
Abstract
Hemangiomas are the most common primary hepatic tumors, but there are few reports of their occurrence elsewhere in the abdomen. The concurrent existence of multiple fibrous nodules of the omentum, mesentery, and porta hepatis, along with a gastric hemangioma, in a child raises the question of syndromic association. Our search of the English literature revealed only rare mentions of hemangiomas involving the stomach and mesentery or omentum. These lesions have attracted clinical attention by symptoms of obstruction, gastrointestinal bleeding, intussusception, infection, perforation, or vague abdominal pain. Although some tumors exist unnoticed for many decades and are identified only incidentally, others present emergently and require immediate surgical attention. We report the case of a 14-year-old boy who presented with symptoms similar to those for appendicitis or duplication cyst, who was found to have a torsed gastric hemangioma and multiple benign fibrous nodules in the abdomen. The presence of multiple vascular or fibrous lesions is associated with genetic syndromes that can have lifelong and reproductive repercussions; so it is imperative that these tumors be recognized by diagnosticians.
Introduction
Hemangiomas are the most common primary neoplasms of the liver; however, fewer hemangiomas have been documented in other areas of the abdomen. A Pubmed search of the literature for case reports using the terms “hemangioma” and “stomach” and not “metastatic” yielded 127 entries since 1963, 53 of which could be confirmed to involve the stomach; only 25 of these reports were in English. A few of them refer to a primary hemangioma or lymph–hemangioma of the stomach in a patient of any age; the reports in English having readily accessible clinical information are listed in the table in Fig. 1. Search of the computerized pathology database at Penn State Milton S. Hershey Medical Center, Hershey, for the diagnosis of hemangioma in the abdomen over an 11-year period from 2001 to 2012 yielded only 11 cases occurring outside of the liver and, of those, only one presenting in a child. These lesions have attracted clinical attention by symptoms of obstruction, gastrointestinal bleeding, intussusception, infection, perforation, or vague abdominal pain. Although some tumors exist unnoticed for many decades and are identified only incidentally, others present emergently and require immediate surgical attention. We report the case of a 14-year-old boy who presented with symptoms similar to appendicitis or duplication cyst, who was found to have a torsed gastric hemangioma and multiple benign fibrous nodules in the abdomen.
(
Case Report
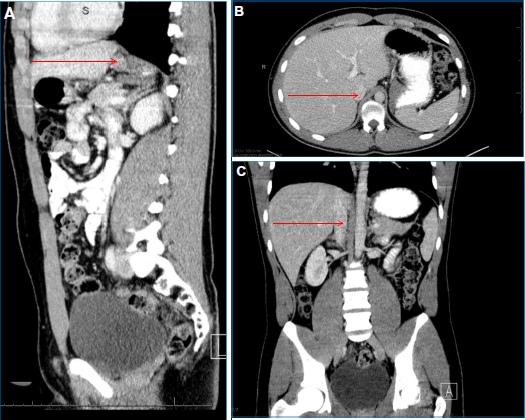
Our patient is a 14-year-old male who presented with 24 hours of constant, worsening right-sided abdominal pain. He denied other symptoms such as nausea, diarrhea, or blood in stool. The patient had no fever and had normal laboratory findings, including no elevation in white blood cell count or shift, normal urinalysis, and normal liver panel. A computed tomography scan was performed, showing an inflamed tubular structure anterior to the colon in the right upper quadrant, which was clearly not the appendix because the appendix was visualized in its typical location (Fig. 1). There was also fluid in the right upper quadrant, with fat stranding around the tubular structure, which was thought to be either a Meckel's diverticulum or an inflamed bowel or gallbladder duplication cyst. With that assessment, the patient was scheduled for a laparoscopic procedure.
Laparoscopic evaluation was chosen as the initial modality to further evaluate the mass due to the uncertainty of the diagnosis. The surgical procedure entailed accessing the abdomen with a 5 mm port. A diagnostic laparoscopy was performed, and based on the findings, the remaining procedure was elected to be completed laparoscopically. Three additional 5 mm ports were placed in the right lower and left lower quadrants, and in the midline suprapubic region. The umbilical port was upsized to a 12 mm port to accommodate a stapler. An additional 5 mm port was placed in the right upper quadrant due to the positioning of additional lesions.
During the operation, a pedunculated mass was visualized along the transverse colon with wrapped omentum. The omentum was excised, and the conical-shaped, inflamed, and ischemic mass was gently peeled away from the colon. The colon was secondarily inflamed but was not involved with the mass and had no serosal injury. When traction was applied to the mass, it could be seen coursing through the greater omentum. The proximal end originated from the greater curvature of the stomach. It was found to be volvulized. This attachment point was resected with an EndoGIA™ linear stapler. There were multiple other masses along the peritoneum in the porta hepatitis. Several other separate mass structures were contained within the greater omentum and removed. Multiple additional masses were found in the right upper quadrant. These did not involve the biliary system but instead were attached to the peritoneum. Ligasure® was used to excise these lesions. Additionally, the appendix was thickened and inflamed and was subsequently excised in the standard fashion.
With the findings of a large pedunculated ischemic mass with multiple other masses from the omentum and peritoneum, the postoperative diagnoses were of gastric duplication cysts, other duplication cysts, and acute appendicitis. Upon receipt by pathology, the main structure was a 5.8 X 2.0 X 1.4 cm tubular, serosa-covered, hemorrhage-filled soft tissue resection. Other specimens were white, firm, solid nodules and tan-pink soft tissue pieces (Fig. 2). Microscopic features of gastrointestinal duplication cysts were not identified, because the bowel wall was not present. There were, instead, blood vessels of varying sizes, including arteries (demonstrated by elastic and smooth muscle actin stains) and venous structures. The gastric mass was acutely hemorrhagic and necrotic, consistent with the history of torsion. The firm nodules of the omentum and peritoneum were composed of mature collagen. This resulted in the final pathologic diagnoses of a hemorrhagic necrotic gastric vascular proliferation; vascular proliferations of the mesentery and omentum; and benign fibrous nodules of the mesentery, omentum, and peritoneum. The patient did well postoperatively and has not had any known sequelae.

(
Discussion
The concurrent existence of multiple fibrous nodules of the omentum, mesentery, and porta hepatis, along with a gastric hemangioma, in a child raises the question of syndromic association. Our search of the English literature revealed only rare mentions of hemangiomas involving the stomach and mesentery or omentum. Angiomas reported were either single or multiple and syndromic, eg, as part of the blue rubber bleb nevus syndrome or von Hippel–Lindau disease. We have reported the case of multiple hemangiomas, the main lesion originating from the greater curvature of the stomach and the others from the peritoneum of the right upper quadrant and the greater omentum. The gastric hemangioma became torsed, causing the patient right-sided abdominal pain.
Vascular tumors, most frequently hemangiomas, are the most common tumors in infants, occurring in 1%–2% children. 1 Prevalence is higher (10%) in premature infants of very low birth weight. 1 Hemangiomas are characterized by overgrowth of normally structured vessels, which show increased endothelial proliferation. Hemangiomas can be present at birth, but often appear within a couple of weeks after birth or during infancy. They can be superficial, deep, or both, with either single or multiple lesions possible. The vessels may vary in size, ranging from dilated thin- or thick-walled channels, to capillaries, to lobular clusters of spindle cells with barely recognizable vascular spaces in cellular hemangiomas of infancy. While hemangiomas are common in childhood, they seldom occur in any intraabdominal site other than the liver or spleen. When they occur in the gastrointestinal tract, the most common site is the small intestine. 2 Complete resection is curative. 3 A computer search of pathology cases at our institution over the previous 11 years yielded no such hemangioma in a child.
The differential diagnoses must be considered. Entities considered among the differential diagnoses of this case include vascular malformations, fibromatoses including desmoid type, lymphangiomas, solitary fibrous tumor, bowel duplication cysts, gastrointestinal stromal tumor, and diverticulum.
Hemangiomas that present in infancy appear similar to vascular malformations, from which they must be distinguished. The current classification system is based on the landmark investigation by Mulliken and Glowacki 4 published in 1982, which proposed a simplified classification of vascular anomalies based on biological activity. As a result, we now recognize two main types of vascular anomalies: vascular tumors and vascular malformations. Differentiating between these two types is essential because their treatment is quite different.
Vascular malformations are abnormal clusters of blood vessels that occur during fetal development. These types of lesions are always present at birth and will typically grow in proportion to the growth of the child. Sometimes, their growth is quite rapid, and without treatment, a vascular malformation will not diminish or disappear.4,5 There are a number of different subtypes of vascular malformations, depending on the predominant channel abnormality. These include capillary malformations such as port-wine stains, lymphatic malformations, venous malformations, arteriovenous malformations, and combined vascular malformations. A vascular malformation consists of vessels which are deformed due to an error in development.
Desmoid tumors are the most common fibrous neoplasms in the pediatric population, with the extremities and trunk often being involved. Over 90% occur spontaneously but can be associated with Gardner syndrome or familial adenomatous polyposis. 6 The fibromas have infiltrative margins and tend to recur if incompletely excised. 7 Desmoid fibromas usually demonstrate beta-catenin mutations detectable by immunohistochemical studies. Fibromas that lack demonstrable beta-catenin mutations are not typical of desmoid fibromas. A case of multiple mesenteric masses in an adult, proven not to be desmoid fibromatosis, has been reported. 8
Duplication cysts are congenital abnormalities that form along the tubular gastrointestinal tract and consist of enteric tissue, but these lack communication with the bowel.9,10 The duplication cysts are typically lined by at least rudimentary mucosa and may demonstrate degenerative or inflammatory changes. Submucosa, muscularis propria, and even serosa may be present. Duplication cysts of the stomach or intestines tend to occur along the omental or mesenteric aspects, respectively.
Solitary fibrous tumors typically arise from the pleura, but nonpleural sites of origin have been documented in younger populations as a bland-appearing spindle cell neoplasm. Cellular foci may alternate with less-cellular fibrous areas in a variety of patterns. The spectrum of solitary fibrous tumors extends to hemangiopericytomas and low-grade fibromyxoid sarcomas, but distinction is made by clinical presentation of a deep soft tissue or serosa-based mass. 11
Hemangiomas involving the stomach.

Lymphangiomas are classified as simple, low-flow malformations with variably sized lymphatic spaces. Inconspicuous endothelium and a watery eosinophilic coagulum in some luminal areas are the basic microscopic features. Smooth muscle can accompany larger vascular spaces. These lesions are irregularly distributed in the soft tissue, often in salivary gland tissue or thymus if in the mediastinum. Occurrence in the abdominal cavity leads to vague symptomatology and late presentation.12,13 Abdominal lymphangiomas have been diagnosed in adults relatively more commonly than in children.
Gastrointestinal stromal tumors are smooth muscle tumors that most frequently arise along the adventitia of bowel. They are densely cellular, well circumscribed, nonencapsulated, and noncavitated. These tumors are slow growing and tend to not be pedunculated and, therefore, only minimally symptomatic. Their histologic and immunohistochemical features distinguish them from the other entities in the differential analysis. 14
Diverticula arise from the wall of a luminal organ and are lined by tissue elements arranged in their regular relationships and contiguous with the lumen. Tissue forming the diverticulum bears histologic features characteristic of the organ or site of origin. Symptomatology varies by size of the diverticulum, presence of heterotopia, and impact of the diverticulum on adjacent structures. 15
In summary, the histologic features of the peritoneal nodules in this boy most closely fit the diagnosis of hemangioma. No genetic testing was performed, because the child lacked any kind of dysmorphism or family history to prompt exploration of this and was also without financial means to undergo extensive testing.
Author Contributions
KAM and DVR conceived and designed the experiments. SEO and KAM analyzed the data. SEO and KAM wrote the first draft of the manuscript. KAM and DVR contributed to the writing of the manuscript. SEO, DVR, and KAM agree with results, conclusions. KAM developed structure and arguments for the paper. KAM made critical revisions and approved final version. All authors reviewed and approved final manuscript.