
Abstract
Background:
Globally, neonatal mortality remains a serious catastrophic problem for newborns, particularly in a low-resource setting. There were no neonatal mortality trend studies in the study area.
Objective:
This study aimed to determine the trends and risk factors of neonatal mortality at the neonatal intensive care unit of Felege Hiwot Comprehensive Specialized Hospital, Northwest Ethiopia.
Methods:
An institution-based retrospective cross-sectional study was conducted among 870 admitted neonates from January 1, 2016 to December 31, 2020 in the neonatal intensive care unit by a stratified simple random sampling technique. Data were entered into EpiData and then exported to STATA 14.0 for analysis. A linear regression statistical model was used for trend analysis and binary logistic regression was carried out to identify explanatory variables of neonatal mortality.
Results:
Overall, neonatal mortality averagely increased by 2.1% per year throughout the 5 consecutive years. In this study, rural residency [adjusted odds ratio (AOR): 1.96, 95% confidence interval (CI): (1.26, 3.06)], birth asphyxia (AOR: 7.73, 95% CI: 4.31, 13.84), congenital deformity (AOR: 3.61, 95% CI: 1.17, 11.18), low birth weight (AOR: 2.13, 95% CI: 1.23, 3.67), respiratory distress syndrome (AOR: 3.32, 95% CI: 1.97, 5.59), Ambu-bag resuscitation (AOR: 0.16, 95% CI: 0.07, 0.38), taking antibiotics (AOR: 0.50, 95% CI: 0.27, 0.90), glucose (AOR: 0.47, 95% CI: 0.30, 0.72), and oxygen (AOR: 0.26, 95% CI: 0.16, 0.41) were associated with neonatal mortality.
Conclusions:
This 5-year trend analysis revealed an increased trend of NMR, indicating more work is still needed to make progress toward meeting the SDG goal by 2030. Rural residency, birth asphyxia, congenital deformity, low birth weight, respiratory distress syndrome, Ambu-bag resuscitation, taking antibiotics, glucose, and oxygen were associated with neonatal mortality. Therefore, all stakeholders shall give due attention to reducing this timely-increasing trend of neonatal mortality.
Background
Neonatal mortality (NM) is the term used to describe fatalities that occur within the first 4 weeks of life after birth. 1 Early neonatal mortality (ENM) and late neonatal mortality (LNM) are the 2 categories of neonatal mortality that refer to deaths that occur within the first 7 days of life and between 8 and 28 days following birth, respectively.2,3
Neonatal mortality was a substantial contributor to morbidity and mortality in children under the age of 5 years, particularly high in low-income countries including Ethiopia. Numerous factors might have contributed to NM. Poor power of women to seek healthcare, women’s low habit of postnatal visits, giving birth at home, delayed breastfeeding after birth, and giving multiple births were all linked to a higher likelihood of NM. 4 In addition to these, neonatal sepsis, birth asphyxia, low birth weight, prematurity, mode of delivery, meconium staining, neonatal medical, and congenital-related causes are also having a large contribution to NM.5,6
Global and national strategies were designed to reduce NM. For instance, the Sustainable Development Goals (SDGs) have been applied internationally since 2016. The country, Ethiopia, adapted a national preventive strategy of NM in line with a United Nations health agenda. Ethiopia designed a National Strategy for Newborn and Child Survival in June 2015 with an ambitious vision of reducing the NMR from 28 to 11/1000 by 2019/2020. To soundly achieve the above vision and goals of the country, the provision of high-quality healthcare is essential for mothers, infants, and children, and it will be successfully practiced to reduce the impact of NM. 7
Although attempts to reduce NM have been made gradually since 1990, more efforts were still required, to achieve a national and global neonatal health agenda. 8 Given that, NM must be adequately addressed to achieve the SDGs aim since it continues to be a major national and global health concern. 9 Globally, NM currently contributes to two-thirds of under-5, and childhood mortality. 10 It is estimated that 2.5 million newborns died within their first month of life, equating to almost 7000 deaths every day. 11
Though global trends in neonate mortality have shown progress Sub-Saharan Africa has made the weakest progress in lowering neonatal death rates. 12 For instance, Sub-Saharan Africa (SSA) together with South Asia accounted for 79 percent of all neonatal deaths at the country level, with SSA having the highest NMR 13 and of the 20 countries with the greatest risk of neonatal death worldwide, 75% are in Africa. 14 Additionally, a recent study found that the yearly NMR in developing countries was 9 times greater than that of developed countries. 8
In Ethiopia, NM accounted for 42% of all deaths in children under the age of 5 years. 15 Despite making great strides, Ethiopia continues to have one of the highest NMRs in the world, ranking among the 10 countries that account for two-thirds of all newborn deaths globally and among the 6 that account for half of all deaths among children under the age of 5 years.15-17
Readers bear in mind that NM reported in the neonatal intensive care unit (NICU) was a subcomponent of NM reports in the general population. In a study done in Amhara Regional State in 2018, NMR in the NICU was 186 per 1000 admitted neonates which was very high as compared with a study conducted in different regions of the country, Ethiopia. 18 An occasional report in 2019/20 from the NICU of Felege Hiwot Comprehensive Specialized Hospital (FHCSH), implied that NM was raised gradually. 19 This makes it impossible to accomplish the 2030 health agenda unless this real problem was timely identified and genuine evidence-based scientific solutions were made. Though NM reports from all over the world and SSA showed a considerable decline, EDHS 2019 and occasional annual reporting in FHCSH revealed a rise.17,20 This calls for attention to be given to meet SDG 3.2’s goal of reducing NMR to 12 deaths per 1000 live births by 2030. 9
Not only these but also there were no clear progressive NM trend studies in the NICU across the country including our study area, and no one could not deny that the issue needs validation. As a result, designing a title that addresses these specific objectives like; trends and associated factors of neonatal mortality rate at the neonatal intensive care unit of Felege Hiwot Comprehensive Specialized Hospital from January 1, 2016 to December 31, 2020, in Bahir Dar, Northwest Ethiopia, 2021 was compulsory. Additionally, results obtained from this study will help programmers to evaluate their efforts toward the goal of SDG. Furthermore, this study will serve as baseline information for further studies.
Methods and Materials
Study design, setting, and population
An institution-based retrospective cross-sectional study was conducted at the NICU of FHCSH from January 1, 2016, to December 31, 2020, in Bahir Dar city, Northwest Ethiopia. Bahir Dar is the capital city of Amhara Regional State which is located 565 km away from Addis Ababa, the capital city of Ethiopia. 21 In this hospital, the pediatrics NICU had 4 sub-departmental units (ie, preterm unit, KMC unit, mother side unit, and septic unit), containing 20, 20, 30, and 10 beds respectively. In these sub departmental units there were a total of 1300, 1380, 1040, 2660, and and 2020 admitted neonates in the year 2016, 2017, 2018, 2019, and 2022 respectively. All medical records of admitted neonates in the NICU of FHCSH were considered as source population where as those who were eligible and randomly selected medical records of neonates were included in the study. However, medical records of neonates with incomplete and lack of pertinent information were excluded from the study.
Sample size determination
The sample size was calculated by using the smallest AOR of the previous study at NICU 22 by using the following formula:

Where: N = total sample size; E = required number of events (death); P(E) = the probability of an event (death) obtained from the previous study is 0.17; Zβ = the power of the study, the area under the normal curve for the value of β (power = 80%), Zβ = 0.84; OR = Odd Ratio. After the substitution of each value in the following formula:
E =
(ln 1.58)2
Then, N = 148/0.17 = 870. Therefore, the total sample size was 870 neonatal medical records.
Sampling technique
Initially, eligible neonates’ medical registration numbers (MRN) from January 1, 2016 to December 31, 2020 were taken from registration book. Then, we list out every month’s MRN and their corresponding index serial numbers in Excel and SPSS. Finally, eligible MRNs were generated through a random computer generation system. A stratified simple random sampling technique was employed step by step in the subsequent months using MRN as a sampling frame. After this, when the records of neonates had no pertinent information inside were randomly replaced by withdrawal of cards. Again, if it has no any information inside for the second time, withdrawal of the second card without replacement of the first card by simple random was carried out. Based on simple random sampling without replacement (SRSWOR) sampling technique, 15 neonatal medical records were replaced. According to the data obtained from FHCSH, the total number of admissions from 2016 to 2020 was 8400. A random computer generation system with a stratified simple random sampling technique was employed after proportionally allocated. The reason for performing proportional allocation and random sampling for every month separately was, for the sake of handling trend data, to make chronologically arranged and uniform distributions of the study units in each month.
Variables
Neonatal mortality is the outcome variable and variables listed under neonatal-related factors were; calculated gestational age at birth, sex of the neonate, birth weight, and maternal-related factors including maternal place of residence, mode of delivery, place of delivery, maternal Human immunodeficiency virus (HIV) status, maternal positive laboratory results like hepatitis B virus (HBV) and hepatitis C virus (HCV) infection as well as venereal disease research laboratory (VDRL) tests. In addition to these, variables that were listed under neonatal medical condition-related factors were; respiratory distress syndrome, birth asphyxia, sepsis, and congenital malformation. Finally, variables that were grouped under the type of treatment given were; Ambu-bag resuscitation, antibiotics, anticonvulsants, glucose, oxygen, blood transfusion, and thermal care were independent predictor factors of neonatal death.
Operational definitions
Maternal laboratory results: VDRL, HBV, and HCV test results.
Gestational age: intrauterine fetal age was measured from the beginning of the woman’s last menstrual period until the time of birth or based on ultrasound estimation.
Mode of delivery: were classified as cesarean section and vaginal delivery (including both spontaneous and assisted delivery).
Birth weight: classified as normal birth weight if a weight of a newborn is greater than 2500 g, low birth weight if below 2500 g, and macrosomic if above 4000 g based on WHO classification. Other causes of neonatal admission include meningitis, meconium aspiration syndrome, anemia, small bowel obstruction, large bowel obstruction, jaundice, and thermal burns.
Data collection tools and procedures
The data extraction checklist was adapted from the NICU registration books and reviewed from different kinds of literature which were conducted previously. 24 The data was extracted from NICU medical registration books and neonatal medical charts by 2 trained BSc nurses.
Data processing and analysis
First, the data was coded and edited after that checked for its completeness and consistency, and then entered into EpiData version 3.1 and exported to STATA 14.0. Finally, binary logistic regression was carried out to identify the associated factors of NM. Trends in the overall neonatal mortality were numerically calculated as the average increment minus average reduction of the consecutive years divided by 5 years. Descriptive statistics were used to measure the characteristics of the study variables. In addition, trend analysis with linear regression statistical model was used to show the 5 years neonatal mortality trends in the NICU. All variables with P < .2 in the bivariable analysis were included in the final model of multivariable analysis to control all possible confounders. Finally, the AOR with 95% CI was computed and variables with a P-value less than .05 in the multivariable simple logistic regression model were taken as significant risk factors of NM.
Data quality assurance
To assure data quality, a 1-day training was given for the 2 data collectors and a supervisor. The data was checked daily to reduce incompleteness and inconsistency by the principal investigator. Feedback and corrective actions were taken upon review of the daily submitted data.
Ethical consideration
Ethical clearance was obtained from the Institutional Review Board of Bahir Dar University with an approval number med287/2021. After discussing the purpose and method of the study, verbal informed consent was obtained from Felege Hiwot Comprehensive Specialized Hospital official bodies before collecting data. Since the study used secondary data from the registration logbook informed consent for the participants was waived by the Ethical Review Committee of school of Public Health, College of Medicine and Health Science, Bahir Dar University. No identifying information were indicated on the checklists, and confidentiality was assured throughout the study.
Results
Study population characteristics
A total of 870 admitted neonates were included in the study. Among these admitted neonates, more than 57% were male, and about 37% were low birth weights. Again, about 38%, 60%, and 2% were preterm, term, and post-term in gestational age at delivery.
Maternal characteristics
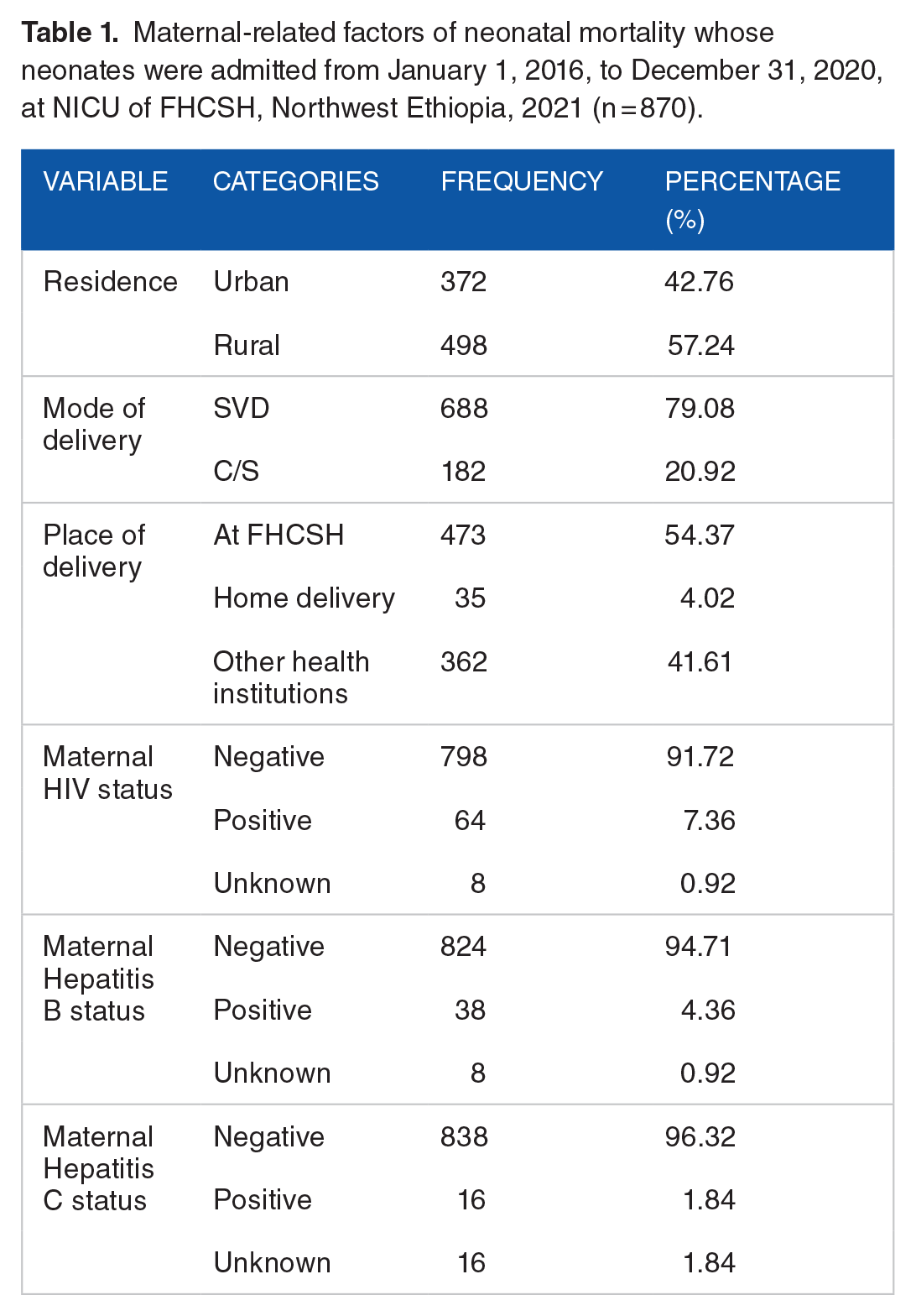
Among 870 women, 57.24% were from rural areas and 7.36% among all women were HIV positive (Table 1).
Maternal-related factors of neonatal mortality whose neonates were admitted from January 1, 2016, to December 31, 2020, at NICU of FHCSH, Northwest Ethiopia, 2021 (n = 870).
Causes of neonatal admission and death
Among NICU-admitted neonates, the leading cause of neonatal admission was sepsis (77.82%), whereas the least cause of admission was congenital malformation (3.10%; Table 2). Sepsis was the leading cause of neonatal death (29%), and the least (1%) cause was congenital malformation (Figure 1).
Causes of neonatal admission among neonates admitted at NICU of FHCSH, Northwest Ethiopia, 2021 (n = 870).

Other causes of neonatal admission includes; meningitis, meconium aspiration syndrome, anemia, small bowel obstruction, large bowel obstruction, jaundice, and thermal burn.

Neonatal death and their causes among neonates admitted at the NICU of FHCSH, in Bahir Dar, Northwest Ethiopia, 2021 (n = 870).
Neonatal treatment-related characteristics
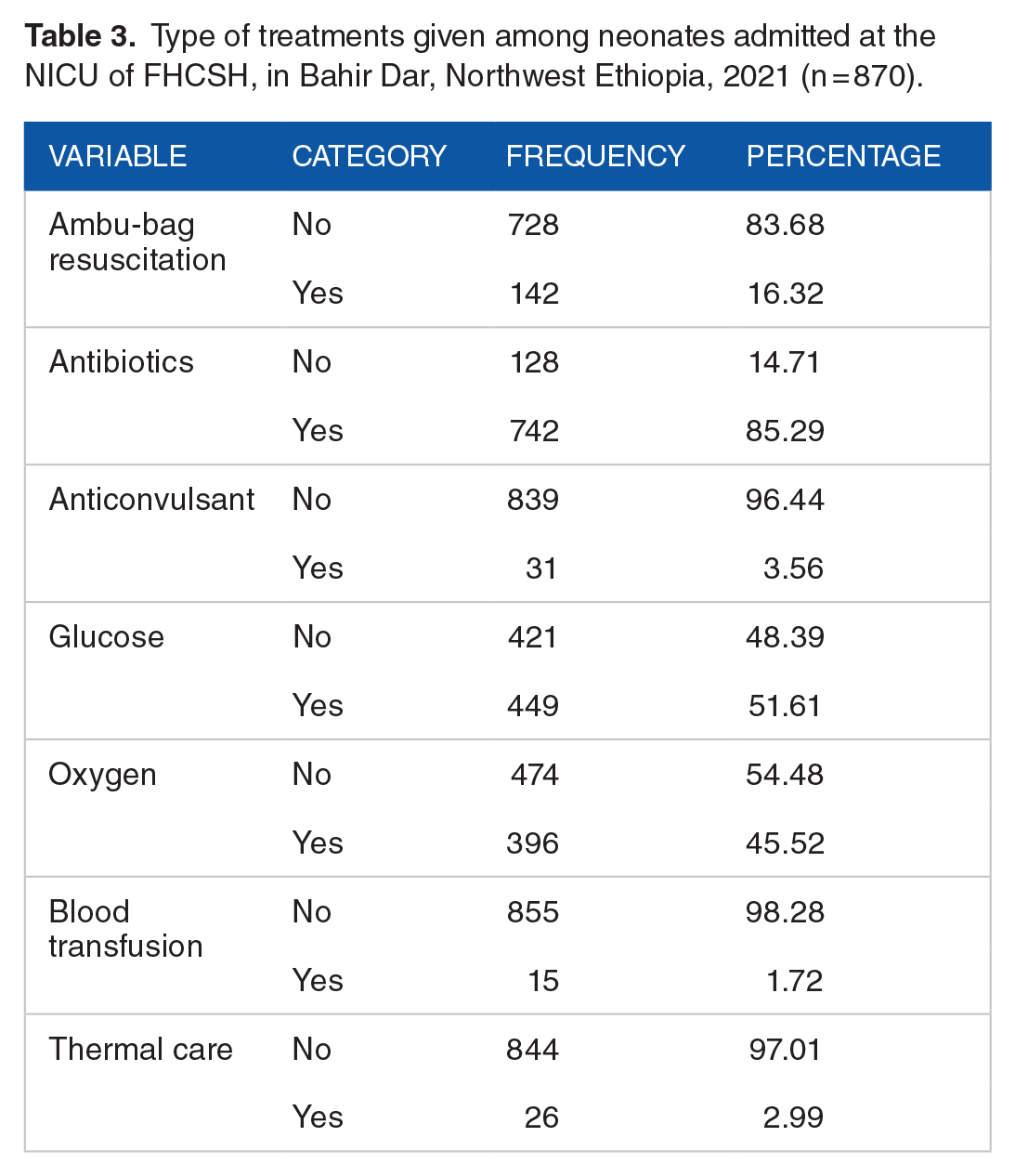
Among 870 neonates, the highest number of neonates were treated with antibiotics and the least number of neonates were treated by blood transfusion (Table 3).
Type of treatments given among neonates admitted at the NICU of FHCSH, in Bahir Dar, Northwest Ethiopia, 2021 (n = 870).
Proportion of neonatal mortality
Among 870 neonates, 190 (21.80%) of them died during the study period at the NICU of FHCSH. Therefore, the cumulative incidence rate was 218 per 1000 admitted neonates.
Trends of neonatal mortality from 2016 to 2020
In this 5 years trend graph in the 12 months moving average trend graph, the average reduction of NM from 2016 to 2017 was 16% and from 2017 to 2018 was 17%, while the average increment of NM from 2018 to 2019 was 19% and from 2019 to 2020 was 35%. As a result, to clearly understand, the overall NMR at the NICU was numerically calculated as the average increment minus average reduction divided by 5 years [(ie, 0.35 + 0.19/2) − (0.17 + 0.16/2)]/5 years which is equal to 2.1%. Therefore, the average increment of NMR from 2016 to 2020 was 2.1% per year. As shown in the graph in (Figure 2), the 12 months moving average trend graph from 2016 to 2020, clearly showed the increasing trends of NM after making 12 months per moving average. As a result, the thin red moving average trend graph was nearly overlapped with the red thicker linear line trend graph after taking 12 months of the central moving average.
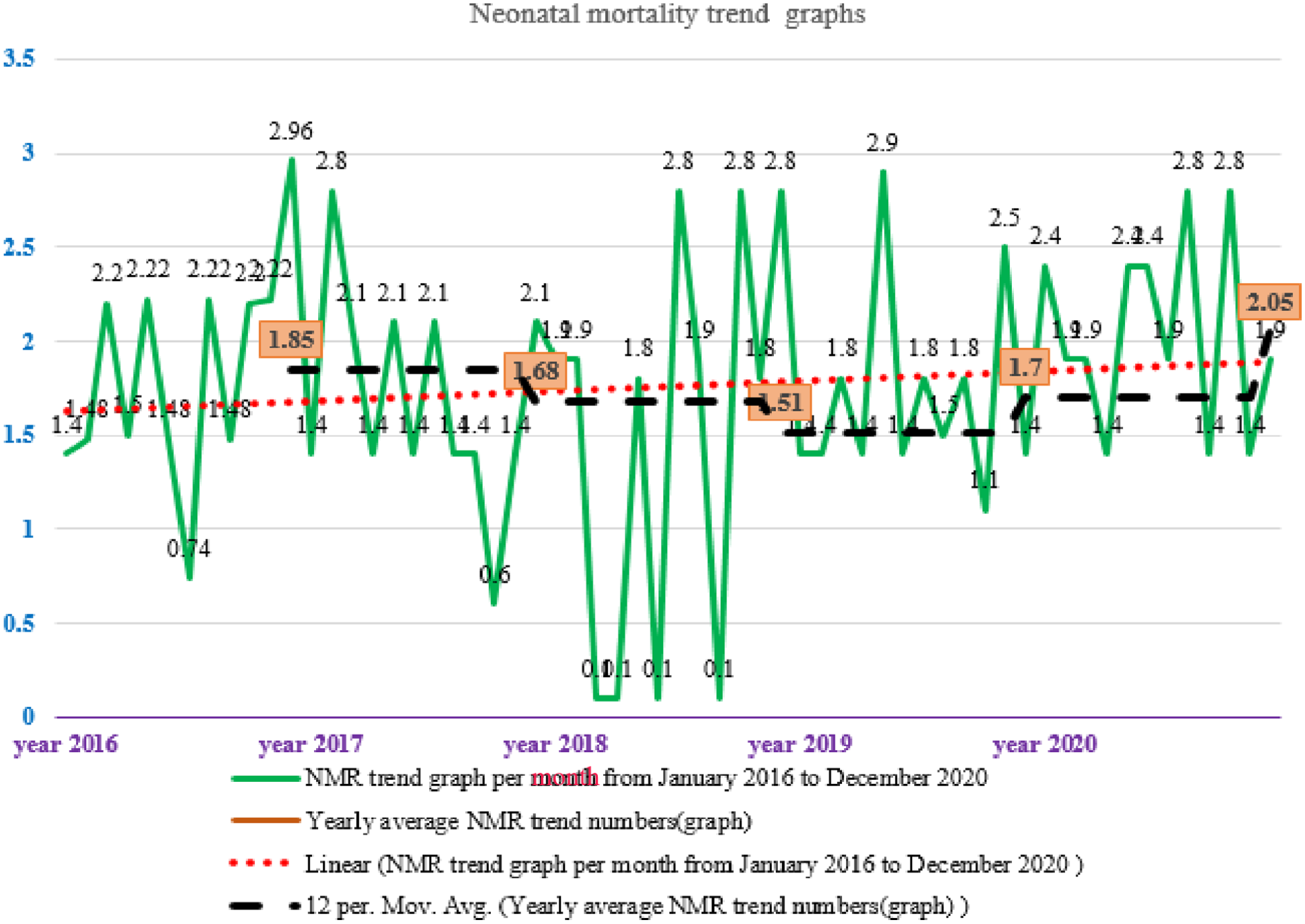
Trends of NMR based on 12 months per MA among neonates admitted at the NICU of FHCSH from 2016 to 2020, Bahir Dar, Northwest Ethiopia, 2021 (n = 870).
Risk factors of neonatal mortality
Logistic regression analysis was employed to select the statistically significant variables. The following 22 variables; residence, sex, mode of delivery, place of delivery, maternal HIV status, maternal hepatitis B virus, maternal hepatitis C virus, maternal VDRL, gestational age of neonate at birth, presence of prematurity, presence of sepsis, presence of birth asphyxia, presence of congenital deformity, presence of low birth weight, presence of RDS, giving of Ambu-bag resuscitation, antibiotics, anticonvulsant, glucose, oxygen therapy, blood transfusion, and thermal care were entered into bi-variable analysis. In the final model, only 9 variables such as; place of residence, presence of birth, asphyxia, presence of congenital deformity, presence of low birth weight, presence of RDS, Ambu-bag resuscitation, antibiotics given, glucose, and oxygen therapy were statistically significant risk factors of neonatal mortality with a P-value of less than .05 at 95% CI.
The odds of death of neonates who came from rural areas were 1.96 times (AOR: 1.96, 95% CI: 1.26, 3.06) compared to urban areas by keeping other factors constant. Moreover, neonates admitted with birth asphyxia was 7.73 times the odds of death (AOR: 7.73, 95% CI: 4.31, 13.84) as compared with health institution delivery. Furthermore, the odds of death of neonates admitted due to congenital deformity were 3.61 times (AOR: 3.61, 95% CI: 1.17, 11.18) than those without congenital deformity. Not only these but also the odds of death of neonates admitted due to low birth weight 2.13 times (AOR: 2.13, 95% CI: 1.23, 3.67) compared to normal birth weight. In addition to these, the odds of death due to RDS was 3.32 times (AOR: 3.32, 95% CI: 1.97, 5.59) compared to those admitted without RDS. Finally, the odds of death of neonates who got Ambu-bag resuscitation, antibiotics, glucose, and oxygen therapy were 84% (AOR: 0.16, 95% CI: 0.07, 0.38), 50% (AOR: 0.50, 95% CI: 0.27, 0.90), 53% (AOR: 0.47, 95% CI: 0.30, 0.72), and 74% (AOR: 0.26, 95% CI: 0.16,0.41) risk reduction compared to neonates who did not get the corresponding treatments respectively by keeping other factors constant for all interpretations (Table 4).
The bivariable and multi-variable logistic regression analysis of neonatal mortality among neonates admitted at the NICU of FHCSH, in Bahir Dar, Northwest Ethiopia, 2021 (n = 870).

1-Reference category.
Associated variables based on bivariable selection criteria.
Statistically significant variables at multivariable analysis with a 5% level of significance.
Discussion
In this study, NM was 218 per 1000 NICU-admitted neonates. This finding was higher as compared with a study in Amhara Referral Hospitals 186, 18 southern Ethiopia study 165, 22 Gondar University Hospital 173, 25 and Jimma University hospital 133 per 1000 live births. 26 These variations between studies could be due to differences in sample size, and follow-up periods.18,25 In this study, the average annual NMR trend was 2.1% per year in the NICU from 2016 to 2020. This finding was supported by Ethiopian mini EDHS 2019 and annual 2019/2020 reports from the NICU of FHCSH even though the rate was double in my study.17,20 This might be due to the weak monitoring system. 27
In this study, the odds of death of neonates from rural areas were 1.96 times (AOR: 1.96, 95% CI: 1.26, 3.06) higher than in urban. This finding was supported by studies at Nekemte Referral Hospital. 24 This might be due to the differences in healthcare-seeking behavior between urban and rural residents and the difference in average distance from the health setup. Place of delivery was a significant factor of NM. As a result, home deliveries were 3.73 times more likely to die than health institutions. This finding was supported by a study conducted by the University of Gondar. 28 This could be due to the absence of safe delivery practices and post-natal care at home. 29
In addition to this, the odds of congenital deformity-related death were 3.61 times (AOR: 3.61, 95% CI: 1.17, 11.18) higher compared to those without congenital deformity. This was supported by a study conducted in a global network study. 13 Again, the odds of death due to low birth weight were 2.13 times (AOR: 2.13, 95% CI: 1.23, 3.67) more than normal birth weight. This is supported by a study in eastern Ethiopia, 30 and a Global Network study in low-income countries. 13
Furthermore, the presence of respiratory distress syndrome and birth asphyxia were also important risk factors for NM. The odds of death of neonates who were admitted with the presence of respiratory distress and birth asphyxia were 3.32 and 7.73 times higher than neonates without respiratory distress syndrome and birth asphyxia respectively. These findings were supported by a study conducted in Eastern Ethiopia, 30 in the referral hospital of Debre Markos, 31 a Hospital of St.Luke at Wolisso, 32 a referral hospital at Dilchora Dire Dawa, 33 and a study in SSA. 34 Likewise, birth asphyxia was supported by a study conducted in Southern Ethiopia, 22 Eastern part of Ethiopia, and Northern parts of Ethiopia, in Tigray.30,35 In addition, this finding was also supported by a study in Bangladesh 36 and a study in developing countries. 1 This was strongly due to the difficulty of breathing.
Finally, the odds of death of neonates who got Ambu-bag resuscitation, taking antibiotics, glucose, and oxygen given were 84% (AOR: 0.16, 95% CI: 0.07, 0.38), 50% (AOR: 0.50, 95% CI: 0.27, 0.90), 53% (AOR: 0.47, 95% CI: 0.30, 0.72), and 74% (AOR: 0.26, 95% CI: 0.16, 0.41) risk reduction compared to neonates who did not get the above corresponding treatment modalities respectively by keeping other factors constant for all interpretations. The reason could be birth asphyxia is the leading cause of neonatal mortality. However, this medical state and other causes of neonatal mortality might be resolved with bag and mask resuscitation together with oxygen therapy, antibiotics, and glucose. This finding is supported by studies carried out by Shikuku, Hadgu, and WHO.37-39
Limitations and strengths of the study
The main strength of this study was to show the 5-year trends of NM by using the historical data from the period 2016 to 2020. Despite these strengths, this study did not address the impact of training on the reduction of neonatal mortality.
Conclusion and Recommendation
According to this 5-year trend analysis study, the average trend of NMR has risen from January 1, 2016, to December 31, 2020, indicating that more work is still needed to make progress toward meeting the SDG goal by 2030. Place of residence, having birth asphyxia, congenital deformity, low birth weight, RDS, Ambu-bag resuscitation, taking antibiotics, glucose, and oxygen therapy were found to be statistically significant factors of neonatal mortality. Therefore, all stakeholders shall give due attention to reducing this timely rising trend of neonatal mortality.
Footnotes
Acknowledgements
The authors would like to thank Bahir Dar University College of Medicine and Health Science for title approval. Again, we would like to acknowledge the staff members who worked in the hospital’s card room, NICU, and Amhara Public Health Institute for their support during the data collection time. Lastly, we extend our gratitude to the data collectors and a supervisor for their valuable contribution to making this study a reality.
Abbreviations
ANC: Antenatal Care; AOR: Adjusted Odds Ratio; CI: Confidence Interval; EDHS: Ethiopian Demographic Health Survey; ENM: Early Neonatal Mortality; FHCSH: Felege Hiwot Comprehensive Specialized Hospital; HBV: Hepatitis B Virus; HCV: Hepatitis C Virus; HIV: Human Immune Virus; KMC: Kangaroo Mother Care; LNM: Late Neonatal Mortality; MRN: Medical Registration Number; NICU: Neonatal Intensive Care Unit; NM: Neonatal Mortality; NMR: Neonatal Mortality Rate; RDS: Respiratory Distress Syndrome; SRSWOR: Simple Randomly Sampling Without Replacement; SDG: Sustainable Development Goals; SSA: Sub-Saharan Africa; VDRL: Venereal Diseases Research Laboratory; WHO: World Health Organization.