
Abstract
Objective
To scrutinize the assumed association between chronic periodontal disease and preterm low birth weight (PTLB) infants.
Design
Prospective study.
Setting
Tanta University Hospital.
Patients
The study incorporated 200 pregnant women in the first stage of labor of a single baby with intact membranes. A hundred women had definite preterm labor and delivered, later live infants whose birth weight were < 2500 g and 100 women with full term labor and delivered, later live infants weighting ≥2500 g.
Intervention
All patients included in the study were subjected to history taking, general, obstetrical examination and periodontal evaluation. The levels of IL-6 and TNF-α were measured in gingival cervicular fluid, maternal serum and amniotic fluid using ELISA technique.
Results
A significant association between chronic periodontal disease and preterm low birth weight infants.
Conclusion
Screening of pregnant women chronic periodontal disease seems to be a helpful prediction and consequently prevention of preterm labour.
Keywords
Introduction
Despite the many advances in medicine, the rate of preterm birth has not significantly decreased over the past several decades. Consequently, the identification of risk factors for preterm birth which are amenable to intervention would have far-reaching and long-lasting effects. 1
There is emerging evidence of a relationship between periodontal health and adverse pregnancy outcomes, particularly preterm birth/preterm low-birth-weight (PTLB) infants. Preterm birth is defined as delivering at less than 37 completed weeks of gestation, whereas preterm low-birth-weight infants are born less than 37 weeks and weigh less than 2500 g. 2
The aim of this study was to scrutinize the assumed association between periodontal disease and preterm PTLB infants.
Patients
This study included 200 pregnant women with a singleton gestation recruited from women admitted to the labor suite of Obstetrics department of Tanta University Hospital during the period from October 2006 to September 2009. The enrolled women were presented in the first stage of labor with intact membranes. A hundred of them had definite preterm labor and one hundred with full term labor. The subjects were subdivided into two equal groups:
Methods
All patients included in the study were subjected to history taking, general and obstetrical examination.
Periodontal evaluation includes review of a person's medical and dental history, followed by a clinical examination. 3 The clinical examination includes ascertaining probing depths, percentage of bleeding on probing depth 4 and the Community Periodontal Index of Treatment Needs (CPTIN) Score. 5 CPITN ranged from 0-4. 0 = Healthy; 1 = Bleeding on probing; 2 = Supra and sub-gingival calculus; 3 = Shallow pockets (3.5-5.5 mm); and 4 = Deep pockets (>6 mm), using a calibrated periodontal probe was quantified.
An informed consent was obtained from every case after counseling.
The levels of IL-6 and TNF-α were measured in gingival cervicular fluid, maternal serum and amniotic fluid using enzyme-linked immunosorbent assay (ELISA).
TNF-α levels were determined using ELISA test (Bender Med Systems, Human TNF-α).
For statistical analysis, the range, mean and standard deviation were calculated. The difference between two means was statistically analyzed using the students (t) test. Mann-Whitney test (Z) was performed to test differences in mean values between groups when the observations were not found to follow the normal distribution Pearson's correlation coefficient (r) was calculated to test the association between two variables. Tests of reliability of each marker were calculated. Significance was adopted at P < 0.05 for interpretation of results of tests of significance. 6
Results
The control and patients group were statistically comparable regarding demographic characteristics, age and gravidity.
The mean value of the gestational age was 32.82 ± 1.96 weeks in patient's group compared with 39.34 ± 1.15 weeks in the control group. The P value (0.001) shows significant statistical difference both groups regarding the gestational age.
Positive and negative predictive values of the studied markers. The CPITIN score, bleeding depth and % of bleeding on probing in the studied groups. IL-6 in gingival cervicular fluid, serum IL-6 and amniotic fluid IL-6 in patients and control groups. TNF-α in gingival cervicular fluid, serum and amniotic fluid in patients and control groups. Correlation between Infant birth weights in grams.
Significant. It is apparent that there is a significant negative correlation between IL-6 in GCF, IL-6 in AF, TNFα in GCF, TNFα in AF and infant neonatal birth weight.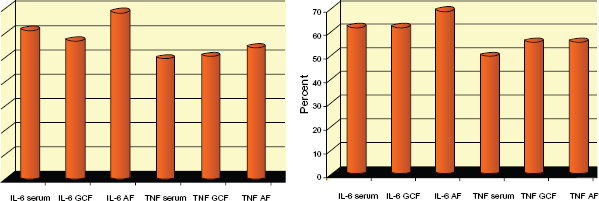



The mean value of the infant neonatal birth weight was 1996.68 ± 296.33 grams in patient's group compared with 3303.93 ± 417.11 grams in the control group. The P value (0.001) shows significant statistical difference in patients and control groups regarding the infant birth weight.
Discussion
The hypothesized connection between periodontal infection and adverse pregnancy outcome is not recent. Galloway in 1931 suggested a deleterious relationship between periodontal disease and pregnancy. After a study in which he had full-mouth x-rays on all prenatal patients and subsequently treated those who demonstrated radiographic symptoms of chronic infection, he concluded that ‘routine care of pregnancy should include a full-mouth x-ray of the patient's teeth as a part of the first examination’. 7
In the contemporary investigation we found a significant connection between periodontal disease and the incident of premature labour. At labour, the mean gestational age among women with periodontal disease was 32.82 ± 1.96 weeks compared with 39.34 ± 1.15 weeks in the control group. Similarly, we found an important relationship between periodontal disease and neonatal birth weight. The mean value of the neonatal birth weight was 1996.68 ± 296.33 grams in patient's having periodontal disease compared with 3303.93 ± 417.11 grams in the control group.
The mechanism by which maternal infection mediates early delivery is unclear. Genetic variation in response to these infections may play a role in the risk for prematurity. 8 A solid body of evidence indicates that cytokines play a central role in the mechanisms of inflammation/infection-induced preterm parturition.9,10 Evidence in support of the participation of interleukins includes: 1) production by human decidua in response to bacterial products, 2) increased concentration and bioactivity in the AF of women with PTL and infection, 11 3) stimulation of myometrial contractions, and 4) induction of PTL and delivery by administration to pregnant animals, which was blocked by the administration of an antagonist. 12
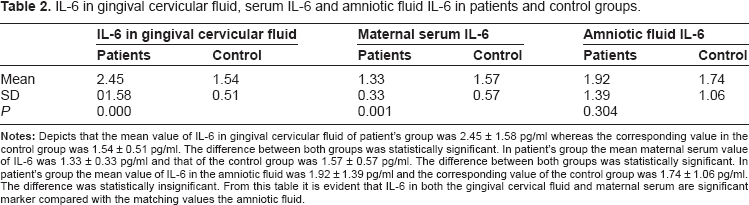
The results of the present effort revealed that IL-6 in the gingival cervical fluid is the only significant inflammatory marker for the occurrence of premature labour whereas IL-6 in maternal serum and amniotic fluid are of insignificant importance.
Interleukin-6 concentrations in amniotic fluid are considered a marker of intra-amniotic inflammation frequently associated with microbiological infection in the amniotic fluid or the chorioamniotic space. 13 Romero et al reported the results of a case control study in which IL-6 determinations were conducted in stored fluid of patients who had a pregnancy loss after a mid-trimester amniocentesis and a control group who delivered at term. Patients who had a pregnancy loss had a significantly higher median amniotic fluid IL-6 concentration than those with a normal outcome. 14 Similar findings were reported by Wenstrom et al. 15 Of note is that maternal plasma concentrations of IL-6 were not associated with adverse pregnancy outcome.
Gestational age in weeks.

Significant. It is obvious that there is a significant negative correlation between IL-6 in GCF, TNFα in GCF, TNFα in AF and gestational age.
Reliability of different study variables for diagnosis of low birth weight.

Significant. It is observable that estimation of maternal serum IL-6 in GCF, IL-6 in GCF had a significant importance in prediction of low birth weight.
Preterm birth is associated with elevated production of pro-inflammatory cytokines such as TNFα at the maternal-foetal interface. 16
In agreement with that, we found significant higher values TNF-α in gingival cervicular fluid and maternal serum and amniotic fluid of patient's with periodontal disease and premature labour compared with controls.
In that concern, there is evidence supporting the role of tumour necrosis factor-alpha (TNF-α) in mechanisms of preterm parturition includes: 1) TNF-α stimulates prostaglandin production by the amnion, decidua and myometrium, 2) human decidua can produce TNF-α in response to bacterial products, 17 3) AF TNF-α bioactivity and immunoreactive concentrations are elevated in women with PTL and intra-amniotic infection, 17 4) in women with preterm PROM and intra-amniotic infection, TNF-α concentrations are higher in the presence of labour, 18 5) TNF-α application in the cervix induces changes that resemble cervical ripening, 19 and 6) TNF-α can induce preterm parturition when administered systemically to pregnant animals.
It is unclear, whether or not there is also enhanced production of TNFα in response to bacteria that are more frequently associated with preterm birth such as genital mycoplasmas that lack LPS but contain other macrophage stimulating factors.20,21 Bacteria are thought to stimulate maternal immune cells to produce pro-inflammatory cytokines as a part of the host response to infection. 22 Although many proinflammatory cytokines are associated with preterm birth in clinical cases, TNFα appears to be especially important. Administration of this cytokine causes preterm birth in mice, 23 and administration of antibodies to TNFα blocks LPS-induced preterm birth in mice. 24
Lastly, we conclude that there is a significant correlation between chronic periodontal disease and PLBW and inflammatory markers; maternal serum IL-6 in GCF, IL-6 in GCF have a significant predictive value.
Publish with Libertas Academica and every scientist working in your field can read your article
“I would like to say that this is the most author-friendly editing process I have experienced in over 150 publications. Thank you most sincerely.”
“The communication between your staff and me has been terrific. Whenever progress is made with the manuscript, I receive notice. Quite honestly, I've never had such complete communication with a journal.”
“LA is different, and hopefully represents a kind of scientific publication machinery that removes the hurdles from free flow of scientific thought.”
Available to your entire community free of charge
Fairly and quickly peer reviewed
Yours! You retain copyright
Footnotes
This manuscript has been read and approved by all authors. This paper is unique and is not under consideration by any other publication and has not been published elsewhere. The authors and peer reviewers of this paper report no conflicts of interest. The authors confirm that they have permission to reproduce any copyrighted material.