
Abstract
Objective
Accurate and timely diagnosis of rupture of membranes (ROM) is imperative to allow for gestational age-specific interventions. This study compared the diagnostic performance characteristics between two methods used for the detection of ROM as measured in the same patient.
Methods
Vaginal secretions were evaluated using the conventional fern test as well as a point-of-care monoclonal/polyclonal immunoassay test (ROM Plus®) in 75 pregnant patients who presented to labor and delivery with complaints of leaking amniotic fluid. Both tests were compared to analytical confirmation of ROM using three external laboratory tests. Diagnostic performance characteristics were calculated including sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), and accuracy.
Results
Diagnostic performance characteristics uniformly favored ROM detection using the immunoassay test compared to the fern test: sensitivity (100% vs. 77.8%), specificity (94.8% vs. 79.3%), PPV (75% vs. 36.8%), NPV (100% vs. 95.8%), and accuracy (95.5% vs. 79.1%).
Conclusions
The point-of-care immunoassay test provides improved diagnostic accuracy for the detection of ROM compared to fern testing. It has the potential of improving patient management decisions, thereby minimizing serious complications and perinatal morbidity.
Keywords
Introduction
Spontaneous rupture of membranes (ROM) can occur at any gestational age and presents a particularly serious clinical problem if it occurs prior to 37 weeks gestation, where it is responsible for 20%-40% of preterm births.1–3 Thus, accurate and timely diagnosis of ROM is imperative to inform and guide gestational age-specific interventions to optimize perinatal outcomes and reduce the risk of serious complications, including preterm delivery and infections such as chorioamnionitis and neonatal sepsis.4–6 An incorrect diagnosis of ROM (ie, false-positive test) can also have serious clinical ramifications such as the initiation of unnecessary obstetrical interventions that may include hospitalization, administration of medications, and even iatrogenic premature delivery. 7
When ROM is suspected, the diagnosis is conventionally made using the sterile speculum examination to identify leakage or pooling of amniotic fluid, coupled with a microscopic evaluation of a collected specimen for evidence of ferning/crystallization, commonly referred to as the fern test, and pH testing of the fluid with nitrazine test paper.5,8,9 While this approach has remained the standard of care for decades, the results can be equivocal, especially when more than an hour has elapsed since ROM. 10 Additionally, the sterile speculum examination is both subjective and labor intensive and has been shown to have inadequate diagnostic performance characteristics for the accurate detection of ROM.5,11–14
To address this diagnostic dilemma, there has been a concerted effort to develop and commercialize rapid, point-of-care immunoassay tests that accurately detect proteins found in high concentrations in amniotic fluid but at extremely low background concentrations in cervicovaginal secretions. 15 The first generation of these tests used a monoclonal antibody approach focusing on insulin-like growth factor binding protein-1 (IGFBP-1, aka placental protein 12) and placental alpha microglobulin-1 (PAMG-1).16–21 Enthusiasm about this point-of-care approach for the more accurate diagnosis of ROM has led to the recent development of a combined monoclonal/ polyclonal antibody immunoassay to detect two different proteins found in amniotic fluid at high concentrations. 22 The current study directly compares this novel immunoassay with the traditional fern test, each measured in the same patient with suspected ROM.
Materials and Methods
This study compared the diagnostic performance characteristics between two methods used for the detection of ROM at a single institution: (1) the fern test and (2) a monoclonal/ polyclonal immunoassay test (ROM Plus®; Clinical Innovations). Seventy-five (75) pregnant patients between 14 and 41 weeks gestation presenting with a complaint of ROM were involved in this study. According to hospital protocol, a clinician who had demonstrated competency in assessment of ROM performed a standard sterile speculum examination upon the patient's presentation. A swab was first obtained from the vaginal pooling if present or from the vault if not, and a slide was prepared for conventional clinical laboratory evaluation of crystallization (fern test). A second swab was then collected from the vagina for evaluation using the ROM Plus® immunoassay test. The slides prepared for the fern test and the ROM Plus® test were sent to the hospital laboratory for interpretation. Both tests were compared to an analytical confirmation of ROM using an independent reference laboratory.
The methodological details of the monoclonal/polyclonal antibody assay test have been published previously. 22 Briefly, the ROM Plus® is a point-of-care test that accurately detects the presence of two amniotic fluid proteins, IGFBP-1 and alpha-fetoprotein (AFP). The threshold of detection for this assay is 5 ng/mL for IGFBP-1 and 150 ng/mL for AFP. The concentration of these proteins in amniotic fluid is between 10,500 and 350,000 ng/mL for IGFBP-1 23 and from 2,800 to 26,000 ng/mL for AFP. 24
Collected samples were used to establish analytical confirmation of ROM using an external reference laboratory using a composite of three tests: an enzyme-linked immuno-sorbent assay (ELISA) quantification of IGFBP-1 and AFP, a competitive rapid immunoassay test for the diagnosis of ROM (Amnisure®; Qiagen) that detects the presence of PAMG-1 protein, and a repeat of the ROM Plus® test. The final diagnosis of ROM was based on all three analytic confirmation sources being positive. Conversely, the final diagnosis of intact membranes (no ROM) was based on all three analytic confirmation sources being negative.
Both the clinicians and patients were blinded to the results of the ROM Plus® test. Clinical decision making was based on the results of the fern test, physical examination, and the clinical course.
Diagnostic performance characteristics were calculated for each test, including sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), and accuracy (ie, overall agreement). 25 Statistical differences between the test measurements were computed using McNemars exact test, two-sided.
The study protocol and methodology were reviewed by the Memorial Healthcare System IRB. The study design was considered to be an internal validation study, and formal IRB approval was not required as clinical decision making was not altered by the ROM Plus® test results. The research complied with the principles of the Declaration of Helsinki.
Results
Table 1 provides the between-test comparison data for all 75 patients. Approximately 79% (11 of 14) of positive results were in agreement between the two tests. Similarly, only 80% (49 of 61) of negative results were concordant between the fern and ROM Plus® tests. The overall lack of concordance between the test measurements was statistically significant (P = 0.035).
2 × 2 data comparison: RQM plus® vs. fern test.

Sufficient quantities of vaginal fluid were available for 67 patients (89%) to allow analytical confirmation with the three composite measurements. Comparing the ROM Plus® results with the confirmatory analytical confirmation tests resulted in overall excellent diagnostic accuracy with a sensitivity of 100% and a specificity of 94.8% (Table 2). The corresponding PPV and NPV for the ROM Plus® were 75% and 100%, respectively. Only three measurements were discordant between the ROM Plus® test and the analytical confirmation, resulting in an overall accuracy of 95.5% (64 of 67).
Diagnostic performance characteristics: ROM Plus® vs. analytical confirmation

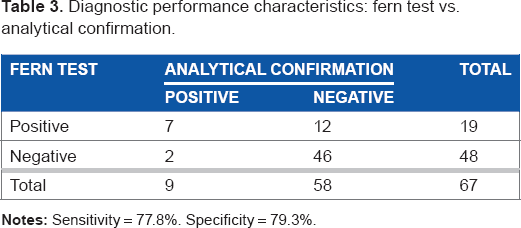
Comparing the conventional fern test with the confirmatory analytical confirmation tests resulted in lower diagnostic accuracy with a sensitivity of 77.8% and a specificity of 79.3% (Table 3). The corresponding PPV and NPV for the fern test were 36.8% and 95.8%, respectively. Fourteen measurements were discordant between the fern test and the analytical confirmation, resulting in an overall accuracy of 79.1% (53 of 67).
Diagnostic performance characteristics: fern test vs. analytical confirmation.
As shown in Table 1, there were 15 cases that had discordant results between the two test measurements. Thirteen of these patients had analytical confirmation, and their individual results are provided in Table 4.
data for discrepant patients.

Discussion
Previously published results have shown robust diagnostic accuracy (sensitivity 99% and specificity 91%) for the ROM Plus® and low specificity (72%) for the fern test. 22 The findings from the current study corroborate and extend these results and suggest that fern testing is inferior to ROM Plus®, especially with respect to detecting true-negative results. The high level of diagnostic accuracy achieved with the ROM Plus® is particularly important in cases of equivocal ROM as nearly one-quarter of all patients ultimately diagnosed with ROM do not present with overt clinical evidence of ruptured membranes on initial presentation. 8 Indeed, in the current study, over 95% of the ROM Plus® results corresponded with the true analytical confirmation. This excellent level of concordance is in sharp contrast with the fern test that incorrectly classified specimens more than 20% of the time compared with external confirmatory tests.
The high sensitivity consistently achieved with the ROM Plus® test is due, in large part, to the unique monoclonal/ polyclonal antibody approach where the polyclonal antibodies combine with multiple (8-12) amino acid peptides contained in the 259 full-length IGFBP-1 protein chain, while the monoclonal tests combine with a single epitope site. This may provide an advantage over other currently available rapid immunoassay tests that rely on a single monoclonal antibody.
The limitations of the current study include the use of only one comparator, the fern test, which has historically provided inadequate diagnostic accuracy for ROM. 14 Nevertheless, microscopic evaluation of vaginal fluid for evidence of crystallization using the fern test remains a common and standard approach, despite the known shortcomings. 1 Another limitation is the choice of the confirmatory test. The gold standard to confirm ROM is to inject indigo carmine into the amniotic sac during amniocentesis and then assess whether any blue fluid is visibly leaking from the cervical or pooling in the vaginal vault. 5 As amniocentesis is an invasive procedure and was not medically indicated in these patients, this confirmation was not performed. The combined use of the ELISA for IGFBP-1 and AFP, another immunoassay for PAMG-1, and repeating the ROM Plus® was considered the best alternative to indigo carmine injection. The validity of the confirmatory process is limited by the technical performance of these assays. Finally, while the current study does represent pragmatic, real-world utilization of these tests, it was conducted at a single center without a rigorous methodological protocol.
This unique monoclonal/polyclonal immunoassay can be performed easily and rapidly at the patients’ bedside by a variety of caregivers without the need for a speculum examination. Indeed, it may be particularly useful in low resource settings where rapid, point-of-care testing has been shown to be more accurate and cost-effective than a sterile speculum examination. 21 While the results should not be interpreted in isolation, it is an ideal addition to the current diagnostic armamentarium for accurately detecting ROM and for guiding correct clinical management decisions to improve obstetrical and neonatal outcomes.
Author Contributions
Designed and conducted the investigation: LR and LS. Analyzed the data: LR, LS, and JB. Developed the structure and arguments for the manuscript draft: JB. Edited the manuscript for content and style: LR, LS, and JB. Agreed with the manuscript results and conclusions: LR, LS, and JB. Made critical revisions and approved final version: LR, LS, and JB. All authors reviewed and approved the final manuscript.
Footnotes
Acknowledgments
We thank Terry Meredith for assistance with data presentation and Peter Shabe for conducting statistical analyses.