
Abstract
Background:
Neonatal hyperbilirubinemia is a widespread and significant clinical problem among neonates worldwide. Globally, every year about 1.1 million babies develop it and the vast majority reside in South Asia and sub-Saharan Africa. Studies on the magnitude and factors associated with neonatal hyperbilirubinemia are limited in Ethiopia. So this study was aimed at assessing the prevalence and associated factors of neonatal hyperbilirubinemia among hospitalized neonates in the neonatal intensive care unit of Jimma Medical Center (JMC), Jimma, South West Ethiopia.
Design:
Hospital-based cross-sectional study was conducted at JMC from July 24 to October 19, 2020.
Methods:
A total of 222 neonates with their mothers were included and conveniently selected. Data was collected by interviewing mothers through structured questionnaires and reviewing neonates’ medical records using a checklist. Multivariable binary logistic regression analyses were employed to identify factors associated with neonatal hyperbilirubinemia.
Results:
from a total of neo-maternal pairs included in the studies; the proportion of Neonatal hyperbilirubinemia was found to be 94 (42.3%). Neo-maternal ABO incompatibility 33 (35.1%), prematurity 41 (43.6%), sepsis 35 (37.2%), Neonatal birth asphyxia 20 (21.2%), and Rh isoimmunization 10 (10.6%) was significantly associated with neonatal hyperbilirubinemia.
Conclusion:
The prevalence of neonatal hyperbilirubinemia in the study setting was high. Antenatal care (including both mother and fetus detail examination and follow-ups) as well as cautions during labor need to focus on since Neonatal hyperbilirubinemia-associated factors were maternal and neonatal. Hence, further assessment, early intervention, and timely treatment are important to mitigate the burdens in neonates due to hyperbilirubinemia.
Introduction
Hyperbilirubinemia is a condition in which excess bilirubin is in the blood. Bilirubin is a non-polar endogenous by-product of heme catabolism with 85% from normal senescent erythrocyte broken down and 15% from ineffective erythropoiesis or turnover of non-hemoglobin hem proteins. 1 In newborns, hyperbilirubinemia becomes clinically apparent as jaundice when total serum bilirubin concentration gets ⩾5 mg/dL in contrast to adults at ⩾2 mg/dL. Accumulation of bilirubin in the skin and mucous membrane causes yellow discoloration of the skin and sclera of the eye and causes cephalocaudally in advancements. 2
Excessive bilirubin induces acute and chronic bilirubin encephalopathy. Acute bilirubin encephalopathy involves clinical presentation of lethargy, hypotonia, poor suck, high-pitched cry, fever, and irritability. Chronic bilirubin encephalopathy (kernicterus) is a severe irreversible and devastating clinical tetrad consisting of movement disorders, auditory dysfunction, oculomotor impairments, and dental enamel hypoplasia 3 where different risk factors cause and potentiate the passage of bilirubin into the brain of neonates and hence increase the risk of neurotoxicity. 4
Neonatal hyperbilirubinemia is a ubiquitous health problem that occurs in 60% of full-term and 80% of preterm neonates. 5 It is still the most common cause of re-hospitalization of the newborn in the first week of life6,7 that imposes many negative effects on both neonates and their families.8,9
Moreover, neonatal hyperbilirubinemia is common and inflicts significant burdens of mortality and morbidly globally. However, the incidence and burdens were unacceptably high in low-income and middle-income countries (LMICs).10-12 There is a multiplicity of risk factors associated with maternal, prenatal, and neonatal factors related to the occurrence of neonatal hyperbilirubinemia that can be modifiable and manageable.13-17 In Nigeria, neonatal sepsis, prematurity, and G-6PD deficiency are factors significantly associated with neonatal hyperbilirubinemia 17 while in Rwanda, birth weight, gestational age, neonatal gender, method of delivery, blood group incompatibility, infections, cesarean section, and prematurity are significantly associated with neonatal hyperbilirubinemia. 18
Neonatal mortality is alarmingly high 19 and hyperbilirubinemia was among the causes of neonatal admission and death in Ethiopia.20-22 Identification of predisposing factors and initiation of appropriate management is paramount in the preventions of hyperbilirubinemia complications. However, there are very little data available on the prevalence of neonatal hyperbilirubinemia and associated factors in Ethiopia particularly in Jimma medical center, as to the knowledge of the principal investigators no study conducted yet on the topic regardless of the burdens of the problems. Therefore, the present study aimed at determining the magnitude of hyperbilirubinemia and associated factors among neonates admitted to neonatal ICU in the study area.
Materials and Methods
Study area, design, and period
A hospital-based cross-sectional study design was used, from July 24 to October 19, 2020, at the Neonatal ICU of Jimma Medical Center (JMC). The hospital (JMC) is located in Jimma city, 352 km southwest of the capital Addis Ababa. Jimma Medical Center is one of the oldest public hospitals in the country, which is established in 1930 E.C by Italian invaders. It has 800 beds with teaching and referral services in the Southwestern part of the country, for approximately 15 000 inpatients, 160 000 outpatient attendants, 11 000 emergency cases, and 4500 deliveries annually coming to the hospital from the catchment population. The neonatal ICU is one of the ICU services that the hospital is currently running. It has 20 neonatal beds and 14 Kangaroo mother care (KMC) beds. The unit also has 3 incubators, 22 radiant warmers, and 3 continuous positive airway pressure (CPAP), 4phototherapy and oxygen concentrator machines. Additionally, there is pulse oximetry, glucometer, and neonatal resuscitation equipment. Advanced procedures such as exchange transfusions and Lumber punctures are performed at the center. The unit is staffed with pediatricians, pediatric residents, and neonatal nurses and is located adjacent to the labor ward to receive high-risk newborns from this unit. Furthermore, the unit also receives neonates referred from other health facilities and homes.
Participant’s selection and exclusion
All neonates aged less than 28 days admitted to Neonatal ICU during the study period and mothers age 18 years and above with informed consent were included in the study. Whereas mothers were unable to give informed consent and unwillingness to participate, neonates with anomalies/malformations and less than 35 gestational age were excluded from the study.
Sample size determination and sampling techniques
The sample size was calculated using the single proportion formula by the following assumption, Proportion of neonatal hyperbilirubinemia is 37. 3%, confidence interval (95%), and a 5% margin of sampling error were tolerated. This gives a total sample size of 359 neonates, but since the estimated study population was less than 10 000. Thus correction formula was used and finally, 222 samples of neonates admitted were included.
The convenient sampling technique was used and the study subjects were consecutively recruited until the required minimum sample size of the study was fulfilled.
Data quality assurance
All quality assurance components were applied in course of these studies. To increase the reliability of data, 2 data collectors were assigned by team leaders of neonatal nurses based on their previous experience in data collection and language skills. Besides training on the data collection procedures was given to the data collector. The instrument used for collections of socio-demographic data was adopted from previous studies of related topics and validated standards like Ethiopian demographic health survey checklists. The study participants were fully informed about the aims of the study, assured about information obtained from them was only for research purposes, and information obtained was anonymized and coded. For laboratory data collection standard operating procedures were strictly followed and implemented before specimen collection up to recording and interpreting of the laboratory results both by those who collect the specimen in the ward and who processing in the lab. Hemolysis-free specimen, protected from light exposure/photo oxidations/and extreme colds of icebox was collected by neonatal nurses. The collected sample was taken from the Neonatal ICU ward and processed in the laboratory. All specimens were collected before administrations of phototherapy for neonates with signs and symptoms of hyperbilirubinemia. Then label the sample and the questionnaire paper with the same identification number to avoid any mix-ups or errors. The expired date of the reagent was checked before the analysis of samples. A blood sample of study subjects used for bilirubin determination was run with both internal quality control materials and manufacture-provided standards/controls. Post analytical data quality check was done by different statistical software through the double entry of data to prevent errors from occurring and the interpretation of results was according to the aims of the studies. The completeness of data was checked and supervised by the principal investigator on daily basis during the entire data collection period.
Data processing and analysis
All the data were cleaned, coded, and entered into Epi data version 3.1 and transferred to SPSS version 23.0 for analysis. Descriptive statistics like frequency, proportions, and percentage were used to summarize the study variable.
Bivariate and multivariate logistic regression models were used to assess how well predictor independent variables explain or predict dependent variables and control possible confounders and identify the determinant factors associated with the prevalence of neonatal hyperbilirubinemia. P-value < .05 was considered statistically significant.
Data collection techniques
An interview-administered structured questionnaire was used to collect socio-demographic and clinical data of mothers and medical records of study subjects were also reviewed by using standard checklists.
About 2 mL of venous blood was collected by experienced neonatal nurses. Then the blood samples were centrifuged for 5 minutes at 4000 revolutions per minute (rpm) to separate serum from other contents of whole blood. The extracted serum was kept in Nunc tube under −200°C deep freeze until laboratory analysis for bilirubin. Later, these frozen sera were analyzed for serum total bilirubin and direct bilirubin by HumaStar 100, a chemistry analyzer (HUMAN Diagnostics, Wiesbaden Germany) fully automated auto analyzer by the direct endpoint enzymatic method. ABO/RH blood grouping of the study subject was determined by direct slide methods from a whole blood specimen.
Results
Socio-demographic and other characteristics of study subjects
In this study, a total of 222 neonates with their mothers were included and made a 100% response rate.
The median age of the study mothers was 26.34 years and more than three-fourths of them were between 20 and 35 years. About 122 (55.0%) mothers were living in rural areas. Of the total interviewed mothers, 159 (71.6%) were housewives. Regarding educational status, 11.7% were unable to read and write, 32.7% primary education, 35.4% secondary education, and 19.7% for higher education were documented study participants. Their previous delivery history revealed that 40 (18.0%) mothers were either history of abortion, stillbirth, neonatal death, or have a history of premature birth “Table 1.”
Socio-demographic characteristics of mothers of neonates at neonatal ICU.

Neonate clinical characteristics
One hundred thirty-eight (62.2%) neonates were male in sex and 42.3% of neonates’ age on admission lies within early neonatal age. Moreover, about 146 (65.8%) neonates were delivered in full-term with a birth weight of 2.5 kg and above were 166 (74.8%). In this study, an Apgar score of 101 (45.5%) for neonates at 1 and 5 minute were recorded. Regarding the feeding status, 175 (78.8%) neonates fed breast milk exclusively and 116 (52.3%) feeding breast started within 1 hour of delivery. In this study, the blood group of neonates was assessed and blood groups “O,” “A” “B,” and “AB” were 102, 63, 46, and 11 respectively. Two hundred twelve (95.5%) of study neonates were rhesus positive. Birth complications were recorded in 10.3% of study subjects. Regarding danger signs and symptoms of neonates, 187 (84.2%) were admitted with one or more danger signs to NICU. Among study neonates, 24 (10.8%) had prolonged durations of defecations or meconium excretions. One hundred eighty (81.1%) admitted neonates administered one or combinations of antibiotic medication “Table 2.”
Neonatal characteristics among neonates admitted to neonatal ICU.

Maternal clinical characteristics
Regarding antenatal care (ANC) follow-up, 216 (97.3%) respondents had at least one follow-up during their pregnancy. Two hundred and thirteen (95.9%) neonates were delivered at health institutions. Home delivery was reported by 9 (4.1%) mothers. Concerning the mode of delivery, spontaneous vaginal delivery accounted for 146 (65.8%) whereas cesarean section 76 (34.2%) mothers. The normal duration of labor was recorded by 159 (71.6%) participants. Oxytocin was used as induction or augmentation of labor by 63 (16.6%) mothers. In this study, 33 (14.9%) delivery of mothers were in breech or non-cephalic presentations. Gestational diabetes mellitus by 6 (2.7%), hypertension by 20 (9.0%), the premature rupture of membrane (PROM) by 23 (10.4%), meconium aspirated syndrome (MAS) 42 (18.9%), and anemia by 7 (3.2%) mothers are identified as a complication during pregnancy. ABO blood group of mothers was assessed and recorded as “O,” “A” “B,” and “AB” by 134, 46, 36, and 6, 60.4%, 20.7%, 16.2%, 2.7% respectively. Similarly, 5.4% of study participant mothers were rhesus negative. Previous treatment for RH immunizations was recorded only in 2 study participant mothers. None of the studies subject mothers have received blood and blood products during their pregnancy or previously. About parity and gravida of mothers, 81 (36.5%) and 141 (63.5%) were prim parity and multiparty respectively. Eighty-five (60.3%) of studies mothers had inter-pregnancy intervals of less than 2 years “Table 3.”
Maternal clinical characteristics of the admitted neonates to neonatal ICU.

Variables were screened by binary logistic regression analysis: Sex of neonate, age of neonates, exclusive breastfeeding, induction of labor, neonatal birth asphyxia, sepsis, ABO blood incompatibility, Rh incompatibility, prolonged defecations of meconium, ampicillin treatment, leukocytosis, thrombocytopenia, prematurity hypoglycemia, and others in neonates had a significant association with neonatal hyperbilirubinemia at P-value ⩽ .25 “Table 4.”
Bivariate logistic regression analysis of different factors with neonatal hyperbilirubinemia among neonates admitted to neonatal ICU.

Abbreviations: 1, reference; COR, crude odds ratio; CI, confidence interval.
P-value < .25. **P-value < .05.
Multivariable binary logistic regression analysis was done by taking variables showing significant association on bivariate analysis at a P-value of ⩽.25 to control (adjust) the possible confounding. Sex of neonate, age of neonates, exclusive breastfeeding, induction of labor, neonatal birth asphyxia, sepsis, ABO blood incompatibility, RH incompatibility, and prolonged defecations of meconium, Leukocytosis, Thrombocytopenia, and Prematurity had a significant association with neonatal hyperbilirubinemia at P-value < .05 of multivariate analysis “Table 5.”
Multivariate logistic regression analysis of different factors with neonatal hyperbilirubinemia among neonates admitted to neonatal ICU.
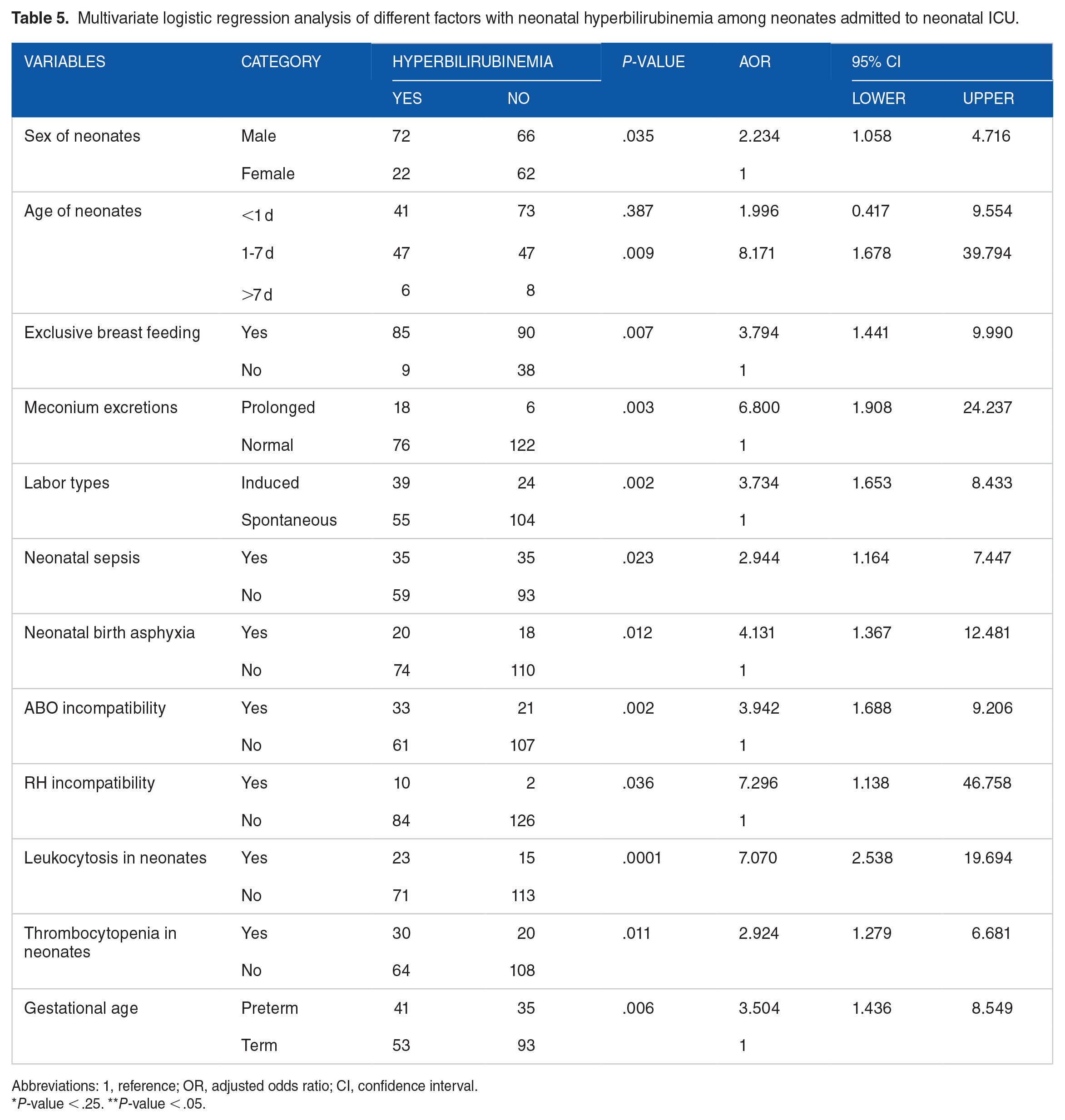
Abbreviations: 1, reference; OR, adjusted odds ratio; CI, confidence interval.
P-value < .25. **P-value < .05.
Discussion
Neonatal hyperbilirubinemia incorporates vital importance on baby morbidity and hospitalizations worldwide wherever the overwhelming majority of the affected neonates reside in sub-Saharan Africa and South Asia. 11 During this study prevalence of neonatal hyperbilirubinemia was 94 (42.3%) which was a lower finding than reported in Malaysia (63%) 23 and South Africa (55.2%). 24 However, it absolutely was beyond a finding from Pakistan (27.6%), 10 Benin (26.5%), 17 and Ghana (32.9%). 24 It was also quite higher as compared to finding from Nepal, 17 Indonesia (4.08%), 25 Iran (12.6%), 26 Congo Brazzaville (7.2%), 27 and Uganda (22.7%). 28 Southeast Nigeria (35%), 29 Rwanda (44.3%), 18 and Black lion Ethiopia. 30 This disparity could be due to sampling size, study period difference, study design, study area, methodology difference, coverage of obstetrics care, definitions of hyperbilirubinemia, and characteristics of the study participant. This study revealed that male neonates had higher odds of developing neonatal jaundice [AOR = 2.234; 95% CI (1.058-4.716)] compared to their female counterparts. The finding was corroborated by studies done in Nepal, 31 and Nigeria. 32 Conversely, this result was concordant with findings in Croatia, 25 and Iran. 26 Furthermore, this could be due to that male newborns have comparatively low levels of ligand which may not be able to process all the bilirubin formed from red blood cells and due to hormonal effects of transporter protein where testosterone down regulates membrane transporter protein which is involved in bilirubin metabolism.
The most affected age group by neonatal hyperbilirubinemia in this study was those neonates in early neonatal periods (1-7 days) at admission which was 50% and those >7 days old were 6.4%. Other studies in black lion hospitals showed that 52.5% of hyperbilirubinemia neonates were 3 to 6 days old at admission and those >6 days old were 32.5%. 11 This showed that as the age of the neonate increases the prevalence of neonatal hyperbilirubinemia decreases; the prevalence of neonatal hyperbilirubinemia is inversely proportional to the age of the neonate.
ABO incompatibility and hyperbilirubinemia were significantly associated in our study (AOR 3.942, CI 1.688-9.206). The number of ABO incompatibility in our study was 54% and 61.2% of them represent 35.10% of the total hyperbilirubinemia infants who developed HB in our study. This finding was consistent with other studies conducted in Northern India, 14 Nepal, 15 and Ethiopia. 22 This finding suggests the possibility of ABO-associated hemolysis as one of the causes of NHB in our study population.
Rh isoimmunization is the most significant cause of hemolytic hyperbilirubinemia in newborn babies. In our study, 12 mother-infant pairs had Rh discordance; 10 participants developed significant hyperbilirubinemia whereas the odds of developing hyperbilirubinemia were significantly high (AOR = 7.296, CI 1.138-46.758). Intravenous immunoglobulin is being used for the treatment of jaundice in newborn infants with hemolytic anemia. This finding was higher than the works of Eleje et al in Nigeria (21.3% of Rh discordant develops Neonatal hyperbilirubinemia) compared to 83.3% in our finding. 33 This disparity can be explained by the administration of anti-D immunoglobulin (33 (46.5%) of these received anti-D prophylaxes) compared to 2 (16.66%) in our findings that demonstrated the relevance of antenatal screening and prevention measures.
In addition, the study discovered that neonatal hyperbilirubinemia had a significant association with sepsis. The odds of neonatal hyperbilirubinemia among neonates who had sepsis were 2.9 times higher compared with those neonates who had no sepsis diagnosis [AOR = 2.944; 95% CI (1.164-7.447)]. Sepsis was also identified as the possible cause of neonatal jaundice in studies conducted in India,14,31 Ghana, 34 and Ethiopia. 22 This similarity in finding might be due to similarities in the study setting that is, intensive care unit (sepsis was a common finding in any hospital admissions and need intensive care). Sepsis could be due to poor hygienic environment, poor obstetric and nursery care, and sepsis would also possibly cause hemolysis of red blood cells and hepatic dysfunction that leads to cholestasis from septic states that leads to accumulation of serum bilirubin within the body, and conjointly arise from varied drugs used for sepsis treatment.
Birth asphyxia was also an important determinant of Neonatal hyperbilirubinemia [AOR = 4.131; 95% CI (1.367-12.481)]. Different studies conducted in Southern Nigeria, 33 and Northern Ethiopia 35 supported that neonatal jaundice is influenced by birth asphyxia. This similarity in finding was because perinatal asphyxia remains a common problem in the neonatal nursery and is a significant coincidence with neonatal hyperbilirubinemia in neonatal intensive care and it was also an insult to the newborn due to lack of oxygen, lack of perfusion to various organs which ends up in multi-organ system dysfunction due to hypoxic damage principally on brain, lung, liver and intraventricular hemorrhage that affect bilirubin conjugation ability of the liver that leads to jaundice. 35 Also, perinatal asphyxia with the hypoxic-ischemic neurological disorder will disrupt the blood-brain barrier, thereby permitting free entry of the unconjugated bilirubin to the neurons leading to a neurological disorder. Besides, kidney damage perinatal asphyxia also causes less excretion of the conjugated bilirubin, thereby inflicting conjugated hyperbilirubinemia and jaundice.
In this study induction of labor with oxytocin had a significant effect on the development of hyperbilirubinemia in neonates [AOR = 3.734; 95% CI (1.653-8.433)]. Our study was consistent with the studies of Peter et al, 16 Islam et al, 35 and Garosi et al. 36 However, the finding was discordant with the study of Kavehmanesh et al 26 and studies conducted in Poland. 37 Since Oxytocin causes osmotic swelling of erythrocytes leading to decreased deformability and hence more rapid destruction with resultant hyperbilirubinemia in the neonate. Neonatal hyperbilirubinemia had a significant association with the feeding mode of neonates particularly with exclusive breastfeeding [AOR = 3.794; 95% CI (1.441-9.990)]. The association was described in studies conducted by Seyedi et al 38 and Eleje 32 This is due to decreased caloric intake/starvation, inhibition of hepatic excretion of bilirubin and an increase in intestinal absorption of bilirubin (enterohepatic circulation) 39 and a component of breast milk 40 are suggested mechanisms for the hyperbilirubinemia associated with breast-feeding.
Inadequate enteral feeding favors increased entero-hepatic circulation and delays defecations of meconium and in our study participants 47.8% of had prolonged initiation of breastfeeding after birth. Consequently, participants who had prolonged initiation of breastfeeding after birth were more likely to develop HB and have delayed patterns of defecations. 31 Similarly, the odds of developing neonatal hyperbilirubinemia among neonates who had prolonged type defecations of meconium were 6.8 times higher compared with normal one [AOR = 6.800; 95% CI (1.908-24.237)]. It was similar to the finding of Seyedi et al. 38 However, it was inconsistent with the study conducted in Turkey 41 and Brazil. 42 The disparity could be due to characteristics’ of studies subjects that is, 34% of our study neonates were preterm in gestation and prematurity is associated with prolonged Passage of meconium when compared to term infants. 43 This is because 1 g of wet meconium contains an equal amount of milligram of bilirubin, delayed passage of meconium, and decreased frequency of meconium passage may increase enterohepatic circulation and contribute to the development of jaundice in neonates.
Thirty- four percent of our study neonates were preterm in gestation which was consistent with available studies. 33 Neonates born preterm had higher chances of developing hyperbilirubinemia than neonates born at term [AOR = 3.504; 95% CI (1.436-8.549)]. Prematurity was also identified as the possible cause of neonatal hyperbilirubinemia in studies conducted in India, 44 Iran, 43 and Ethiopia. 11 This more common in preterm infants was due to the relative immaturity of the red blood cells, hepatic cells, and gastrointestinal tract than in neonates born at term.
Hematological abnormality is one of the commonest problems encountered in the neonatal intensive care unit (NICU). Of this thrombocytopenia and leukocytosis is prevalent, associated with, and commonly follow hyperbilirubinemia due to bacterial infections. 45 Neonatal hyperbilirubinemia had significant association with both thrombocytopenia [AOR = 2.924; 95% CI (1.279-6.681)] and leukocytosis [AOR = 7.070; 95% CI (2.538-19.694)] in our studies respectively. Most of the available works of literature associate thrombocytopenia with complications of phototherapy in hyperbilirubinemia neonates 46 ; however thrombocytopenia due to hereditary thrombotic thrombocytopenic purpura (TTP) caused by ADAMTS13 mutations is a rare but serious condition, often presenting during the newborn period with microangiopathic hemolytic anemia could be a risk factor for neonatal hyperbilirubinemia. 47
Study limitation
The study design has some limitations in particular the generalizability of findings will be limited to infants admitted to the NICU. Since the present study evaluated only hospitalized newborns and the status of outpatient infants is not known. The studies also could not do blood film and G6PD assay to comment on and confirm infection and hemolysis.
Conclusions and Recommendation
Our study indicated the high prevalence of hyperbilirubinemia among neonates admitted to NICU. Gender, Neo-maternal ABO incompatibility, Sepsis, Neonatal birth asphyxia prematurity, and induction of labor with oxytocin were the risk factors associated with the prevalence of hyperbilirubinemia in neonates. Therefore, it is mandatory to screen, treat, and manage hyperbilirubinemia and its associated risk factors in neonates admitted to NICU.
Footnotes
Acknowledgements
We would also like to thank data collectors, study participants, and supervisors as well as those who directly or indirectly contributed to this study.
CORRECTION (August 2023):
There was a typo in the last author's name. Now, the typo has been corrected in the article.