
Abstract
Objective
To examine the educational effects of a tailored leaflet on current drinking behavior, thoughts about drinking alcohol during pregnancy, and knowledge of fetal alcohol syndrome (FAS) among pregnant women.
Design
Intervention.
Participants
We recruited pregnant women who were participating in maternity classes held at five municipal health centers in Saitama Prefecture and Tokyo in Japan.
Methods
Questionnaires were administered before and after distribution of either a tailored or a non-tailored leaflet and again after the women delivered their babies.
Results
More women read the non-tailored leaflet than the tailored one; this was because they felt they could read the non-tailored leaflet immediately. As for educational effects, the tailored leaflet was not superior to the non-tailored one in changing the women's behavior, thoughts, or knowledge.
Conclusion
It is more important for health education leaflets to seem easy to read in terms of volume than to be tailored.
Introduction
Health education materials that are tailored to a particular audience have been reported to be more effective than non-tailored ones.1–3 Such materials have been developed for smoking cessation, improving dietary behavior, and increasing physical activity.4–7
In a previous study, we developed an educational leaflet about drinking during pregnancy. 8 The leaflet was tailored to pregnant women in its appearance and contents. In the process evaluation, pregnant women who participated in four group interviews were asked if they would take it or not if it was placed on the front desk of a maternity hospital along with a “please take one” sign. 9 More than 81% of the women said they would pick up the tailored leaflet, compared with 56% who said they would take a non-tailored leaflet. However, we did not assess the educational effects of the tailored leaflet in the field.
The present study examined the educational effects of the tailored leaflet on current drinking behavior, thoughts about drinking alcohol during pregnancy, and knowledge of fetal alcohol syndrome (FAS) among pregnant women who participated in maternity classes held at municipal health centers. We also examined the long-term educational effect of a single distribution of the leaflet by asking women to complete a questionnaire after their babies were delivered.
Method
Participants
In Japan, municipal health centers run maternity classes to provide health education to female residents who
are pregnant for the first time. Most maternity classes consist of four sessions, with each session held on the same day of the week over a one-month period. The frequency of the maternity classes depends on the population administered by the center; some small towns, for example, hold only three courses of maternity classes each year, while some health centers in Tokyo's 23 special wards run maternity classes every month.
We recruited pregnant women in maternity classes held by five municipal health centers in Tokyo and Saitama Prefecture, an adjacent prefecture to Tokyo. Some participants took part in all sessions, but some did not.
Description of the Intervention
We measured the educational effects of tailored and non-tailored leaflets at three time points (pre-intervention, post-intervention, and follow-up). Participants were divided into three groups (tailored-leaflet group, non-tailored-leaflet group, and control group) by the month in which they participated in classes at the same municipal health center (Fig. 1). First, we administered a pre-intervention questionnaire to the three groups on the first day of a maternity class. After participants completed the questionnaire, we distributed a tailored leaflet to the participants in the tailored-leaflet group and a non-tailored leaflet to the participants in the non-tailored-leaflet group. Nothing was distributed to the control group. Second, we administered a post-intervention questionnaire to the three groups on the last day of the maternity class. For the tailored-leaflet and non-tailored-leaflet groups, we requested participation in a follow-up survey to be sent by postal mail. Those who agreed to participate were asked to write their mailing address in the post-intervention questionnaire. We sent the follow-up questionnaire to only those who agreed to participate.
Study design.
The National Institute of Public Health Institutional Review Board, with which the second author was affiliated when the study was conducted, approved the study procedures.
Leaflets
The tailored leaflet was tailored using the results of four group interviews with a total of 33 pregnant women who participated in our previous study. 8 This half-folded leaflet is printed in full color, and its folded size is 210 mm long and 148 mm wide (Fig. 2). The title, “What a mom can do for her baby to be born,” is on the front cover with a photograph of a baby. This leaflet explains the harmful effects of drinking alcohol during pregnancy. It describes FAS and shows a bar chart that depicts effects of alcohol on fetal development and a photograph of a child with FAS. On the back cover, the leaflet asks pregnant women not to drink alcohol during their lactation period as well. In addition, it gives advice for family and friends of pregnant women.

A half-fold leaflet.
The non-tailored leaflet was made by a nonprofit organization that consults on alcohol problems. This leaflet is printed in two colors, is reed-shaped, and is 225 mm long and 105 mm wide (Fig. 3). On the front cover, the title “Do you know? Pregnancy and Alcohol” is printed with an illustration of a pregnant woman with a wine glass in her hand. In this leaflet, women are advised not to drink during pregnancy and lactation, but without the use of charts or photos.
A reed-shaped leaflet.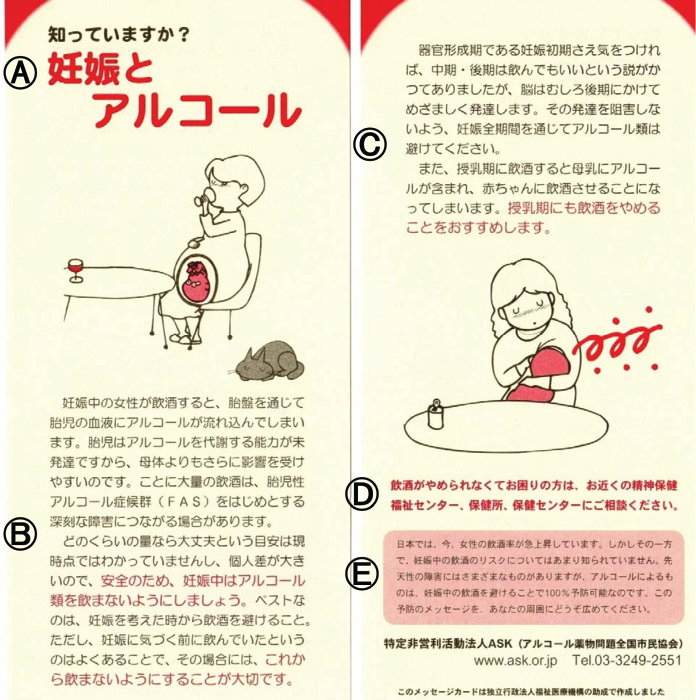
The effect of drinking alcohol during pregnancy and lactation was not mentioned by educators in the maternity classes.
Measures
Demographics
Content of three questionnaires.

Items included in the questionnaire are indicated by +.
Only tailored and non-tailored leaflet groups were asked this question.
Women were asked if they drank alcohol in the period after the maternity class and until delivery.
Whether Participants Read the Leaflet
We asked the participants in the two leaflet groups whether they had read the leaflet. Participants could choose multiple answers from the following choices: “read it completely,” “read half of it,” “read very little of it,” “did not read it at all,” and “did not receive it.” Participants who answered “read it completely” or “read half of it” were asked to indicate their reason from the following choices: “became interested,” “appealing to look at,” “it looked like something I could read quickly,” “useful,” “saw words I was familiar with,” and “other” with space to write an answer. Participants who answered “read very little of it” or “did not read it at all,” were also asked to indicate their reason by choosing multiple answers from the following: “was not interested,” “unappealing to look at,” “too much detail,” “not useful,” “content already known,” and “other” with space to write an answer.
Current Drinking Habits
We asked about current drinking habits in pre- and post-intervention questionnaires. In the follow-up questionnaire, we asked if they drank in the period after the maternity class and until delivery. Response options were “every day,” “more than once a week,” “more than once a month,” “hardly drink,” and “not drink at all.”
Thoughts about Drinking during Pregnancy
Participants were asked what they thought about drinking during pregnancy in all questionnaires. The response options were “no problem,” “no problem if it is a proper quantity,” “should drink moderately,” “abstinence if possible,” and “absolute abstinence.”
Knowledge of FAS
Participants were asked how much they knew about FAS in all three questionnaires. Response options were “heard it for the first time,” “only heard the name,” and “know what FAS is.” In addition, those who answered “only heard the name” or “know what FAS is” were asked for the source of this information at post-intervention. Participants could choose multiple answers from the following responses: “school,” “health center,” “hospital/clinic,” “family member/friend,” “television/book/magazine,” “Internet,” and “other” with space to write an answer.
We also asked about the cause of FAS at post-intervention and follow-up. Response options for this question were “smoking,” “adverse effects of medication,” “chromosomal abnormality,” “alcohol consumption,” “insufficient nutrition,” “environmental change,” “heredity,” and “do not know.” Participants could choose multiple answers.
Although we used per protocol set (PPS) analysis first, we also conducted an intention-to-treat (ITT) analysis including all participants who completed the pre-intervention questionnaire in order to examine the difference by analytical methods. To deal with missing data, previously recorded data were used as substitutions in the last questionnaire. For instance, if a participant answered “absolute abstinence” on the question regarding thoughts about drinking during pregnancy at pre-intervention and the response to the same question at post-intervention was missing, we substituted “absolute abstinence” for the missing data. The criterion for statistical significance was set at p < .05. All analyses were performed using SPSS version 19.0.
Results
Demographic characteristics by groups are presented in Table 2. The mean month of pregnancy was 6.4 ± 1.0 in the tailored-leaflet group, 6.4 ± 1.1 in the non-tailored-leaflet group, and 6.1 ± 1.1 in the control group. In each group, more than 90% of women were in their first pregnancy.
Characteristics of participants.

Pearson's chi-square test.
Table 3 shows the extent to which they read the leaflet. All the women in the two leaflet groups received a leaflet. Those who answered “read it all” or “read half of it” were asked to choose the reasons from multiple answers. The percentages of those who said they read the leaflet because “it looked like something I could read quickly” were 29.4% for the tailored leaflet and 57.5% for the non-tailored leaflet (p < .05). Data for those who said that they “read very little of it” or “did not read it at all” were excluded from further analysis.
The extent to which they read the leaflet.

Pearson's chi-square test.
Regarding drinking habits, 89.2%, 91.9%, and 92.2% of participants chose “not drink at all” at the pre-intervention, post-intervention, and follow-up period, respectively. Pearson's chi-square test showed no significant associations in the proportions of current drinking habits (“every day,” “more than once a week,” “more than once a month,” “hardly drink,” and “not drink at all”) among the three groups at both pre- and post-interventions. The McNemar test showed no significant differences in any group in the percentage of those answered “not drink at all” between pre- and post-interventions. Over 90% of women in the tailored-leaflet and non-tailored-leaflet groups chose “not drink at all” at follow-up. There were no statistically significant associations in the proportions of current drinking habits between groups at both post-intervention and follow-up. There were also no significant differences in the percentages of those who chose “not drink at all” between post-intervention and follow-up in either of the two leaflet groups (McNemar test). ITT analyses showed no statistical significance in either between-group or within-group comparisons (not shown in Table).
Thoughts about drinking during pregnancy between pre- and post-interventions.

Between-group comparison in the percentage of “absolute abstinence” at pre-intervention was examined by 2 × 2 cross-tabulation. P values of this test are (
McNemar's test was used for within-group comparison of the percentage of “absolute abstinence” between pre- and post-interventions.
Pearson's chi-square test examined associations between proportion of each answer and groups at pre- and post-interventions, respectively.
Thoughts about drinking during pregnancy at pre- and post-intervention and follow-up.
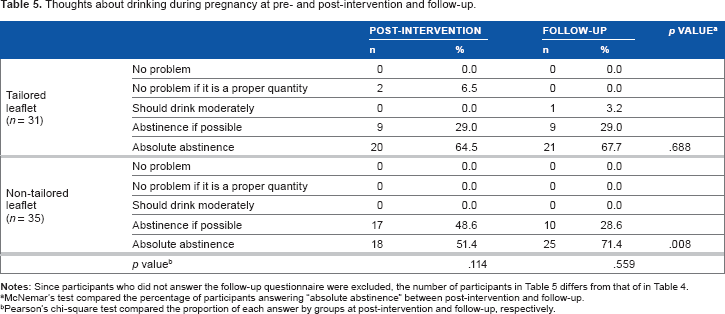
Since participants who did not answer the follow-up questionnaire were excluded, the number of participants in Table 5 differs from that of in Table 4.
McNemar's test compared the percentage of participants answering “absolute abstinence” between post-intervention and follow-up.
Pearson's chi-square test compared the proportion of each answer by groups at post-intervention and follow-up, respectively.
How much do you know about fetal alcohol syndrome (FAS)?

McNemar's test compared the percentage of participants answering “know what FAS is” between pre- and post-interventions.
Pearson's chi-square test compared the proportion in each answer by groups at pre- and post-interventions, respectively.
The cause of fetal alcohol syndrome (FAS).

Multiple choices.
Pearson's chi-square test was used for between-group comparison at post-intervention.
Pearson's chi-square test was used for between-group comparison at follow-up.
Recalculation of the participants who chose “alcohol consumption” only.
In both tailored and non-tailored leaflet groups, there were no statistical within-group differences between post-intervention and follow-up (McNemar's test).
As for the sources of information about FAS, the percentage of those who answered “leaflet” was significantly higher in the two leaflet groups than in the control group (65.1% in the tailored-leaflet group, 52.8% in the non-tailored-leaflet group, and 13.3% in the control group).
Discussion
PPS analysis could cause selection bias, but our ITT analysis yielded results similar to the PPS analysis. Thus, the selection of women for the analyses did not seem to bias the results. Since our data relied on self-reports, its accuracy might suffer from social desirability effects. In order to connect the answers of the same person at different time points, our questionnaires had to require participants to provide their names.
The tailored leaflet used in this study was developed through focus group discussions in a previous study. 8 In a previous evaluation, we found that pregnant women preferred the tailored leaflet in draft version over the non-tailored one because the former had a more attractive front cover, detailed content, and presented a real-life example, unlike the latter. 9 In a practical setting, however, they tended to read the leaflet that was easier to read. The percentage of women who read the entire leaflet was higher in the non-tailored-leaflet group than in the tailored-leaflet group (Table 3).
No participants who received the non-tailored leaflet answered that they “did not read it at all” (Table 3). This was surprising because other studies reported that as many as 6-14% of people who received health education materials did not read them at all.10,11 In a study by Maeda et al, 25% of mothers with a child 0-4 years old did not even remember if they had read a leaflet about sudden illnesses among children. 12 A similar result was observed in our tailored-leaflet group, with 9.1% answering that they did not read the leaflet at all.
Our finding that 57.5% of those who read the non-tailored leaflet gave the reason that “it looked like something I could read quickly” supported the idea that health education materials should be easily read by targeted people. 13 People with hectic schedules cannot spare much time for healthcare, so it seems to be important to provide health information materials that can be read easily. No matter how good the content is, it is meaningless if people do not read it. Since people cannot be forced to read health education materials, except perhaps in a textbook in a classroom setting, it is important to encourage the willingness of targeted people to read them.
This study aimed to assess the educational effects of a tailored leaflet on drinking behavior, thoughts, and knowledge among pregnant women. We could not detect a significant change in drinking behavior since 89.2% of the women did not drink before the intervention. The percentage of the pregnant women in this study who consumed alcohol was a little higher than the 4.6% in another study of Japanese pregnant women. 14
The Second Health Japan 21, the second health policy for Japan in the 21st century, set a goal to reduce the percentage of pregnant women who drink alcohol from 8.6% to 0% by 2014. 15 At pre-intervention, 86.8% of women had heard information about drinking during pregnancy (Table 2), but just a few of them knew what FAS is (Table 6). In Japan, women of reproductive age have few opportunities to receive formal alcohol education despite the volume of maternity books and magazines. Even in maternity classes held by municipal health centers, only 24% of healthcare providers mentioned alcohol drinking during pregnancy. 16 The respondents in that study pointed out inconsistencies in the literature concerning harmful alcohol-consumption levels during pregnancy, leading to a lack of confidence in teaching this topic. Development of evidence-based alcohol education materials would help healthcare providers to give accurate information to pregnant women.
The significant within-group differences in thoughts about drinking during pregnancy that are shown in Tables 4 and 5 seem to be due to the lower percentage of “absolute abstinence” that was reported at the earlier time points. A between-group comparison by 2 x 2 cross-tabulation, however, showed a significant difference in the percentage responding “absolute abstinence” only between the tailored-leaflet group and the control group at pre-intervention (p = .015, data not shown). Regardless of the percentages reporting “absolute abstinence” at the earlier time points, a single distribution of either leaflet increased the percentages to about 60% at post-intervention (Table 4) and 70% at follow-up (Table 5). Thus, we assumed that distribution of either leaflet could improve understanding of the harmful effects of drinking during pregnancy for a certain percentage of women.
We did not find a difference in thoughts about drinking between the tailored-leaflet and non-tailored-leaflet groups. Previous studies showed that non-tailored material that is a good fit for targeted people was as effective as tailored material in terms of changing attitudes and intentions.1,17 In those studies, the tailored material was developed from a tailoring assessment questionnaire that was administered to the participants. The findings showed that non-tailored materials of moderate-fit and poor-fit for targeted people were less effective than tailored and good-fitting materials. We can conclude that regardless of whether materials are tailored, those that are a good match to the interests of targeted people might be effective.
A comparison between pre- and post-intervention results in Table 6 shows significant educational effects of the two leaflets for acquiring knowledge of FAS. The level of knowledge at post-intervention significantly differed by groups. More participants in the tailored-leaflet group answered, “know what FAS is” than did those in the non-tailored-leaflet group. Since the results in Table 6 reflect self-evaluation of their knowledge, we further evaluated whether participants learned correctly, and these results are shown in Table 7. Although nearly 100% of the women chose “alcohol consumption” as a cause of FAS, the percentage of women who chose only the correct answer was below 80% at both post-intervention and follow-up. The percentage of choosing only the correct answer did not significantly differ by the groups at either time point. On the basis of this result, we could not conclude that the tailored leaflet was more effective in advancing knowledge than the non-tailored one. Few studies have assessed the effectiveness of tailored materials from the viewpoint of advancing knowledge. In a study addressing dietary behavior, there was no significant difference in nutrition knowledge between tailored and non-tailored groups. 3
Our follow-up survey after delivery showed that women retained their knowledge for a long time after reading the leaflets (Table 7). Scala et al also reported a marked improvement in participants’ knowledge and its persistence over time after reading a leaflet directed at adults with chronic obstructive pulmonary disease (COPD). 18
In conclusion, our tailored leaflet was not superior to a non-tailored one in changing the behavior, thoughts, and knowledge of our participants. We found that it was more important that health education leaflets seem easy to read than that they are tailored to a target group.
Author Contributions
Conceived and designed the experiments: NS. Analyzed the data: NT. Wrote the first draft of the manuscript: NT. Contributed to the writing of the manuscript: NT and NS. Agree with manuscript results and conclusions: NT and NS. Jointly developed the structure and arguments for the paper: NT and NS. Made critical revisions and approved final version: NS. All authors reviewed and approved of the final manuscript.
Dsiclosures and Ethics
As a requirement of publication the authors have provided signed confirmation of their compliance with ethical and legal obligations including but not limited to compliance with ICMJE authorship and competing interests guidelines, that the article is neither under consideration for publication nor published elsewhere, of their compliance with legal and ethical guidelines concerning human and animal research participants (if applicable), and that permission has been obtained for reproduction of any copyrighted material. This article was subject to blind, independent, expert peer review. The reviewers reported no competing interests.
Footnotes
Acknowledgements
We thank the women and municipal health centers who participated in this study.