of retained products of conception after medical termination of pregnancy in all women who completed the follow-up (24). The positive and negative predictive values were 91.3% and 100%, respectively. TVS can increase the detection rate of retained products of conception after medical termination of pregnancy (24).
Wong et al. (34) reported almost the same about transvaginal sonography. It had a sensitivity rate of 100% and a specificity rate of 80% in the detection of residual products of conception, after first-trimester spontaneous abortion (34).
Markovitch et al. (31) described the sonographic appearance of the uterine cavity after mifepristone and found an echogenic mass with well-defined borders with or without Doppler flow signals up to 2 weeks after treatment. They (31) concluded that this intrauterine abnormality may represent normal physiologic response following medical abortion with mifepristone.
Many authors suggested that D&C should be avoided unless clinical symptoms or signs necessitate this procedure. (11, 26, 35, 36).
We conclude, therefore, that the measurement of the endometrial thickness is a good predictor of failure of the medical abortion and may prevent an unnecessary surgical intervention in patients whose endometrial width on F/U is below 11 mm. However, in cases where the endometrium is wider than 11 mm the sonographic FU should be weekly continued.
Footnotes
Disclosure
The authors report no conflicts of interest.