
Abstract
Objective
The objective of this study was to evaluate the effect of phenobarbital and phototherapy combination on the total serum bilirubin of the newborn infants with isoimmune hemolytic disease (IHD) and its impact on blood exchange transfusion rates.
Patients and Method
This single-blinded, prospective, randomized, controlled trial was conducted between March 2013 and December 2014 at the pediatric ward of two Military Hospitals in Jordan. A total of 200 full-term neonates with IHD were divided randomly into two groups: (1) the phenobarbital plus phototherapy group (n = 103), and (2) the phototherapy-only group (n = 97). Infants in group 1 received an oral dose of 2.5 mg/kg phenobarbital every 12 hours for 3 days in addition to phototherapy. The total serum bilirubin was observed.
Results
Of the total 200 included newborn infants, 186 infants completed the study: 97 infants were included in group 1 and 89 infants in group 2. The difference between the mean total serum bilirubin levels at 24, 48, and 72 hours after starting the trial was clinically and statistically significant at P < 0.05. The differences between the two groups were also statistically significant at P < 0.05. Of the total 186 who completed the study, only 22 underwent blood exchange transfusion [7 from group 1, and 15 from group 2 (P = 0.0478)].
Conclusion
In a limited-resources setting, phenobarbital in combination with phototherapy may be helpful to newborn infants with IHD, as it results in a faster decline in total serum bilirubin, thus decreasing the need for blood exchange transfusion than phototherapy alone.
Introduction
Hyperbilirubinemia is the most common medical problem requiring rehospitalization, evaluation, and management during the neonatal period.1–3 Isoimmune hemolytic disease (IHD) is the most common pathologic cause of unconjugated hyperbilirubinemia in the newborn. 4 Transient encephalopathy or acute bilirubin encephalopathy and its sequelae, kernicterus, are the most serious complications of unconjugated hyperbilirubinemia.1,4,5 Unless their levels are high enough, requiring an exchange transfusion, the current approved mainstay of treatment of indirect hyperbilirubinemia of the newborn is phototherapy.1,2,4,5 Exchange transfusion can lead to many serious complications such as thrombocytopenia, portal vein thrombosis, umbilical or portal vein perforation, necrotizing enterocolitis, arrhythmia, cardiac arrest, hypocalcemia, hypomagnesemia, hypoglycemia, respiratory and metabolic acidosis, and all other potential complications of blood transfusions.1,4,5 High-dose intravenous immunoglobulin (IVIG) has been shown to reduce total bilirubin and the need for exchange transfusion in neonates with Rh and ABO IHD.6–8 Phenobarbital administration to pregnant mothers and their offspring was shown to reduce by 50% the peak serum total bilirubin concentrations caused by physiologic jaundice. 4 The major effect of phenobarbital is to increase hepatic glucuronosyl transferase (UGT) activity and the conjugation of bilirubin, apart from possibly enhancing hepatic uptake of bilirubin. 4
Several studies have evaluated the effect of phenobarbital on nonpathologic, indirect hyperbilirubinemia.9–17 The objective of this study was to evaluate the effect of phenobarbital and phototherapy combination on the total serum bilirubin level of newborns with IHD and its impact on the blood exchange transfusion rate.
Patients and Method
This single-blinded, prospective, randomized, controlled trial, which was approved by the Jordanian Royal Medical Services Ethical Committee, was conducted between March 2013 and December 2014, at the level III neonatal intensive care unit and pediatric ward at Prince Hashem Military Hospital, Zarqa, Jordan, and Queen Alia Military Hospital, Amman, Jordan. Parents or guardians of all enrolled infants gave their written, informed consent for participation in the study, which was conducted in accordance with the principles of the Declaration of Helsinki. A total of 200 full-term jaundiced neonates with ABO incompatibility, Rh incompatibility, or both were divided randomly using the odd and equal numbers of the admission sequence into two groups: the phenobarbital plus phototherapy treated group (n = 100), and the phototherapy-alone group (n = 100). Infants in the phenobarbital plus phototherapy group received an oral dose of 2.5 mg/kg phenobarbital every 12 hours for 3 days (this was dispensed in linctus simplex in a concentration of 1 mg/mL) in addition to phototherapy, while the neonates in the phototherapy-only group received phototherapy with the same amount of the linctus simplex but without phenobarbital. Crossover was not allowed between groups.
The sample size was calculated based on 95% confidence interval, absolute accuracy of 0.1, and sensitivity of 80%.
All enrolled infants met the following criteria: full term, less than 8 days of life, birth weight between 2.5 and 4.0 kg, ABO or Rh incompatibility or both, total serum bilirubin ≤20 mg/dL, direct bilirubin <1.5 mg/dL, PCV ≥ 35%, on breast milk, negative C-reactive protein (CRP) on admission, no dysmorphic features or congenital abnormalities, no signs or symptoms of neonatal sepsis requiring the administration of antibiotics, and no other medical conditions.
Exclusion criteria included the following: parents’ wish to stop the study or if the baby was discharged against medical advice; the newborn infant showing increase in the liver enzymes, apnea, or respiratory arrest; hypotension, feeding intolerance, hypoactivity, or irritability; or positive blood culture after 48 hours of admission.
The primary outcomes of the study were to evaluate the effect of phenobarbital on total serum bilirubin of newborns “with IHD and its impact on the blood exchange transfusion rate. Two methods were used to test the effectiveness of phenobarbital: (1) the total serum bilirubin in both groups, and (2) the number of infants needed blood exchange transfusion in each group.
The effects of subtypes of IHD, sex, and positive direct Coombs test (DCT) on the response to the treatment and the effect of treatment on rebound hyperbilirubinemia were studied as secondary outcomes.
Total serum bilirubin, direct bilirubin, alkaline phosphatase (ALP), alanine transaminase (ALT), aspartate amino-transferase (AST), and PCV were measured at the beginning and at 6, 12, 24, 48, 72 hours after the initiation of treatment, and 24 hours after the treatment was stopped.
The decision to start phototherapy and phenobarbital was made on the basis of the age of the baby in hours and serum total bilirubin (STB) levels, as per the American Academy of Pediatrics guidelines for phototherapy.
Phototherapy was stopped when the STB level fell to 2 mg/dL or below the level at which phototherapy would be indicated for that age. Significant bilirubin rebound (SBR) was defined as post-phototherapy bilirubin level needing reinstitution of phototherapy.
Conventional standard-irradiance-level Fluoro-lite phototherapy units (A Drager and Siemens Company) were used for all included infants.
The phenobarbital dose was double-checked by a neonatologist and a registered nurse before it was given to the babies. All blood samples were drawn by a registered nurse and sent to the local laboratory at Prince Hashem Military Hospital and Queen Alia Military Hospital. All enrolled infants were attended to and examined on a daily basis by the neonatologist.
Blood exchange transfusion was done based on the total serum bilirubin, as per American Academy of Pediatrics guidelines for blood exchange in hospitalized infants.
The newborn with IHD was the unit of analysis in this study. A descriptive statistical study was carried out on the measured variables. Some data collected in this prospective study were parametric and others nonparametric. The t-test, odds ratio (OR), and two-sided 95% confidence intervals (95% CIs) were used when dealing with proportions. CI calculations were used to analyze the results. The level of significance was set at P < 0.05.
Results
There were no differences in the characteristics of the included newborn infants of the two groups (Table 1). Of the total 200 included newborns, 186 (97 in the phenobarbital and phototherapy group and 89 in the phototherapy-only group) completed the study. Of those who did not complete the study, eight got discharged against medical advice (five of them from the phenobarbital and phototherapy group, and three from the phototherapy-only group), two infants from the phototherapy-only group showed positive blood cultures after 48 hours, one infant from the phenobarbital and phototherapy group developed hypotension, two infants had feeding intolerance, also from phenobarbital and phototherapy group, and one infant from phototherapy-only group developed hypoactivity.
Characteristics of included newborn infants.
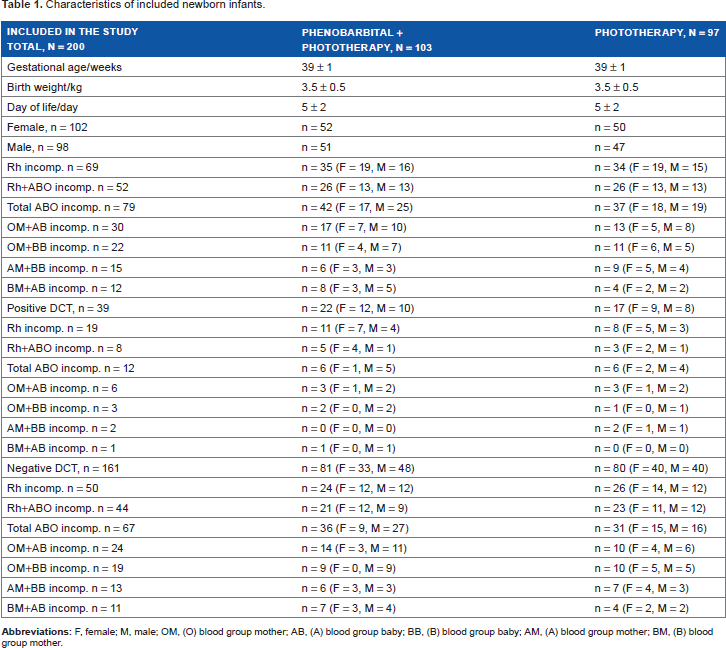
Table 2 and Figure. 1 show the mean total serum bilirubin levels in the two groups on 0, 6, 12, 24, 48, 72, and 96 hours of the trial and compare the difference between the initial and the final bilirubin levels in the two groups. The difference between the mean total serum bilirubin levels at 24, 48, and 72 hours after starting the trial is clinically and statistically significant at P < 0.05. The differences between the two groups are also statistically significant at P < 0.05.

Effect of phenobarbital and phototherapy versus phototherapy only on TSB.
Mean total serum bilirubin on hours of study, and differences between means for initial and final hours in both groups.

P < 0.05.
Mean direct bilirubin in those who were treated with phenobarbital and phototherapy reached 0.4 ± 0.2 mg/dL after 24 hours of treatment initiation, and the level went back to the initial value of 0.5 ± 0.2 mg/dL after 24 hours of stopping treatment, while those treated with phototherapy-only maintained the same level of direct bilirubin during the observational time, as shown in Figure. 2.

Effect of phenobarbital and phototherapy versus phototherapy only on direct bilirubin.
In both groups, there was no change with time in the mean ALP (170 ± 5 mg/dL), ALT (20 ± 5 mg/dL), and AST (35 ± 5 mg/dL), and there was no difference in the effect of the two types of treatment on the PCV (35% ± 5%).
Regarding the prevalence of exchange transfusion, the difference was clinically and statistically significant between the two groups, as shown in Table 3.
Comparison of the effect of different factors on the risk of exchange transfusion in patients with isoimmune hemolytic disease of the newborn.

There were no clinically or statistically significant differences in the risk for exchange transfusion between male and female infants with hyperbilirubinemia due to isoimmunization of both groups (OR = 1.1667; 95% CI = 0.1913–7.1167; P = 0.8673).
The risk of exchange transfusion in patients with positive DCT was clinically and statistically significant in comparison with patients with negative DCT. Meanwhile, there was no significant difference between the phototherapy-only and phenobarbital plus phototherapy groups on the need for exchange transfusion in those with positive DCT, as shown in Table 3.
Comparing the effect of both types of treatment on the prevalence of exchange transfusion in patients with Rh incompatibility, it was found to be neither clinically nor statistically significant, while in patients with ABO incompatibility it was found to be clinically but not statistically significant. The same comparison between patients with both Rh and ABO incompatibility showed that it was clinically and statistically very significant (Table 3).
On studying the effect of both types of treatment on the prevalence of exchange transfusion in patients with different types of ABO incompatibility, of the 12 patients with ABO incompatibility who underwent blood exchange, 5 (41.6%) were with OM+AB incompatibility, 3 (25.0%) were with OM+BB incompatibility; 3 (25.0%) were with AM+BB incompatibility, and only 1 (8.3%) with BM+AB incompatibility. There was less prevalence of exchange transfusion in patients who were included in the phenobarbital and phototherapy group except those with OM+BB incompatibility.
In general, 25.8% of the infants with IHD developed rebound hyperbilirubinemia. The rebound of bilirubin was clinically and statistically less prevalent when phenobarbital was administered in combination with phototherapy (Table 4).
Effect of phenobarbital on positive rebound of bilirubin in all patients with hyperbilirubinemia due to isoimmunization.

Discussion
This study was designed to evaluate the effect of phenobarbital and phototherapy combination on the total serum bilirubin of the newborn infants with the IHD and its impact on blood exchange transfusion rates, to help both newborn infants with IHD (who are at the risk of either blood exchange transfusion and its complications or kernicterus) as well as healthcare providers with limited resources, with no facility for intensive phototherapy and expensive IVIG.
Several studies on the effect of phenobarbital on the hyperbilirubinemia of non-hemolytic disease of newborn infants have been conducted, which have shown that phenobarbital decreases the rate of blood exchange transfusion9,11–13,16–21; on the other hand, some studies have reported that phenobarbital has no effect on the TSB level in newborns with nonhemolytic disease and thus has no effect on the rate of blood exchange transfusion.22,23
There are several studies that evaluated the effect of phenobarbital prophylaxis given either to the mother of suspected ABO or Rh incompatibility fetus just before delivery, or to the newborn immediately after birth.13–15,24–28
The originality of this study is that it is, to the best of our knowledge, the first study to evaluate the effect of phenobarbital and phototherapy combination on the established hyperbilirubinemia of IHD of newborns.
In this study, we compared the effect of a combined therapy with a monotherapy, but we did not have controls, as it was considered unethical to put the included controls in the risk of complications of high levels of bilirubin. Here we would like to mention that Wong et al. 21 , while comparing the relative roles of phototherapy and phenobarbitone in the treatment of non-hemolytic neonatal jaundice, also did not consider it ethical to have controls.
Those newborns who required antibiotics were excluded in our study, as it is a well known fact that some antibiotics can displace bilirubin from bonding to albumin, causing increases in the TSB, and thus can affect the results of the study.
Wong et al, based on on the findings of Waltman et al. 29 , explained the decrease in TSB in the phenobarbital groups in different studies by administering phenobarbitone in an elixir of linctus simplex that contained 36% ethanol, which is as an enzyme inducer as phenobarbital. In our study, both groups were given the same amount of linctus simplex to exclude its effect on the results as previously done by Levin et al. 22 Our study showed that the use of phenobarbital in combination with phototherapy compared to phototherapy alone in established hyperbilirubinemia of IHD of the newborn caused a rapid decrease in the total serum bilirubin, which was associated statistically and clinically with a significant decrease in blood exchange transfusion rate. However, two important studies by Wong et al. 21 and Nazer et al. 30 , which compared the effect of combination therapy with the effect of montherapy on TSB, contradict our findings. This difference could be explained by the fact that both earlier studies were conducted on small numbers of patients with non-hemolytic hyperbilirubinemia. Moreover, Nazer et al studied the effect of both types of therapy in patients with congenital enzyme deficiency (Crigler–Najjar syndrome type I), where one would not expect to observe any effect from the combination of the enzyme inducer (phenobarbitone) and phototherapy. Another factor that could have affected the results of Wong's et al's study was that they underestimated sepsis and they had two deaths due to neonatal septicemia, whereas in our study patients with positive CRP and/or with any sign of sepsis requiring the use of antibiotics were excluded, as sepsis is a well-known cause of exaggerated hyperbilirubinemia. The possibility of variable dose, absorption, or vomiting of oral medication cannot also be excluded.
In general, data from our study indicate that sex has no effect on the rate of exchange transfusion, comparing both groups. It also shows that newborn infants with ABO incompatibility, in general, are subject to more exchange transfusion, while those with the ABO+Rh incompatibility undergo less exchange transfusions.
The impact of DCT on the rate of exchange transfusion has not been discussed in any similar study before, but in our study and, in general, in both negative and positive DCT newborn infants with hemolytic disease of the newborn the rate of exchange transfusion is higher in those who are treated with phototherapy alone, and the risk of patients with positive DCT to undergo exchange transfusion is very high in comparison to those with negative DCT. But at the same time, there is no significant difference between phototherapy-only versus phenobarbital and phototherapy on the need for exchange transfusion in patients with positive DCT.
Another finding that was not mentioned earlier but noted in our study is that the newborns treated with phenobarbital in combination with phototherapy developed significantly less rebound of bilirubin than those who were treated with phototherapy alone.
Our study, unlike Wong et al's, showed the effect of not only phenobarbital and phototherapy on the mean total serum bilirubin but also other liver enzymes (ALP, ALT, and AST).
Finally, this study showed that phenobarbital is a safe drug at least in the same amount and duration that was used in this study, as data from our study showed that only three newborn infants from the phenobarbital and phototherapy group were excluded due to possible side effects of phenobarbital (hypotension and feeding intolerance).
The single limitation of the study is that it was not designed to evaluate any long-term side effects of phenobarbital.
Conclusion
In limited-resource settings, phenobarbital in combination with phototherapy may help newborn infants with IHD, as it results in a faster decline in total serum bilirubin, and thus may decrease the need for blood exchange transfusion than phototherapy alone. Further studies are needed to evaluate any adverse effects and neurodevelopmental outcome of this therapeutic strategy.
Author Contributions
Conceptualized the study: GS. Designed the study: GS. Wrote and edited the manuscript: GS, MK. Collected the data: IA, AA. Analyzed the data: RH, AS. Checked the references: GS. Made critical revisions: GS, RH. All authors reviewed and approved the final manuscript.
Footnotes
Acknowledgment
The authors thank Dr. Shakkoury Ghassan, Professor of Pediatrics, Jordanian Ministry of Health, for help in conducting the statistical analysis and editing this paper.