
Abstract
Previous studies have suggested that altruistic behaviors for children and grandchildren (ABC) have a complex mechanism for psychiatric morbidity among parents and grandparents. The interaction between ABC and sense of obligation to children/grandchildren (SOC) may help to provide a better understanding of the association between ABC and psychiatric morbidity. In this study, we seek to investigate the association between the interaction of ABC and SOC and generalized anxiety disorder (GAD) and major depression (MD) using a nationally representative sample of middle-aged parents/grandparents in the United States (N = 2,193). Among women, feeling obligated was associated with MD regardless of ABC status. Among men, having SOC and providing informal assistance or financial support was associated with GAD morbidity. Further research that elucidates the complexity of the interaction of ABC and SOC on psychiatric morbidity among parents/grandparents is needed.
Introduction
The impact of parenthood on the mental health of parents is inconclusive. While some studies report a negative relationship between parenthood and psychological well-being (Glenn and McLanahan, 1981; Hughes, 1989), others have reported a positive relationship (Aneshensel, Ferichs, and Clark, 1981; Burton, 1998; Kandal, Davies, and Raveis, 1985), and others have indicated no relationship (Evenson and Simon, 2005; Ross, Mirowsky, and Goldsteen, 1990; Umberson and Gove, 1989).
Altruistic behavior is defined as “behavior intended to benefit another, even when this risks possible sacrifice to the welfare of the actor” (Monroe, 1996). Thus, taking care of children, including healthy and adult children, is considered a type of altruistic behavior. Lee, Colditz, Berkman, and Kawachi (2003) showed that those who took care of healthy children were more likely to die of coronary heart disease in the Nurse Health Study, suggesting that taking care of healthy children can also be stressful. However, this study did not examine the impact of altruistic behaviors on father's mental health. A recent study conducted in Denmark, showed that new fathers did not show depressive symptoms after the delivery of a new baby, while mothers showed higher postpartum depressive symptoms (Munk-Olsen, Laursen, Pedersen, Mors, and Mortensen, 2006), suggesting that fatherhood is not as stressful as motherhood.
A recent study showed that the impacts of altruistic behavior to children and grandchildren (ABC) on the mental health of parents/grandparents varied by the type of ABC (Fujiwara and Lee, 2008). For example, among mothers/grandmothers, financial support to children had a harmful effect on major depression (MD), while among fathers/grandfathers, financial support had a protective effect on the development of MD. This difference might be due to differences of sense of obligation to children and grandchildren (SOC): mothers/grandmothers tend to have high SOC, while fathers/grandfathers have lower SOC (Rossi, 2001).
Considering this background, we hypothesized that the interaction between SOC and ABC might have different associations with psychiatric morbidity among parents/grandparents. The interaction can be investigated by different combinations of levels of SOC and ABC. First, those who have provided ABC with low SOC are considered to be feeling stressed, as they might provide ABC extrinsic motivation (stress group). Second, those who have high SOC but are not providing ABC are considered to be feeling guilty, as they think he or she is supposed to provide ABC but is not doing it (guilt group). Third, those who have a high SOC and provide ABC might feel obsession, as they provide ABC based on their SOC, regardless of whether or not the children or grandchildren are asking them for something, they may not consider their ABC as enough (obsession model).
Thus, the purpose of this study is to compare the psychiatric morbidity of parents/grandparents 1) who provide ABC with a low SOC (stress group); 2) who provide ABC with a high SOC (obsession group), and 3) who do not provide ABC but have a high SOC (guilt group) with reference of non-ABC and low SOC parents/grandparents.
Method
Study Design and Participants
Cross-sectional survey was used to investigate the hypothesis. The National Survey of Midlife Development in the United States (MIDUS) is a collaborative, interdisciplinary investigation of the patterns, predictors, and consequences of midlife development in the areas of physical health, psychological well-being, and social responsibility conducted during 1995–1996 (Brim et al. 2003). Respondents were selected from a nationally representative random digit dial sample of non-institutionalized, English-speaking adults, between 25 and 74 years of age, with oversampling of older respondents, selected from working telephone banks in the coterminous United States. MIDUS respondents first participated in a telephone survey, lasting approximately 40 minutes. The response rate for the telephone survey was 70%. Then, respondents were asked to complete the self-administered mail questionnaire. The response rate for the self-administered questionnaire was 86.8%. This yields an overall response rate of 60.8% for both telephone interview and self-administered mail questionnaire (N = 4,242). As we are interested in caregiving to children, childless participants were excluded from our study. Sampling weights correcting for selection probabilities and non-response allow this sample to match the composition of the U.S. population on age, sex, race, education, and marital status. Finally, the weighted number of the sample became 2,193 (1,162 for females and 1,031 for male). Detailed information regarding the MIDUS study is available in a previous publication (Brim, 2000).
Measures
Psychiatric Morbidity
MIDUS researchers assessed generalized anxiety disorder (GAD) and major depression (MD) using telephone responses to the screening versions of the WHO's “Composite International Diagnostic Interview Short Form” (CIDI-SF), Version 1.0 (Kessler, Andrews, Mroczek, Ustun, and Wittchen, 1998; World Health Organization, 1990). GAD and MD determinations were based on definitions and criteria specified in the DSM-III-R (American Psychiatric Association, 1987). The test-retest reliability and clinical validity of CIDI diagnoses have previously been examined (Blazer, Kessler, McGonagle, and Swartz, 1994). Moreover, GAD and MD scales employed in the present study were used in previous publications, where it was based upon the responses of the MIDUS dataset (Fujiwara, 2007; Kessler, Mickelson, and Williams, 1999).
Altruistic Behaviors for Children and Grandchildren (ABC)
ABC were measured by mail-in questionnaire in three dimensions: informal assistance, emotional support, and financial support. Informal assistance was assessed by asking the following question: “On average, about how many hours per month do you spend providing unpaid assistance, such as help around the house, transportation, or childcare, to your grandchildren or grown children?” Emotional support was assessed by the following question: “On average, about how many hours per month do you spend giving informal emotional support, such as comforting, listening to problems, or giving advice to your children or grandchildren?” For the question of informal assistance and emotional support, respondents answered by indicating the number of hours. Financial support was measured by the following question: “On average, about how many dollars per month do you or your family living with you contribute to your grandchildren or grown children? If you contribute food, clothing or other goods, include their dollar value.” Respondents answered by the amount of dollars. ABC measurements were further divided into 3 categories: (1) non-ABC (2) low ABC and (3) high ABC. Cut-off for low and high ABC was decided based on their distributions. Therefore, informal assistance was categorized as 0, 1–10, and 11 and more hours/months; emotional support was categorized as 0, 1–12, and 13 and more hours/month; financial support was categorized as 0, 1–100, and 101 and more dollars/month.
Sense of Obligation to Children and Grandchildren (SOC)
Norms such as sense of obligation can be measured on a very general level, independent of whether or not an individual has actually confronted the situation posed in an item (Rossi, 2004). SOC was assessed by mail-in questionnaire using the following three questions: “How much obligation do you feel if the following hypothetical situations happened to you: (1) to drop your plans when your children seem very troubled; (2) to call, write, or visit your adult children on a regular basis; and (3) to take your divorced or unemployed adult child back into your home”. Respondents answered by 0–10 Likert scale (0 denoted lowest degree of care and 10 denoted highest degree of obligation). These questions were selected from six pilot surveys of approximately one thousand responses in advance of MIDUS survey (Rossi, 2004) and used as part of a scale of family obligation in previous studies (Grzywacz and Marks, 1999). SOC was calculated using the weighted mean of scored responses. Cronbach's alpha for this scale was 0.74, which is considered to be relatively high. SOC was further categorized into two categories, high and low, based on its average score in this sample.
Parents/Grandparents Covariates
Parents/grandparents covariates such as age, race, education, working status, marital status, and perceived physical health are considered to be associated with psychiatric morbidity, sense of obligation, and ABC. Our rationale for selecting these variables include previous findings by Rossi (2001) in which parents/grandparents' age and education had direct net effects on altruistic behavior for ones family (informal assistance, emotional support and financial support). Being married predicts more emotional support to family members and better perceived physical health was associated with more altruistic behavior. Since race was also associated with ABC (e.g. Goodman et al. 2006), we have included race as a confounding variable. Previous studies have shown that the physical health of the caregiver is associated with caregiving behavior (e.g. Lee et al. 2003). Details of categorization of covariates are shown in Table 1.
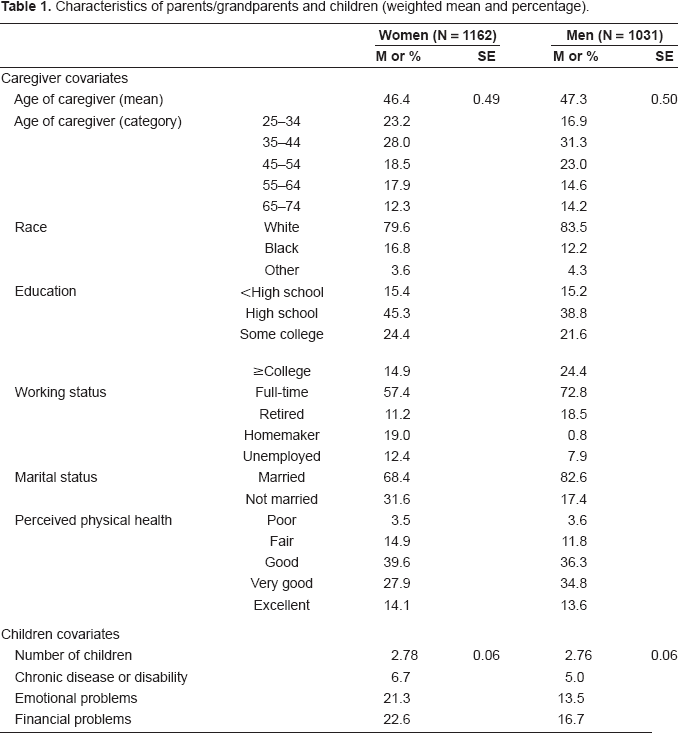
Characteristics of parents/grandparents and children (weighted mean and percentage).
Children's Covariates
The greater number of children in which the parents/grandparents must provide for was significantly related to higher ABC (Rossi, 2001). Child characteristics have been shown to modify the health outcomes of caregivers, specifically the psychological health of the caregiver. King, King, Rosenbaum, and Goffin (1999) found child behavior problems to be the most important predictor of caregiver psychological well-being. In addition, the severity of the disability has been shown to be related to parental stress (Raina et al. 2005). Children's temperament has also been related to feelings of depression in the parents (Beckman, 1983); therefore, we have included emotional problems of the child as a confounding variable in the analyses. As we are also looking for financial contributions to children, we have included financial problems of children as a confounder. Age of children was not included in the model, as age of children was highly correlated with the age of parents/grandparents (correlation coefficient: 0.92, p < 0.001).
The number of children for each respondent was assessed by telephone interview by asking the number of biological children and step, adopted, and other types of children raised by respondents. The total number of children was calculated by summation of the two measures. In addition, status of children was assessed by the following questions: “Please indicate whether the following problems have happened to any of your children in the past 12 months: a) chronic disease or disability, b) emotional problems (e.g. sadness, anxiety), and c) financial problems (e.g. low income, heavy debts).” Respondents answered by dichotomous choice.
Analysis
To investigate the hypothesis, ABC and SOC were combined as follows: 1) low SOC and no ABC (reference group), 2) low SOC and low ABC, 3) low SOC and high ABC, 4) high SOC and no ABC, 5) high SOC and low ABC, and 6) high SOC and high ABC. The different impact of these groups on the psychiatric morbidity of respondents was analyzed using multiple logistic regression with reference group, stratified by sex. We examined the association by the following 3 models: 1) unadjusted model (Model 1), 2) adjusted for parents/grandparents' covariates (Model 2), and 3) adjusted for parents/grandparents' and children's covariates. Sampling weights were applied to adjust for possible selection bias and differential non-response (see detailed weights method for MIDUS in other literature (2). The STATA SE statistical package, version 9, was used to manage the data and to perform the analysis. It is assumed that the association has an independent and significant effect if p < 0.05 and is weak if p < 0.1.
Results
Table 1 describes characteristics of parents/grandparents and their children. Weighted mean age was 46.8 years. Around 73% of men were full-time workers, while 57% of women were full-time workers and 19% of women were homemakers. Married respondents were distributed as 68% for women, and 83% for men. The average number of children was 2.8 for both groups. The number of children varied from 1 to 10 children for each caregiver. The ages of children ranged from 0 to 58, with mean age of 24 years old, in accordance with caregivers age range, from 25 to 74. Thus, in this sample, “children” includes very young children, such as infant, to adult children, who may also have children.
Distributions of ABC and SOC were shown in Table 2. Women showed longer durations of informal caregiving and emotional support and higher SOC than men (p < 0.001). On the contrary, men showed larger amounts of financial support than women (p = 0.022). The percentage of high SOC was higher among women than men (p < 0.001).
Distribution of ABC and SOC (weighted percentage).
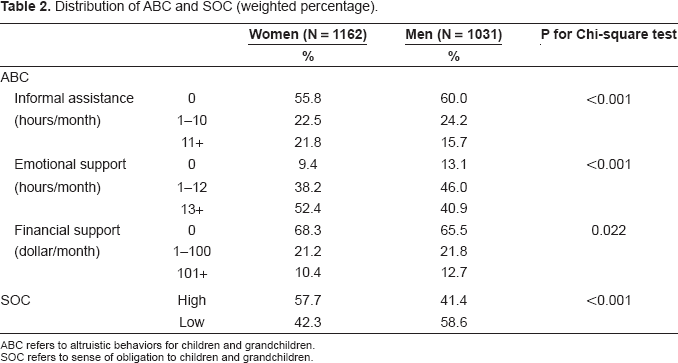
ABC refers to altruistic behaviors for children and grandchildren.
SOC refers to sense of obligation to children and grandchildren.
Table 3 shows the results for weighted odds ratio of psychiatric morbidity of parents/grandparents by combining ABC and SOC among women. High SOC with no informal assistance group (guilt group) was associated with MD morbidity in Model 2. High SOC combined with low informal assistance groups (obsession group) was also associated with MD morbidity in Model 2; however, low SOC with low and high informal assistance groups (stress group) was not associated with MD. The associations were no longer significant after adjusting for children's covariates. Either model of informal assistance was not associated with GAD among women. High SOC and low emotional support group (obsession group) showed a harmful effect for MD morbidity in Model 2. The harmful effect of emotional support was no longer significant after adjusting for children's covariates. High SOC combined with low financial support group (obsession group) had a harmful effect on MD after adjusting for children's covariates (Model 3). Low SOC combined with low and high financial support groups (stress group) was not significantly associated with GAD or MD. Although not shown in Table 3, older age and better physical health groups were significantly protected for MD. Race, education, working status, and marital status were neither significantly associated with GAD nor MD. Those who have ill or disabled children and children with emotional problems showed a significantly higher prevalence of MD, but not GAD. The number of children and financial problems of children are not significantly associated with GAD or MD.
Weighted odds ratios of psychiatric morbidity by the combination of ABC (informal assistance, emotional support, financial support) and SOC, women (mothers/grandmothers).
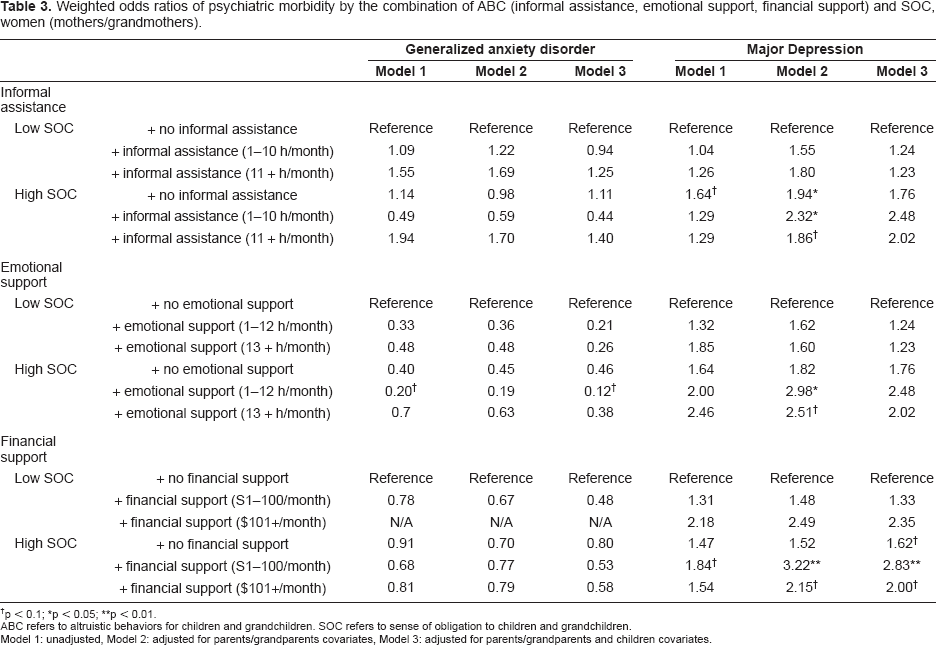
p < 0.1;
p< 0.05;
p < 0.01.
ABC refers to altruistic behaviors for children and grandchildren. SOC refers to sense of obligation to children and grandchildren.
Model 1: unadjusted, Model 2: adjusted for parents/grandparents covariates, Model 3: adjusted for parents/grandparents and children covariates.
Results for weighted odds ratio of psychiatric morbidity of parents/grandparents by combination of ABC and SOC among men are shown in Table 4. High SOC with low and high informal assistance groups (obsession group) were highly associated with GAD morbidity after adjusting for parents/grandparents and children's covariates (Model 3). The same association was not observed for MD. High SOC without informal assistance group (guilt group) was neither associated with GAD nor MD. With regard to emotional support, either model was associated with neither GAD nor MD among men. High SOC with high financial support groups (obsession group) showed higher GAD morbidity. Specifically, those with a high SOC who support their children with more than 100 dollars per month were about 15 times more likely to have GAD after adjusting for covariates. Although the data is not shown in Table 4, younger age, unemployed, and worse physical health groups showed higher psychiatric morbidity. Race, education, and marital status were neither significantly associated with GAD nor with MD. The number of children was significantly associated with GAD in the analysis of emotional and financial support. Other covariates on children were not associated with GAD or MD.
Weighted odds ratios of psychiatric morbidity by the combination of ABC (informal assistance, emotional support, financial support) and SOC, men (fathers/grandfathers).
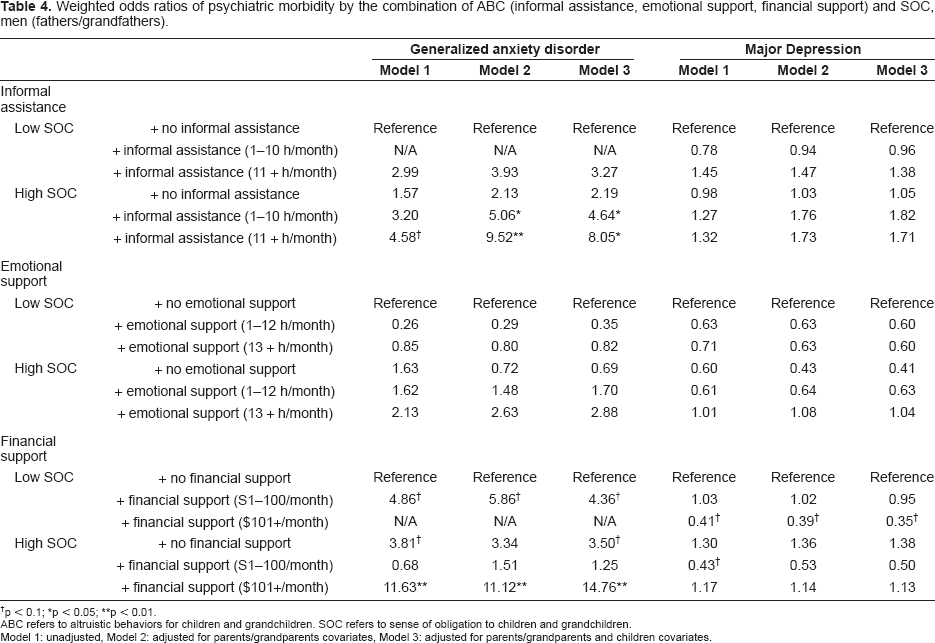
p < 0.1;
p< 0.05;
p < 0.01.
ABC refers to altruistic behaviors for children and grandchildren. SOC refers to sense of obligation to children and grandchildren.
Model 1: unadjusted, Model 2: adjusted for parents/grandparents covariates, Model 3: adjusted for parents/grandparents and children covariates.
Discussion
Our research contributes to the family psychology literature by demonstrating that the interaction between ABC and SOC had different impacts on specific psychiatric morbidity. To highlight, among women, having high SOC but not providing them with informal assistance was associated with MD morbidity (guilt group); any type of ABC with high SOC was harmful for MD (obsession group). Among men, having high SOC and providing informal assistance or financial support was associated with GAD morbidity (obsession group). Low SOC and providing ABC (stress group) were not significantly associated with psychiatric morbidity in both women and men.
To the best of our knowledge, this study is the first to show the association between the interaction of ABC and SOC and psychiatric morbidity of parents/grandparents. A previous study showed that emotional and financial support was harmful on MD development among women (Fujiwara and Lee, 2008). This study adds to the literature that those who feel high SOC and provide any type of ABC are at risk of MD among women. Those with low SOC are not at risk of MD regardless of ABC. This suggests that women feel obligated to provide ABC, which might be associated with low self esteem. For example, “I am not a good mother if I do not provide enough emotional or financial support to children/grandchildren”. An interesting finding from our research is that those with high SOC and who did not provide informal assistance was harmful for MD (guilt group). Providing informal assistance would be a central role for mother/grandmother. As having a chronic disease or emotional problems mediated the effect of not providing informal assistance with high SOC on MD, parents/grandparents might feel guilty when children have extra needs, and they do not feel guilty when children are healthy.
For men, a previous study showed that providing emotional support is harmful for MD, but providing informal assistance and financial support were protective for MD (Fujiwara and Lee, 2008). In this study, either type of ABC was significantly associated with MD. However, providing informal assistance and financial support with high SOC were associated with high prevalence of GAD. Considering the high comorbidity of MD and GAD, the findings in the current study is inconsistent with the previous study. The reverse causation (i.e. men feel high SOC and provide informal assistance and financial support due to having GAD) would help to interpret the association. The association between SOC and GAD might be strong enough to diminish the protective effect of ABC on psychiatric morbidity.
Contrary to our hypothesis, except for financial support by men, the stress group (i.e. ABC with low SOC) was not associated with psychiatric morbidity. Rather, men with low SOC and providing financial support were protective for the development of MD. We hypothesizd that those who provide ABC with low SOC might feel stress, but actually, they might feel more positive. Several previous studies have reported the positive effect of ABC, or caregiving on caregiver (e.g. Schwartz and Gidron. 2002). Those who are heavily involved with caring for their children tend to derive more purpose from life and more meaning from the parental role (Burton and DeVries, 1992; Gattai and Musatti, 1999; Hayslip, Shore, Henderson, and Lambert, 1998). Parents with children who are mentally-ill feel rewarded through their sense of satisfaction from fulfilling their parental duty and realization of a deeper sense of self and a deeper understanding of life (Schwartz and Gidron, 2002). The satisfaction generated from caregiving comes from the interpersonal dynamic between the caregiver and the person cared-for, the intrapersonal orientation of the caregiver, and a desire to promote a positive outcome for the person cared-for (Grant and Nolan, 1993). These positive effects might arise as side effect of providing ABC, for those who have low SOC.
Although GAD and MD are highly comorbid, our study showed that the ABC and SOC had different associations with GAD and MD. Specifically, SOC was more likely to be associated with MD among women, and more likely to be associated with GAD among men. It has been reported that pure GAD and MD have different specific antecedent risk factors (Moffitt et al. 2007). Pure MD is predicted more strongly by low positive emotion, but not GAD, suggesting that individuals with a higher threshold for experiencing positive emotion are at specific risk for MD (Watson, 2005). In our study, more women who have SOC are considered to have a higher threshold for expressing positive emotion (i.e. unsatisfied with their caregiving behaviors) than men. Therefore, they showed higher morbidity of MD, but not GAD. It has also been reported that pure GAD had risks during childhood, such as adverse family environment (e.g. low SES, child maltreatment), which is not associated with pure MD. Thus, it is suggested that more men who have SOC experienced adversity during childhood than women; therefore, they show high GAD morbidity but not MD. Further research to investigate the sex difference of the effect of childhood adverse experiences on SOC and eventually the onset of psychiatric morbidity, for both GAD and MD is needed.
The limitations of this study provide abundant material for future research. First, as the MIDUS study is a cross-sectional study, the causality of the associations between the interaction of ABC and SOC with GAD and MD cannot be established. Reverse causation may explain the association; e.g. mothers with MD tend to feel higher SOC towards their children, but also do not provide ABC. In addition, temporality of the association could not be established as some results were not consistent with each other. Second, there may be other confounders to explain the associations. For example, an inborn nervous temperament may be associated with increased SOC and having GAD. Further research is needed to measure possible inborn temperament confounders. Third, ABC was assessed by the combination of altruistic behaviors to children and grandchildren. The impact of altruistic behaviors to children on the mental health of parents might be different from the impact of altruistic behaviors for grandchildren on grandparents' mental health. As we observed significant age effects for psychiatric morbidity (i.e. the older participants were protected from psychiatric morbidity), altruistic behavior only for children may have a stronger impact on the psychiatric morbidity of parents as participants became younger. Further research needs to consider this age effect to investigate the association between ABC, SOC and mental health. Fourth, a relatively small sample size of ethnic minorities precluded the analysis of stratification by race. We did not observe a significant effect of race, which is consistent with a previous study (Goodman et al. 2006). Further research oversampling ethnic minority groups may find different associations between the difference of ABC and SOC with mental health by race.
Despite these limitations, this study has several strengths. First, as the MIDUS study is a nationally representative sample, the findings can be generalized within U.S. society. Second, the large study sample provided strong statistical power to adjust for possible parents/grandparents and children confounders. Third, the MIDUS study used an established diagnostic scale of GAD and MD based on the DSM-III-R. Previous studies frequently used The Center for Epidemiologic Studies Depression Scale to measure psychological health, but this scale failed to distinguish anxiety and depression. Fourth, the MIDUS study covered adults at mid-life, between 25 and 74 years of age, those who often take care of children, but often receive less attention as an at-risk group for mental disorders.
Based on these findings, it is recommended for physicians and mental health workers to recognize women who report a higher SOC but are not providing informal assistance or financial support, which is a risk factor for MD, and for men who show higher SOC and providing informal assistance or financial support to have GAD. Health care providers should ask their patient about ABC and SOC if they have children or grandchildren. It is particularly recommended for physicians and mental health workers to pay attention to mothers who have ill children but who are not providing care, as they are at risk of having MD.
In conclusion, there are different impacts on the psychiatric morbidity of parents/grandparents depending on the interaction of ABC and SOC, sex of parent/grandparent, and components of ABC. Women who felt a high SOC but did not provide informal assistance (guilt group) or women who provide any type of ABC with high SOC (obsession group), were more likely to develop MD. Men who provide informal assistance or financial support and having high SOC showed higher prevalence of GAD (obsession group). Further research that elucidates the complexity of the interaction of ABC and SOC and its effect on psychiatric morbidity of parents/grandparents is needed.
Disclosure
The authors report no conflicts of interest.