
Abstract
Objective
To assess the metabolic implications for patients admitted to a psychiatric hospital in several patient populations.
Method
Data was collected from the medical records of 108 randomly chosen patients initially diagnosed with schizophrenia and depression in our hospital from 2002 to 2003.
Results
Weight gain over a one-year period was demonstrated in each group of patients (treated with antipsychotics or antidepressants) (p < 0.001). After the implementation of routine lipid panel test, several patients were initially diagnosed with dyslipidemia.
Discussion
It is important to order routine laboratory work rationally, as this adds to the cost of hospitalization, while considering standard of care recommendations.
Introduction
Not too long ago, primary care physicians and psychiatrists were enjoying a period of quiescence with the introduction of effective and relatively safe new generation psychopharmacological agents. Selective serotonin reuptake inhibitors (SSRI) and atypical antipsychotic (AAP) brushed away “inconvenient” older generation of antidepressants and antipsychotics that were associated with significant side effect profiles. However, widespread use of the new agents led to increasing recognition of their potential harm(Houy-Durand and Thibaut, 2002). AAP have been implicated in a variety of conditions conceptualized as “metabolic syndrome” or metabolic abnormalities (Antai-Otong, 2004; O'Neill, 2005). Metabolic syndrome(McKee, Bodfish, Mahorney, Heeth, and Ball, 2005) is loosely defined as a combination of pathological conditions such as: hypertension, lipid abnormalities(Wetterling, 2003), abdominal fat, and insulin resistance(Newcomer, 2004). Considering associated high morbidity and mortality of these conditions, it has become imperative to monitor the metabolic status of patients treated with atypical antipsychotics (Almeras et al. 2004; Meyer and Koro, 2004). All atypical antipsychotics have received a black box warning urging physicians to monitor glucose status of patients receiving treatment (“Physicians' Desk Reference,” 2005), even though it has been difficult to demonstrate a causal link between antipsychotics and glucose abnormalities(Saito and Kafantaris, 2002) due to the increased background risk of diabetes mellitus in patients with schizophrenia and the increasing incidence of diabetes mellitus in the general population.
Current recommendations for patients on antipsychotics include periodic weight, blood pressure, lipid profile, and fasting glucose measurements (McIntyre, McCann, and Kennedy, 2001). Patients with a history of glucose intolerance or diabetes, as well as family history of diabetes, are considered high risk and require more stringent monitoring (Lublin, Eberhard, and Levander, 2005).
SSRI and mixed norepinephrine or serotonin uptake inhibitors do have several side effects including weight gain(Ruetsch, Viala, Bardou, Martin, and Vacheron, 2005). The side effects varies between medication of the same class(Papakostas, 2008). Furthermore, patients with depression will be on medication often for many years, due to the nature of the illness, and we should be aware of the cumulative effect of weight gain over the years(Cassano and Fava, 2004).
Furthermore, a variety of medical conditions may present with psychiatric symptoms, for example: endocrine and neurological conditions (Ambrosino, 1972), infections (Schwab, 1982) and metabolic abnormalities (Golomb, 2002).
In summary, laboratory investigation is helpful in three major areas: to rule out a medical condition affecting, or responsible for the psychiatric disturbance and its effect on the psychiatric treatment modality(Escobar, Hoyos-Nervi, and Gara, 2002; Talbot-Stern, Green, and Royle, 2000) (e.g. hypoxia in an elderly woman with an anxiety disorder), to monitor drug levels of certain psychiatric medication(Preskorn, Burke, and Fast, 1993) (therapeutic level or compliance with the medication), and to evaluate the general health status of a patient that may be affected by psychopharmacological agents(Buse, 2002).
This study looks at the prevalence of weight gain and laboratory abnormalities in a selected group of hospitalized patients with schizophrenia and depression.
Methods
Recruitment
For this study, the subjects were randomly selected out of all the patients admitted over a period of one year (2002 to 2003) with diagnosis of schizophrenia and depression at a publicly-funded state hospital. Their progress was then tracked until August 2005.
The study cohort was composed of 45 patients that meet the Fourth Diagnostic and Statistical Manual of Mental Disorders, Text Revision(“Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, Text Revision,” 2000) (DSM-IV-TR) of established schizophrenia diagnosis, 18 patients newly diagnosed with schizophrenia and 45 patients diagnosed with depression.
Data Collection
Data collected reflected psychiatric assessment in terms of diagnosis, treatment history, symptoms and clinical course, and other assessments reflecting psychological status, demographics, and change in social support systems. Compliance to treatment was assessed by patient report (the insight that one has an illness for which medication is needed) and by staff report of patient compliance with the prescribed interventions while hospitalized.
Documentation regarding laboratory work was obtained from charted laboratory reports. Routine laboratory work done for every patient hospitalized until 2004 includes: cell blood count (CBC), basic metabolic panel (BMP), RPR, thyroid panel, HCG, urine analysis (UA), urine drug screen (UDS). In 2004, in conformity to the standard of care, lipid panel was added to the routine laboratory work (RLW). Concurrently, thyroid panel was discontinued due to limited funds allotted for RLW (the cost for lipid panel is just a fraction of the cost of thyroid panel). Documentation of first and last hospitalization was reviewed for each patient in this study.
Analysis
The resultant data was analyzed using Statistical Package for Social Sciences(“Statistical Package for Social Sciences (SPSS) StatSoft [computer program]. Version 9.0.,” 2000) (SPSS, version 12) software for standard deviation and T-test (2-tailed, p < 0.01) analysis. The University of Missouri Kansas City Health Science Institutional Review Board (IRB) as well as the Missouri Department of Mental Health IRB have approved the study yearly since 2002 and the review is HIPPA compliant(Tribble, 2001).
Results
Demographics
Group 1: patients with established schizophrenia. Forty-five of the patients in the study had the diagnosis of schizophrenia for an average of eight years. Average age for this group was 34.7 years. Sixty-six percent were male and 34% females. Ethnically, 43.9% of these patients were African American and 51.2% of Caucasian origin (Table 1). Despite the fact that employment rate did not change between the first and last hospitalization (8.1% vs 7.6%) the percent of patients receiving a form of income increased from 33 to 71% (p = 0.01), mainly due to successful application for social security disability insurance (SSDI) for return patients.
Demographics.
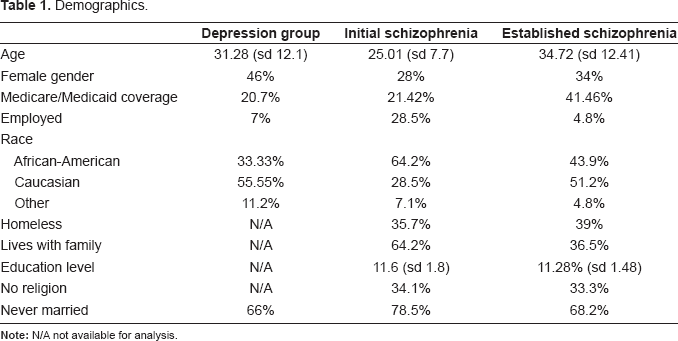
Group 2: patients with depression. For the 45 patients diagnosed with depression, the average age was 31.2 years, 33.33% were African-American, 55.55% Caucasian, and 48% females. Of these patients, only 64.4% had medical insurance at their first visit to our facility (Table 1).
Group 3: patients initially diagnosed with schizophrenia. Average age at the initial diagnosis of schizophrenia was 25 years. Ethnically, 58% of these patients were African American and 24% Caucasian. These patients had achieved an average of 11.1 years of education and 27% (five patients) were employed at the time of initial schizophrenia diagnosis. Ninety-two percent were never married, 58% (14 patients) lived with their families and 33% (eight patients) were homeless. Only 27% (five patients) had medical insurance, three of which received Medicaid.
Of these patients, 18, 25 and 14 were evaluated at least once more in our hospital at 12.8, 9.7 and 9.3 months from their first encounter, for patients with established schizophrenia, depression and initial schizophrenia respectively.
Presentation Pattern
Patients in these three groups presented to emergency department (ED) referred mainly by law enforcement officers, family, and also self referral. Patients diagnosed with depression, were more likely to be referred by police on their first visit (p < 0.001) mainly out of concern for danger to self. For schizophrenic patients, police escort during the last visit was more common (p = 0.04) than in their first, and remained approximately at one third of all patients in the established schizophrenia group (Table 2).
Presentation pattern.
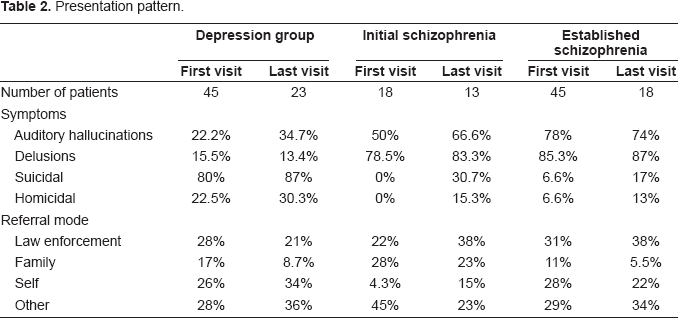
Family referral of patients was more common for the initial visit of patients newly diagnosed with schizophrenia than the other two groups (p = 0.004). At the second presentation, this group was less likely to be referred by family (p = 0.02), and was also similar in the depressed group compared with first presentation (p = 0.16) (Fig. 1). The rate of family referral did not differ between subsequent presentations for the established schizophrenia group.
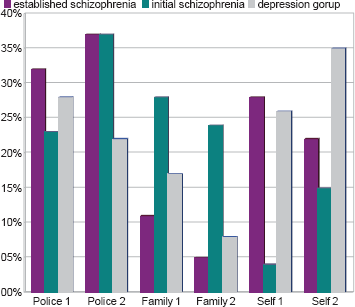
Referral pattern.
Reported compliance with prescribed medication was poor in 80.4 and 31 percent for patients with schizophrenia and depression respectively.
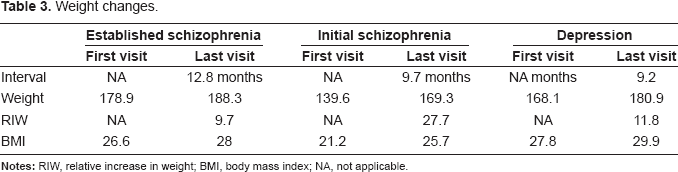
Weight Gain
Weight gain in the initial schizophrenia group who were naïve to antipsychotic therapy averaged 30 pounds (Table 3) after 9.2 months of treatment. This group gained more weight than either two groups (p < 0.01). There was also a statistically significant increase in weight from the first presentation to the second presentation in established schizophrenia group (from 179.9 lb to 188.3 lb, p < 0.001) and in depression group (from 168.1 to 180.9 lb, p < 0.001). Patients in the initial schizophrenia group had Body Mass Indices within normal limits at the first presentation, though this increased after a period of nine months. Patients in the other two groups experienced weight gain at a slower rate, and were on average overweight at first presentation (Fig. 2).
Weight changes.
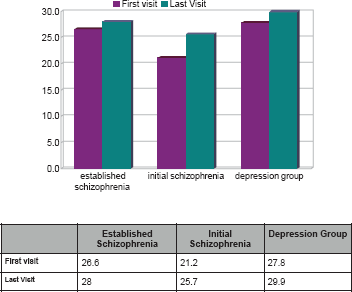
Body mass index dynamics.
Routine Laboratory Investigations
We find no predictable pattern between the groups in relation to the frequency of abnormal CBC panels for the different groups and presentation sequence. For example, a higher percentage of abnormal CBC was found in the first presentation of patients with schizophrenia when compared with the second presentation. However, in depression group, this pattern was reversed. The abnormalities reported were mainly in hematocrit and mean corpuscular volume.
BMP was more frequently abnormal at the first visit when compared to the last visit for all groups. The BMP reflected electrolyte imbalance (elevated or decreased sodium and potassium) in all groups, with more abnormalities found in schizophrenic patients. Liver function panel abnormalities were relatively equally distributed between groups.
None of the patients in any of the groups had a positive RPR titer.
Approximately one fourth of the patients in the three groups had positive UDS. No significant difference was found between the groups or presentations. Cannabis was the most frequent substance of abuse found by UDS in approximately 90% of patients who were positive. Cocaine was the second most common illicit substance used in combination with cannabis in both the schizophrenia group and depressed group, totaling 6% and 20% respectively of patients who were positive.
Depressed patients with thyroid abnormality were all noted to have hypothyroidism, as compared to both schizophrenia groups, which had patients with either hyperthyroidism or hypothyroidism (Table 4). After the routine thyroid panel was discontinued at our facility, none of the schizophrenic patients had this test ordered, where as the thyroid panel was inconsistently ordered in the depressed group, although the detection of thyroid function anomalies remained the same as compared to the first visit.
Abnormal laboratory results for patients with depression and schizophrenia.
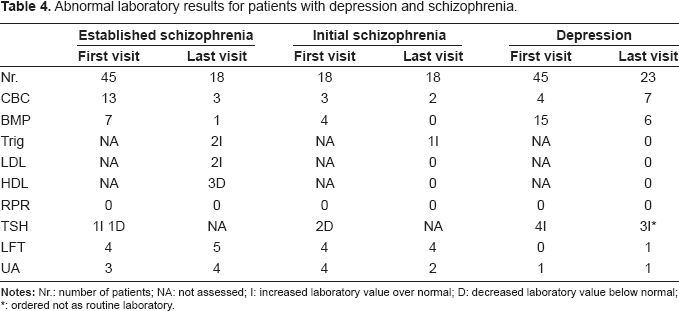
ordered not as routine laboratory.
At the first visit none of the patients had a lipid panel drawn. After this test was done routinely, we identified three of 18 and one of 13 patients with hyperlipidemia in the established and initial schizophrenia groups, respectively; while none of 23 patients with depression had an abnormal lipid panel.
Discussion
Monitoring of side effects to medication is mostly done in outpatient setting (Lamberti et al. 2006). However, in those settings interventions are often delayed due to various factors, such as the time lapsed until the psychiatrist receive the ordered laboratory results, interval between scheduled appointments and communication between psychiatrist and primary care physician (most psychiatrists do not routinely treat the medical conditions discovered, rather refers the patients to their primary care provider). Therefore, the investigations done during hospitalization provide a specific advantage, as patients diagnosed with laboratory abnormalities can have access to treatment of these conditions during the hospital stay fostering implementation of treatment immediately if indicated (Morgan D, 2008).
This study was done in a publicly funded state hospital serving a diverse indigent population. The most dramatic finding was the significant increase in weight for patients naïve to antipsychotic medication (initial diagnosis with schizophrenia), from an average of 139.6 to 169.3 lb. In patients with established diagnosis of schizophrenia this trend persisted but to a lower magnitude. There may be several explanations for this finding. First, the antipsychotic medications have an established side effect of weight gain, which may be more significant in patients without prior exposure to these agents. Secondly, patients with more frequent hospitalizations may require higher dose of medications, and in certain cases more than one agent to stabilize their condition. Also, patients with depression had the same trend, even though they started with higher BMI. AAP have an idiosyncratic (regardless of dose) weight gain side effect(Henderson, 2007). If weight gain is observed during the first weeks of treatment despite diet, exercise and adjustment of the dose, other interventions should be considered early, as the weight gain trend is likely to continue. However, the degrees of weight gain differ with different medications(Newcomer, 2007). There are several theories that try to account for the weight gain, including decreased degree of physical activity, histaminic considerations, degree of sedation, serotoninergic antagonism, possible hypothalamus involvement and increased appetite(Henderson, 2007). Interventions to limit and prevent weight gain should be instituted even before starting the medications (including education about diet, exercise and monitoring weight)(Henderson, 2008). Once the weight gain occur despite of preventive intervention, it is difficult to lose it. In terms of interventions, the most effective approach is to change medications(Casey et al. 2003). Also, several behavioral and pharmacological interventions have been described, with various successes.
Standard batteries of tests ordered at the time of admission have specific benefits in identification of treatable conditions. The discontinuation of standard thyroid panel did not decrease the rate of detection of hypothyroidism in patients with depression, as psychiatrists ordered these tests if indicated (hypothyroidism is a condition that it is known to mimic depressive symptoms or to exacerbate depressive disorder). That is not the case for either group of patients with schizophrenia, where TSH was not ordered at all at the last visits (when it was not included in the standard battery of tests). Introduction of the standard lipid panel, besides being standard of care, has lead to identification of 3 out 18 patients whom can benefit from lipid lowering medication. Out of more than 100 patients, none had a positive RPR titer, even though this test is routinely done in many inpatient facilities, due to the potential risk of treponema infection in inner-city patient population(Ernst, Farley, and Martin, 1995). It is debatable how often it should be done for the same patient at subsequent presentations.
UDS results.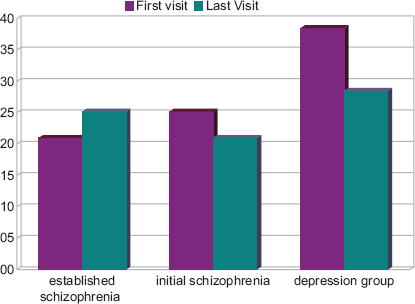
Study Limitations
This study has several limitations. One limitation of this study is typical of retrospective chart reviews, in that there was no control of racial and demographic distribution. A second limitation is sample size. Furthermore, because the mission of the hospital is public mental health services, and a patient population that is largely uninsured, our patients tend to use our facility for both acute inpatient treatment as well as outpatient-like services. Patients that were not admitted to the hospital did not have laboratory work done in majority of cases. In same situations, some of the patients who were hospitalized continued to refuse laboratory work through out their hospital stay. Also, due to the design of the study (long period of follow-up and multiple hospitalizations and medication changes) we could not look at specific correlation between individual psychotropic medication and metabolic implications.
Conclusion
Even in the managed care era, routine laboratory work has a necessary place in the practice of psychiatry. However, it adds to the cost of hospitalization. It is important to order studies rationally, and, in doing so, to also consider the pattern of seeking care of these specific patient populations, as they tend not to have a routine pattern of follow up. Our study shows that the addition of lipid profile and the discontinuation of thyroid panel saves money and at the same time helps to identify patients that may benefit from lipid lowering treatment.
Financial Disclosure
No Grant or financial contribution from outside sources was used for this project.
Proprietary Statement
None.
Institutional Review Board University of Missouri Kansas City and Department of Mental health has approved this study since 2002.