
Abstract
Background
Extended in vitro embryo culture and blastocyst transfer have emerged as essential components of the advanced reproductive technology armamentarium, permitting selection of more advanced embryos considered best suited for transfer.
Aim of study
The aim of this study was to compare between cleavage stage and blastocyst stage embryo transfer in patients undergoing intracytoplasmic sperm injection, and to assess the role of assisted hatching technique in patients undergoing blastocyst transfer.
Patients and methods
This study was carried out on two groups. Group I: 110 patients who underwent 120 cycles of intracytoplasmic sperm injection with day 2-3 embryo transfer—for unexplained infertility or male factor within the previous 3 years. Their data obtained retrospectively from medical records.
Results
Comparison between both groups as regards the reproductive outcome showed a significant difference in pregnancy and implantation rates, both being higher in group II (P < 0.05) Comparison between both subgroups as regards the reproductive outcome showed a highly significant difference in pregnancy and implantation rates, both being higher in Group IIa (P < 0.01). There was also a significantly higher rate of multiple pregnancies among Group IIa (P < 0.05).
Conclusion
Blastocyst transfer is a successful and improved alternative for patients with multiple failed in vitro fertilization attempts, associated with a significant increase in pregnancy and implantation rates. Furthermore, laser assisted hatching increases implantation and clinical pregnancy rates.
Introduction
There are many variables of success in an in vitro fertiliztion (IVF) embryo transfer (ET) cycle. The implantation potential of good quality embryos remains low during IVF, despite advances in ovarian stimulation regimens, the method of assisted fertilization and improved culture conditions. 1
The optimal time to perform embryo transfer (ET) had remained controversial. Cleavage stage (day 2 or 3) ET was generally used in IVF and became established as the usual approach. This intentional placement of a day 2 or 3 embryo directly into the uterine cavity was recognized as non-physiologic, but there was little to offer as an alternative due to the inability to sustain human embryos in culture to the blastocyst stage. 2 The rationale for blastocyst culture is to improve both uterine and embryonic synchronicity. 3
Recent advances in the understanding of nutrient requirements of embryos, and the improvements in culture media 4 have led to the possibility of extending their culture from the standard procedure of 2-3 days (early cleavage embryo transfer) to 5-6 days (blastocyst culture). The adoption of extended embryo culture to the blastocyst stage during the last decade has entailed new challenges. 5
Extended in vitro embryo culture and blastocyst transfer (BT) have emerged as essential components of the advanced reproductive technology armamentarium, permitting selection of more advanced embryos considered best suited for transfer. 6 BT should enable transfer of fewer but higher quality embryos resulting in increased implantation rates. 7
However, despite this technical progress in IVF procedure, embryo implantation rate remains low. Failure of implantation and conception may result from an inability of the blastocyst to escape from the zona pellucida. Artificial disruption of this coat is known as assisted hatching (AH) and has been proposed as a method for improving the success of assisted conception. 8
Aim of the Work
The aim of this study was to compare between cleavage stage and blastocyst stage embryo transfer in patients undergoing intracytoplasmic sperm injection (ICSI), and to assess the role of assisted hatching technique in patients undergoing BT.
Patients and Methods
This study was carried out on two groups.
Unexplained infertility was defined as: patients with at least one year of infertility, all patients had patent fallopian tubes detected by hysterosalpingography and/or laparoscopy, normal ovulation confirmed by midluteal progesterone level more than 5 ng/ml and normal hormonal profile (FSH, LH, prolaactin and TSH) in the early follicular phase and all the male partners had a normal semen analysis according to WHO criteria. 9
Patients of Group I were selected from medical records of Ain Shams University Maternity hospital, Assisted Reproduction Technology Unit while patients of Group II were recruited from multi-center local private outpatient settings.
Any patients with infertility due to ovarian, tubal or uterine factors were excluded from the study.
An informed consent was obtained from all participants and the study was approved by the medical ethics committee of Ain Shams University Hospital.
For patients in Group I
Evaluation of their medical records was done, with emphasis on epidemiological data, basal hormonal profile, protocol of ovulation induction, number and quality of oocytes retrieved, number of oocytes injected, number of fertilized oocytes, and the number and quality of embryos transferred on day 2-3. The pregnancy and implantation rates were obtained.
For patients in Group II
Full history taking and thorough clinical examination was done.
All patients had an
Basal hormonal profile: (day 2-3 of menstrual cycle) follicle stimulating hormone (FSH), leutinizing hormone (LH), prolactin hormone (PRL), Thyroid stimulating hormone (TSH), Estradiol (E2), anti-mullerian hormone (AMH) and total testosterone.
Pelvic ultrasound: for exclusion of ovarian and uterine pathology
Hysterosalpingogram and/or laparoscope: for tubal patency and exclusion of any pelvic pathology.
Semen analysis of the patient's partner. Where abnormal results were defined in reference to the World Health Organization Criteria. 10
Controlled ovarian hyperstimulation
Using long protocol of ovulation induction. To ensure regularity of the cycle, oral contraceptive pills (OCPs), Yasmin (Scherring AG, Germany) was started on 1st day of the preceding cycle, on day 18 of the OCPs, gonadotrophin releasing hormone (GnRh) analogue, Triptorelin Acetate 0.1 mg (Decapeptyl, Ferring, Kiel, Germany) SC injection was started and continued daily. After completion of OCPs and menstruation, serum estradiol (E2) was measured on day 2 of the cycle to ensure complete suppression of pituitary gland, and then human Menopausal Gonadotrophin (hMG) (Menogon, Ferring, Kiel, Germany) in a daily dose of 225 IU intramuscular injection was started on 3rd day. Transvaginal ultrasound folliculometry was stared on day 5 of stimulation using micro-convex endocavity probe 6CV1, 5-8 MHz (Mindray DC3 ultrasound, China), and every other day till at least 3 graffian follicles reached >18 mm when triggering of ovulation using human chorionic gonadotrophin (HCG) (Choriomon, IBSA Institut Biochimique SA, Switzerland) 10,000 IU were injected intramuscularly. Thirty six hours later, ultrasound guided oocyte pick up was done. Semen samples were collected by masturbation. Sperm injection was done and developed embryos were incubated in suitable culture media for 5 days till expanded blastocyst stage.
Randomly on day 5, through a computer generated program, laser assisted hatching was done for blastocysts of 23 patients. Balstocyst transfer was carried out on day 5. After BT, luteal phase support started using progesterone vaginal pessaries 400 mg (Cyclogest® Vaginal Pessaries, Noristan Limited, Waltloo, Pretoria) for 14 days. Fourteen days post embryo transfer; patients undertook a blood pregnancy test. Only women with a β-HCG titre 25 IU/mL were considered positive. At seven weeks gestation, clinical pregnancy was confirmed with visible fetal heart beats by ultrasound.
Technique of laser assisted hatching
A 1480-nm diode laser in a computer-controlled non-contact mode was used for laser hatching (Zilos-tk™ Hamilton Thorne Biosciences, Beverly— Massachusttes, USA). The Zilos-tk™ is attached to an Olympus IX-71 (Olympus, Tokyo, Japan) inverted microscope below the objective turret. Quarter laser-assisted hatching (Q-LAH) was applied to each embryo as described previously. 11 The thinning of the zona pellucida by laser shots was initiated at one point and continued until 25% of the zona pellucida was drilled.
Statistical analysis
Data were presented as mean + SD, frequencies (number of cases) and relative frequencies (percentage) when appropriate. All data were transferred to IBM cards using IBM personal computer, analyzed with statistical program for social science “SPSS V11.0, SPSS Inc., Chicago, IL, USA”. Student t-test was used for comparison between two normally distributed quantitative data while Mann-Whitney U-test was used for comparison between two non-normally distributed data. For comparing categorical data, Chi square (X2) or Fischer exact test were used. P > 0.05 considered non significant, P < 0.05 considered significant and P < 0.01 considered highly significant
Results
This study included two groups.
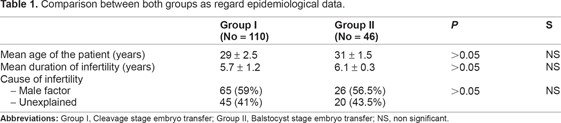
Comparison between both groups as regard epidemiological data.
Comparison between both groups as regards basal hormonal profile.

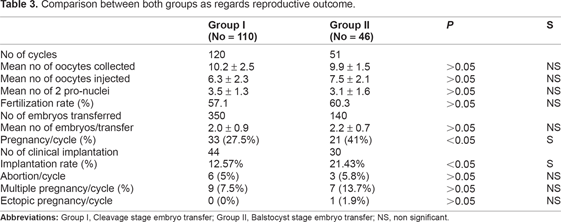
Comparison between both groups as regards the reproductive outcome showed a significant difference in pregnancy and implantation rates, both being higher in group II (P < 0.05) (Table 3).
Comparison between both groups as regards reproductive outcome.
Patients in Group II were further subdivided into 2 equal groups; Group IIa (23 patients), who had laser assisted hatching (LAH) and Group IIb (23 patients), which did not have assisted hatching (No-LAH). There was no significant difference between both groups as regards age, duration or cause of infertility, and basal hormonal profile (Tables 4 and 5).
Comparison between both subgroups as regards epidemiological data.

Comparison between both subgroups as regards basal hormonal profile.

Comparison between both subgroups as regards the reproductive outcome showed a highly significant difference in pregnancy and implantation rates, both being higher in Group IIa (P < 0.01). There was also a significantly higher rate of multiple pregnancies among Group IIa (P < 0.05) (Table 6).
Comparison between both subgroups as regards reproductive outcome.

Discussion
For infertile patients undergoing in vitro fertilization (IVF), blastocyst transfer (BT) brings a number of potential advantages over traditional cleavage-stage embryo transfer. Because day 2-3 embryos normally should transit the oviduct only, their direct exposure to an intrauterine microenvironment is physiologically inappropriate. This mismatch is obviated by BT. Moreover; the nutritional milieu inside the fallopian tube is not the same as within the endometrial compartment, a feature possibly antagonistic to implantation when a day 2-3 embryo is placed directly within the uterus. Delaying transfer to day 5-6 may also improve reproductive outcome by reducing risk of embryo expulsion. 2
In this study, 110 patients who underwent 120 cycles of intracytoplasmic sperm injection (ICSI) (Group I) with day 2-3 embryo transfer, were compared with 46 age matched infertile female patients undergoing 51 ICSI cycles with BT. Comparison between both groups as regard age, duration or cause of infertility, and basal hormonal profile, showed no statistical significance. The results showed a significant difference (P < 0.05) between group I and II in pregnancy rates (27.5% vs. 41%) and implantation rates (12.57% vs. 21.43%) respectively.
Similar studies have shown that blastocyst stage embryo transfer has higher pregnancy rates when compared to cleavage stage transfer. Better embryo selection and a more physiologic stage of transfer are possible explanations. 12
Many papers compare the pregnancy rate of blastocyst transfers to that of the cleavage stage.13,14 It has been documented that blastocyst transfer has a higher implantation rate than that of cleavage stage transfer and is effective for cases with repeated implantation failures. 15 In one study it was stated that day 6 embryo transfers resulted in significantly higher ongoing pregnancy and implantation rates compared with day 3 embryo transfers (41.1% and 23.6% vs. 50.1% and 38.1% respectively). No differences were found in terms of multiple gestations. 16
As the benefits of BT continue to be widely debated,17,18 the reality of clinical practice is that not all patients are good candidates for BT. This is because it is possible that after five days in culture, no embryo will survive to the blastocyst stage and the IVF cycle will be cancelled. Moreover, selection criteria for BT are variable and there is no consensus on the appropriateness of BT protocols applied specifically to patients with multiple unsuccessful IVF cycles. 19
In this study, there was no statistical significant difference (P > 0.05) between both groups as regards multiple pregnancies, although a higher percentage was recorded among Group II (13.7%) as compared to Group I (7.5%).
One potentially negative aspect of human blastocyst culture has been the observation that monozygotic twinning may occur at a higher rate with extended in vitro embryo culture, 20 compared to traditional day 3 embryo transfer.
In this study no monozygotic twins were recorded. Considerable speculation has been offered to explain why monozygotic twins might occur more often in assisted reproduction in general, and more specifically, in extended culture for BT. Some investigators have theorized that prolonged in vitro culture could be associated with alternation of the zona pellucid and the hatching process. 21
In contrast, more recent research has concluded that concerns about monozygotic twinning should not be a factor to discourage extended embryo culture for blastocyst transfer, considering the higher pregnancy rate and lower number of transferred embryos in BT cycles compared to embryo transfers performed at earlier developmental stages. 22
Although it has been documented that BT may raise the rate of monozygotic twins, other studies on the reproductive outcomes among patients who had embryo transfers noted that maintaining embryos in laboratory culture until the blastocyst stage has not been shown to lead to more pregnancies than regular IVF. 4
The poor implantation rate after the transfer of apparently normal looking embryos is one of the unsolved problems incurred in IVF. Besides intrinsic embryo abnormalities or defective uterine receptivity, hatching failure could also partly explain the low implantation rate in IVF. It has been hypothesized that assisted hatching (AH) may enhance embryo implantation, not only by mechanically facilitating the hatching process, but by also permitting early embryo endometrium contact. 11
AH has been advocated as a means of assisting the natural hatching process and enhancing implantation. 23 It is based on the presumption of creating artificial openings (slits or holes) in the zona pellucida to assist the in vivo hatching process of embryos. This technique has been shown to increase implantation and pregnancy rates.
In this study, patients in Group II were further subdivided into 2 equal groups; Group IIa (23 patients), which had laser assisted hatching (LAH) and Group IIb (23 patients), which did not have assisted hatching. Comparison between both subgroups as regards the reproductive outcome showed a highly significant difference in pregnancy and implantation rates, both being higher in Group IIa (P < 0.01). There was also a significantly higher rate of multiple pregnancies among Group IIa (P < 0.05).
In contrast however, other studies have stated that although the difference in clinical pregnancy rate had increased by AH, yet it did not reach statistical significance. 24 In addition another randomized study, failed to show any beneficial effect of LAH on implantation and pregnancy rates following the transfer of thawed embryos. 25
In conclusion, BT appears to be a successful and improved alternative for patients with multiple failed IVF attempts. LAH increases implantation and clinical pregnancy rates. Bearing in mind that blastocyst culture may end with no embryos for transfer, and the difficult technique of LAH, these options should be offered cautiously to the patients and proper selection is mandatory. Finally, it will be important to undertake further research emphasizing embryo and blastocyst morphology to better define which patients are best suited for BT, and how in vitro culture conditions may be optimized.
Disclosure
Author(s) have provided signed confirmations to the publisher of their compliance with all applicable legal and ethical obligations in respect to declaration of conflicts of interest, funding, authorship and contributorship, and compliance with ethical requirements in respect to treatment of human and animal test subjects. If this article contains identifiable human subject(s) author(s) were required to supply signed patient consent prior to publication. Author(s) have confirmed that the published article is unique and not under consideration nor published by any other publication and that they have consent to reproduce any copyrighted material. The peer reviewers declared no conflicts of interest.