
Abstract
Objective
The objective of this study is to determine the correlation of Apgar score with asphyxial hepatic injury and neonatal mortality in moderately and severely asphyxiated newborns.
Material and Methods
This is a secondary analysis of our prospective observational case-controlled study. Sixteen neonates with severe birth asphyxia (five-minute Apgar ≤3) were compared with either 54 moderate asphyxia neonates (five-minute Apgar >3) or 30 normal neonates. Liver function tests were measured on postnatal days 1, 3, and 10 in the study and control groups. Neonatal mortality was observed in the study and control population.
Results
Correlation of Apgar score in severely asphyxiated neonates compared with normal Apgar score neonates and moderately asphyxiated neonates for deranged hepatic function showed significant correlation (odds ratio [OR] 4.88, 95% CI 3.26–5.84,
Conclusion
The severity of hepatic dysfunction correlates well with increasing severity of asphyxia. The neonatal mortality also showed good correlation with Apgar score in our study, although we need a large multicentric trial to confirm our observations. Apgar score combined with hepatic dysfunction can be used as a prognostication marker for neonatal mortality.
Keywords
Introduction
A recent study published in
Perinatal asphyxia is one of the leading causes of neonatal mortality in developing countries such as India15,18 when compared to perinatal asphyxia being cause of neonatal mortality in developed countries.
19
In addition, perinatal asphyxia causes an even more number of children to develop neurological sequelae. The clinical signs following perinatal asphyxia have been called hypoxic–ischemic encephalopathy (HIE). HIE is multisystem involvement such as brain (seizures both clinical and electroencephalography [EEG] proven, neonatal encephalopathy, stupor, and coma),
20
renal,
21
hepatic, cardiovascular, pulmonary, and hematological,22,23 although isolated nervous system involvement is also seen.
24
Various biochemical markers have been used to find out organ dysfunction.
25
The standard definition of perinatal hypoxia as described by the AAP includes when a neonate demonstrates all of the following: (a) profound metabolic or mixed acidemia (pH <7.00) on an umbilical arterial blood sample, if obtained, (b) an Apgar score of 0–3 for longer than five minutes, (c) neurologic manifestation, EEG, seizure, coma, or hypotonia, and (d) evidence of multiorgan dysfunction.
26
The other criteria that have defined asphyxia and have included HIE as a cause of neonatal encephalopathy include (a) prolonged (>1 hour) antenatal acidosis, (b) fetal heart rate less than 60 beats/min, (c) Apgar score ≤3 at ≥10 minutes, (d) need for positive pressure ventilation for >1 minute or first cry delayed for >5 minutes, (e) seizures within 12–24 hours of birth, and (f) burst suppression or suppressed background pattern on EEG or amplitude integrated EEG.
27
Hepatic dysfunction is usually seen in these asphyxiated newborns as liver is the site of innumerable metabolic processes. There is usually an early, abrupt, and transient (within 24–72 hours after) increase in various hepatic enzymes, namely aspartate transaminase (AST), alanine transaminase (ALT), alkaline phosphatase (ALP), and lactate dehydrogenase (LDH). Usually, this increase returns to baseline within 10 days after birth.
28
A recent study published in
Material and Methods
This is a secondary analysis of our study, in which we have compared and correlated the hepatic dysfunction on the basis of five-minute Apgar score in newborns with severe asphyxia with newborns with moderate asphyxia and normal control neonates. 30 We also compared the five-minute Apgar score correlation with neonatal mortality in severely and moderately asphyxiated neonates.
This prospective observational case-controlled study was conducted in the neonatal intensive care unit of Umaid Hospital, Tertiary care hospital in Jodhpur, India, over a period from January 2011 to December 2011. The study was approved by the institutional research board (IRB) of S.N. Medical College, Jodhpur, Rajasthan, India. A convenient sample of 100 full-term intramural neonates (retrospective data of last one year regarding intramural neonates with moderate and severe asphyxia were analyzed) was taken. These neonates were enrolled in the study after taking written parental consent. The study population had two groups, study group A (case) comprised 70 newborns, suffering from birth asphyxia, ie, an Apgar score of 7 or less at five minutes, while control arm (group B) had 30 healthy newborns with Apgar score more than 7 at five minutes. Neonates were further sorted according to Apgar score at five minutes as mild (6 and 7), moderate (4 and 5), or severe (3 or less) and graded into HIE stages by the Sarnath and Sarnath staging system. 31 The exclusion criteria included neonates having a congenital malformation or a primary disease of liver or bacterial sepsis or receiving potentially hepatotoxic drug therapy.
Full medical history, including perinatal history, especially the history of anesthesia during cesarean section and drug intake by mother or infant with detail clinical and neurological examination laying stress on abdominal examination with the exception of newborns with liver disease or neonatal sepsis, were noted. All biochemical parameters of liver function, ie, the serum ALT (normal value 6–50 U/L), AST (normal value 35–140 U/L), ALP (normal value 150–400 U/L), LDH (normal value 160–450 U/L), total protein (normal value 4.5–8.4 g/dL), serum albumin (normal value 2.5–3.6 g/dL), bilirubin (total and direct; normal value <2 mg/dL), prothrombin time (PT; normal value 10–16.2 seconds), and International Normalized Ratio (INR; normal value 1.1–1.2) were measured postnatal days 1, 3, and 10 in both study and control groups. Normal cutoff values were taken as per neonatal reference normogram. Liver was observed for congenital malformation or abnormality of biliary tract within 24 hours of birth by an ultrasound. Newborn infants who developed liver dysfunction were managed conservatively as per the standard hospital protocol. The management of asphyxiated neonates involved monitoring of seizure and also maintenance of normal metabolic milieu, including glucose, serum electrolytes, acidosis, pH, and calcium. The neonate shock was managed with vasopressors, and target was blood pressure at 50 centile as per gestational age. 32 The neonatal seizures were managed with phenobarbitone (maximum loading of 20 mg/kg and minimum loading of 10 mg/kg followed by maintenance dose of 3–5 mg/kg/day) and Phenytoin (maximum loading of 20 mg/kg and maintenance dose of 5–8 mg per kg/day) as second line of anticonvulsants. Anticonvulsants were started after ruling out any metabolic abnormality. Any neonate with severe respiratory distress and respiratory failure was given invasive ventilation as per the unit policy. All neonates underwent head ultrasound at the time of discharge. The criteria for liver impairment were ALT >50 U/L, AST >140 U/L, ALP >420 U/L, LDH >580 U/L, total protein <4.5 g/dL, serum albumin <2.5 g/dL, PT >20 seconds, and INR >1.2.
Statistical calculation
All the data were entered in Microsoft excel sheet, and statistical analysis was executed using SPSS version 21 for windows. The asphyxiated newborns with five-minute Apgar score less than 3 (severe asphyxia) were compared with moderate asphyxiated newborns with Apgar score (4 and 5) and also with normal neonates (>7) that acted as control. Various liver function tests (ALT, AST, LDH, ALP, PT, INR, serum albumin, total bilirubin, and direct bilirubin) and neonatal mortality were compared between each group. Student's
Results
Out of 70 asphyxiated newborns, 16 newborns had severe birth asphyxia and remaining had moderate birth asphyxia. Thirty healthy newborns with normal Apgar score acted as control.
The mean weight of neonates in severe asphyxia group was 2.90 ± 0.34 kg, which was not statistically significant compared with neonates with moderate asphyxia (3.06 ± 0.36 kg) and also when compared with normal neonates (2.90 ± 0.30 kg).
The mean gestational age in severe asphyxia group was 38.02 ± 0.8 weeks, whereas the mean gestational age in the moderate asphyxia and control group was 38.60 ± 0.6 weeks and 38.52 ± 0.5 weeks, respectively (
On comparing the various liver function tests between severely asphyxiated newborns (five-minute Apgar score ≤3) versus newborns with moderate asphyxia (five-minute Apgar score 4 and 5), at age of first day, third day, and tenth day, there was significant increase in serum LDH (Fig. 1) and total bilirubin on day 1 with other liver function test being not significantly deranged. On day 3, there was significant decrease in total bilirubin and serum albumin (Fig. 2) and there was trend toward significant decrease in direct bilirubin level. At age of 10 days, there was significant increase in serum LDH level (Fig. 1; Table 1).

Comparison of serum lactate dehydrogenase (LDH) in neonates with severe asphyxia, with moderate asphyxia, and severe asphyxia with normal control (*significant difference between I and II and Significant difference between I and III).
Comparing the various liver function tests between newborns with severe asphyxia and moderate asphyxia, and severe asphyxia and normal neonates at age of first day, third day and tenth day.
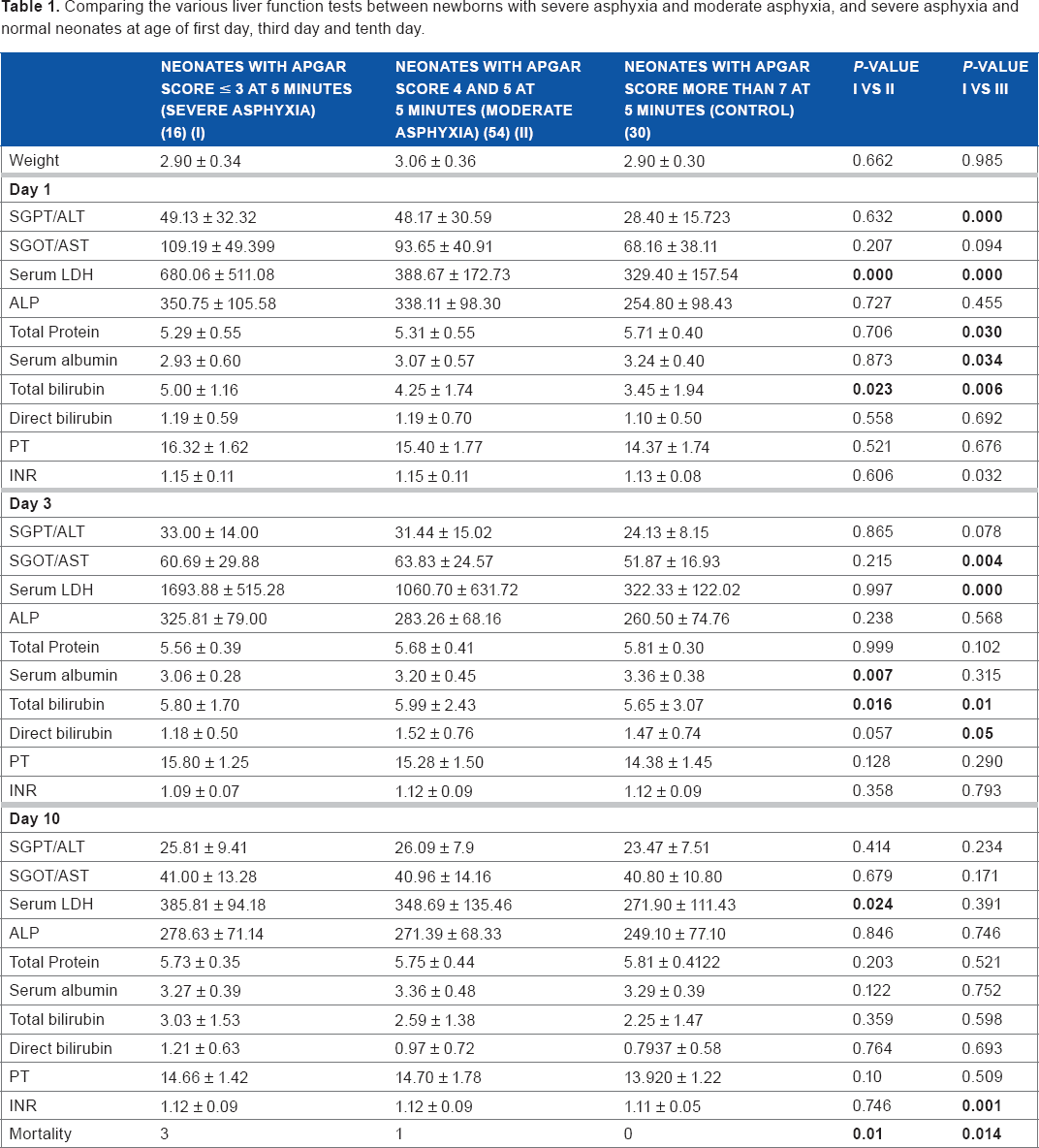
The comparison of various liver function tests between newborns with Apgar score ≤3 (severe asphyxia) versus normal control newborns at age of one, three, and tenth postnatal life showed that on day 1, there was significant increase in serum ALT (Fig. 3), serum LDH (Fig. 1), and total bilirubin, whereas there was significant reduction in total protein and serum albumin (Fig. 2). At postnatal age of three days, there was significant increase in serum AST (Fig. 3), serum LDH (Fig. 1), and total bilirubin and also there was significant reduction in direct bilirubin. At age of day 10, there was a significant difference in only INR that showed increased INR in severely asphyxiated neonates (Fig. 4; Table 1).

Comparison of total protein and serum albumin in neonates with severe asphyxia, with moderate asphyxia, and severe asphyxia with normal control (*significant difference between I and II and #significant difference between I and III).
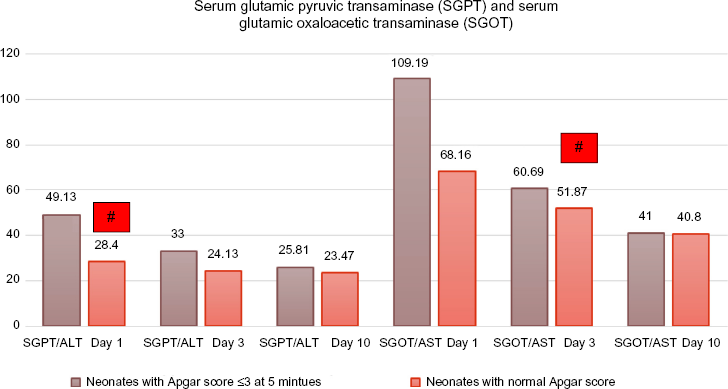
Comparison of serum glutamic pyruvic transaminase (SGPT)/alaninine transferase (ALT) and serum glutamic oxaloacetic transaminase (SGOT)/aspartate transferase (AST) in neonates with severe asphyxia and control (#significant difference).

Comparison of International Normalized Ratio (INR) in neonates with severe asphyxia and normal control (#significant difference).
There was a significant increase in neonatal mortality in neonates with severe asphyxia in comparison to moderate asphyxia neonates and normal Apgar neonates (Table 1). Correlation of Apgar score in severely asphyxiated neonates compared with normal Apgar score neonates and moderately asphyxiated neonates for neonatal mortality showed significant correlation (odds ratio [OR] 2.23, 95% CI 1.42–3.04,
Discussion
Perinatal asphyxia is an insult to the fetus or the newborn due to lack of oxygen and/or lack of perfusion to various organs of the body. Neonatal birth asphyxia is a multisystem disorder and involves almost all organs of body in one way or other. The liver also exhibits different biochemical and histopathological changes secondary to asphyxia. Birth asphyxia in newborn infants can cause hepatic hypoxic injury, leading to release of intracellular enzymes and significant increase in their level.22,23 The aim of present study was to evaluate the severity and type of liver dysfunction in relation to Apgar score and HIE grading of asphyxiated neonates and also to determine the correlation with neonatal mortality.
We reported that in severely asphyxiated neonates on day 1, serum LDH and bilirubin can be used as markers to assess the severity of hepatic injury, whereas on day 3, decrease in serum albumin can be used. As liver injury will lead to decrease in synthetic function, leading to significant decrease in albumin level, whereas on day 10, serum LDH can be used to assess the degree of liver injury. Neonatal mortality is significantly increased in condition of asphyxia, where the newborns have five-minute Apgar score less than 3, which matches with the recent study published in
Islam et al performed a prospective study of 70 full-term asphyxiated newborns. Venous blood was analyzed between second and fifth days of life to estimate serum AST, ALT, ALP, serum total bilirubin, serum total protein (STP), serum albumin, and PT The mean AST, ALT, ALP, STP, serum albumin, and TSB of asphyxiated babies were 76.3 ± 37.4 U/L, 82.2 ± 48.08 U/L, 369.6 ± 123.05 U/L, 55.7 ± 8.8 U/L, 32.6 ± 5.5 g/L, and 5.5 ± 2.01 mg/dL, respectively, and those of normal babies were 23.5 ± 8.5 U/L, 26.5 ± 7.8 U/L, 208.2 ± 46.9 U/L, 66.3 ± 10.4 g/L, 40.9 ± 6.5 g/L, and 4.5 ± 1.2 mg/dL, respectively, and these differences were statistically significant (
Karlsson et al conducted study to investigate the occurrence of hypoxic hepatitis in full-term infants after birth asphyxia and the temporal enzyme pattern in asphyxiated newborn infants. AST, ALT, LDH, gamma-glutamyl transferase, total and conjugated bilirubin, Cholinesterase activity, albumin, INR, and nucleated red blood cell count were prospectively measured in 26 full-term asphyxiated newborns. Samples were collected three times during the first 72 hours and once between days 6 and 12 after birth. Fifty-six healthy newborns acted as control whose sample were collected 24–172 hours after birth. They reported increase in ALT, AST, and LDH in asphyxiated neonates and hence concluded that birth asphyxia can induce an enzyme pattern in serum compatible to hypoxic hepatitis. 34 The results of the present study also showed increase in hepatic enzymes in asphyxiated neonates.
A recent published study by Karlsson et al assessed whether LDH, ALT, and AST during the first 12 hours after birth predict HIE and adverse neurodevelopment outcome in newborn term infants with intrapartum signs of fetal distress. The authors reported that a cutoff level of 1049 U/L for LDH was not only the best predictor of HIE (sensitivity 100% and specificity 97%) but was also useful for long-term outcome after HIE. 35 The same findings were reported by Thoresen et al in which they predicted serum LDH as a novel biomarker, with a high negative predictive value in the assessment of outcome in therapeutic hypothermia-treated asphyxiated term infants. 36 We too reported significant increase in serum LDH level in comparison to normal neonate, and the increase was more in neonates who had severe asphyxia in comparison to neonates with moderate asphyxia. In the present study, neurodevelopmental outcome was not seen in relation to Apgar score severity.
In another recent well-conducted study by Chhavi et al that sought serum liver enzyme pattern in birth asphyxia-associated liver injury, enrolled 60 controls and 62 cases singleton term newborns with birth asphyxia and ≤72 hours of age. Serum liver enzymes were measured at <24 hours, 24–72 hours, and at 6–12 days of age for cases and at 1–6 days of age for controls. They reported asphyxiated newborns had higher serum levels of ALT, AST, and LDH than the control infants, with peak at 24–72 hours followed by a sharp decline by 6–12 days of age. 37 The results were similar to our study but there was no differentiation between moderate and severe asphyxia.
Sánchez-Nava et al conducted a study in 120 newborns, which were placed into two groups: group 1 of the asphyxiated neonates who were given oxygen at intermittent positive pressure for more than a minute and group 2 of healthy neonates with an Apgar greater than 7 after the first and five minutes and without any apparent pathology. Their results showed a real increase in level of all three transaminases (ALT, AST, and LDH) in the asphyxiated neonates, while on the other hand, this increase was not seen in the normal neonates. There were statistical differences between the two group by which they conclude that the quantification of these enzymes can be useful as a diagnostic tool in cases of perinatal asphyxia. 38 These findings were comparable with our study results.
There are many other studies in asphyxiated neonates, which have studied hepatic dysfunction in asphyxiated neonates28,39–47 but we could not find any study that has correlated the hepatic dysfunction in moderately and severely asphyxiated neonates on the basis of five-minute Apgar score.
Limitation of the Study
Number of infants having severe asphyxia was small (16 babies) that can make safe statistical conclusions difficult.
We took Apgar score criteria for labeling as asphyxia and we did not include all criteria of AAP for labeling them as perinatal asphyxia
Long-term neurodevelopmental outcome was not assessed to see the correlation between severity of hepatic dysfunction and neurodevelopmental outcome.
Elevation of transaminases may have been influenced by use of drugs such as phenobarbitone or phenytoin in some patients, which was not differentiated.
No correlation of markers of hepatic health was seen with other markers of stress in patients such as acidosis, ventilation, and neonatal seizures.
Conclusion
In perinatal asphyxia, multiple organ systems are damaged secondary to birth asphyxia in neonates, which includes hepatic, renal, hematological, pulmonary, cardiovascular, and nervous systems. The hepatic injury may represent a useful marker for assessment of severity of degree of asphyxial injury (when the neurologic examination is unreliable or misleading). Liver dysfunction in asphyxiated neonates is significant problem and is usually seen in majority of the cases. Hepatic dysfunction in majority of neonates manifest as raised hepatic enzymes, including AST, ALT, LDH, and bilirubin. The severity of dysfunction correlates well with increasing severity of asphyxia and correlates well with poor Apgar score, although we need to do a large multicentric trail to confirm our observations. Apgar score combined with hepatic dysfunction can be used as a prognostication marker for neonatal mortality in infants with severe asphyxia. We should keep a high index of suspicion of hepatic dysfunction in asphyxiated newborn, and all the asphyxiated neonates should be routinely screened for hepatic impairment. Biochemical parameters although, normalized on follow-up, the subtle parenchymal damage and alterations at molecular level may affect liver functions in future life, which require continuous long-term follow-up of these neonates for both hepatic and neurodevelopmental outcomes.
Author Contributions
Conceived and designed the experiments: MC, DS. Analyzed the data: DS, SS. Wrote the first draft of the manuscript: MC, DS. Contributed to the writing of the manuscript: ML, SS. Agree with manuscript results and conclusions: MC, DS, ML, SS. Jointly developed the structure and arguments for the paper: SS. Made critical revisions and approved final version: MC, DS, ML, SS. All authors reviewed and approved of the final manuscript.