
Abstract
Advances in technology have improved our ability to measure physical activity in free-living humans. In the last few years, several large epidemiological studies in Europe and the United States have used accelerometers to assess physical activity in children and adolescents. The use of accelerometers to study physical activity has presented some challenges on how to summarise and interpret the data that they generate, however these studies are providing important information on the levels and patterns of physical activity among children and adolescents. Some studies have reported that few children and adolescents appear to meet the recommended minimum of 60 minutes of moderate to vigorous activity per day. Accelerometers have also allowed examination of the relationships between physical activity and health outcomes like obesity and other chronic disease risk factors such as insulin resistance, aerobic fitness, blood lipids and blood pressure. Use of accelerometers allows such relationships to be estimated with a precision that was previously impossible with self-report measures of physical activity. Such information is already advancing our understanding of the role that physical activity plays in preventing childhood obesity and cardiovascular disease risk.
Introduction
Obesity, a condition in which fat stores are enlarged to an extent that impairs health (Garrow, 1999) has increased among children and adolescents in the last 30 years (Reilly et al. 2007). The primary cause of obesity is energy imbalance, but whether this increase results primarily from too much energy intake, too little energy expenditure, or a combination of both is unclear. Recent advances in the measurement of physical activity (the portion of daily energy expenditure that is most amenable to change) using accelerometry have allowed for more precise and objective measurement of physical activity i.e. the energy expenditure side of the equation. The use of accelerometers was at one time confined to use in small groups but are now being more widely used in large epidemiological studies. This is likely due to the growing scale of childhood and adolescent obesity and the willingness of governments and funders to invest in physical activity research. The adoption of accelerometers into physical activity research among children and adolescents has given rise to a new and higher level of measurement precision. This is substantially changing our understanding of the relationship between physical activity and obesity, as well as a range of other health outcomes.
Large studies using accelerometry include the Avon Longitudinal Study of Parents and Children (ALSPAC) in the U.K. (Riddoch et al. 2007), National Health and Nutrition Examination Survey (NHANES) in the U.S. (Troiano et al. 2008), Trial of Activity in Adolescent Girls (TAAG) in the U.S. (Webber et al. 2008) and the European Youth Heart Study (EYHS) in four European countries—Estonia, Denmark, Portugal and Norway (Riddoch et al. 2004). The Millennium Cohort Study (Anonymous, 2008) in the U.K. also has plans to use accelerometers to measure physical activity in children. This paper will discuss the following, with reference to children and adolescents:
Advances in the measurement of measuring physical activity, in particular accelerometers. The focus will be on the Actigraph accelerometer (Actigraph, LLC, Fort Walton Beach, Florida) as it is currently the most widely used (de Vries et al. 2006), although other accelerometer models will be discussed
Issues relating to interpretation of accelerometer data
Use of accelerometers in large epidemiological studies
Results of obesity and cardiovascular disease risk factor research from large, epidemiological studies using accelerometers
Conclusions and future research directions
Physical Activity Measurement
Accelerometers, pedometers and heart rate monitors have all been used in studies of adults and children (Haskell and Kiernan, 2000). Although objective instruments, such as accelerometers, have advantages over subjective instruments (e.g. self report) they still have shortcomings and there are some unresolved issues in the methodology and interpretation of data (Trost et al. 2005).
Self-report
Self-report instruments include diaries, questionnaires and proxy reports i.e. parental report of children's activity. These instruments are relatively cheap and easy to administer and have been used in large epidemiological studies but they have considerable limitations, especially with children. These include difficulties in recalling the intensity and duration of bouts of activity and the lack of objectivity of the instruments (Shephard, 2003). Such limitations are particularly pertinent in children since the majority of children's activity is sporadic in nature and of short duration and difficult or impossible to recall. This has made it difficult to provide precise guidelines about the optimum frequency and intensity of activity that is required to maintain health (Wareham and Rennie, 1998).
Pedometers
Pedometers, which estimate the number of steps taken over a given period are the simplest method of objectively assessing physical activity (de Vries et al. 2006). They are relatively cheap and usually well tolerated by subjects and can therefore be used on large numbers of people. They are limited in that they usually only count the number of steps taken over a given time period (Bassett and Strath, 2002). They can also give estimates of overall activity as in most populations ambulatory movements make up a large proportion of overall activity (de Vries et al. 2006) but they are unable to measure the intensity of physical activity.
Heart rate monitors
Heart rate monitors use the electrical signal from the heart to measure each heartbeat. They can be used to assess the frequency, intensity and duration of physical activity (Janz, 2002). While the relationship between heart rate and activity intensity (measured by oxygen uptake) is linear at moderate intensities, this is not so at higher and lower levels of activity. This may be a source of error since most children spend a large proportion of their day in sedentary and light activity (Riddoch et al. 2007). The relationship between heart rate and physical activity may also be influenced by emotional stress or type of activity undertaken and fitness levels (Janz, 2002). This means that heart rate monitors should be calibrated for each subject by adjusting for fitness level (e.g. resting heart rate) (Livingstone, 1997). This limits their use in large studies.
Accelerometers
Accelerometers have become increasingly popular as an objective method of assessing physical activity. There are a number of commercially available monitors that work using the same principles, normally using electro-mechanical piezoelectric levers to detect acceleration, although solid-state accelerometers are also used. Some are uniaxial and detect acceleration in a single plane, some bi-directional (such as the Biotrainer, IM Systems, Baltimore, U.S.A.) and some are triaxial (such as the Tritrac-R3D, Professional Products, Madison, U.S.A.) and are able to detect acceleration in three planes.
The Actigraph (formerly known as the Computer Science and Applications [CSA]) monitor, produced by Actigraph, LLC (Actigraph, LLC, Fort Walton Beach, Florida) is the most widely used accelerometer (Welk, 2002). The Actigraph is a uniaxial accelerometer that uses a piezoelectric lever to detect acceleration ranging from 0.05 to 2.13G. As the subject moves, the lever bends and a signal is generated in proportion to the amount of acceleration, thus intensity of movement is recorded. The signal is sampled 10 times per second and the values summed over a user-specified ‘epoch’ (Tryon and Williams, 1996). One-minute epochs have generally been used in field studies and this allows approximately 22 days of recording with the 7164 model. (There is also another model, the 256 that has a larger memory). The ideal epoch length has been subject to discussion—it may be that shorter epoch lengths, e.g. 15 or 30 seconds, can better capture the shorter bouts of higher intensity activity that children tend to do (Baquet et al. 2007). The internal clock in the Actigraph allows time and duration as well as intensity of activity to be monitored, thus daily patterns of physical activity can be described. The Actigraph GT1M has now superseded both these Actigraph models although it has recently been reported that the 7164 model output is 9% higher than the GT1M (Corder et al. 2007a). A laboratory study has also found that the GT1M may be less sensitive at low levels of physical activity (Rothney et al. 2008), so caution is warranted when comparing data from old and new models.
The Actigraph has been validated in both children and adolescents. Ekelund et al. assessed the 7164 Actigraph in free-living children. A correlation coefficient of 0.58 (P < 0.01) between counts/min from the Actigraph and physical activity level assessed by using doubly labelled water as the criterion measure was reported (Ekelund et al. 2001). The 7164 Actigraph has been shown to be valid and reliable in children, with a between instrument correlation of 0.87 being reported (Trost et al. 1998).
Interpretation of Accelerometer Data
Though accelerometers are increasingly being used in large studies there are still uncertainties about their use and how to interpret the data. These include: the number of hours per day and total number of days of measurement required to characterise usual activity; the likely compliance in large studies (and the resulting potential for bias introduced by non-response) and the potential for instrument reactivity (the tendency of the instrument to modify normal behaviour). We have used 7164 Actigraph data from a large study of children aged 11–12 years to examine some of these issues (Mattocks et al. 2008). We found that 3 days of measurement of 10 hours per day was the minimum required to reliably characterise physical activity on one measurement occasion (intraclass correlation coefficient [ICC] of 0.7) (Mattocks et al. 2008). This gave a balance between good reliability and the need to retain the sample for longitudinal analyses (Mattocks et al. 2008). Other studies have used an ICC of 0.8 and have estimated that four days of measurement is required to estimate usual activity (Trost et al. 2000). Use of the ICC to calculate the number of days required to estimate usual activity has recently been questioned as it may underestimate the number of days needed to characterise usual activity (Baranowski et al. 2008). Reactivity was present in the ALSPAC sample but the difference between the first and subsequent days of recording was modest, being about 0.1 of a standard deviation. Children who provided valid recordings tended to be slightly younger, shorter and lighter than children who failed to provide valid recordings but the size of these differences were small. More girls than boys returned instruments with valid data (81% of girls vs. 76% of boys; p < 0.001). Parental variables were not strongly associated with compliance. Children were more likely to comply if their mother had a higher level of education but again the differences were small, suggesting a low risk of bias (Mattocks et al. 2008).
Accelerometers are most often used to assess total physical activity (the volume of physical activity in counts per minute [counts/min]) and minutes of moderate to vigorous physical activity (MVPA). Public health guidelines for physical activity are couched in terms of the number of minutes of MVPA accumulated per day (Department of Health, 2004). Current international recommendations for children are at least 60 minutes of MVPA on every day of the week (Department of Health, 2004; Strong et al. 2005). In order to assess compliance with recommendations, cut-points have been used to estimate the amount of time spent in MVPA. Cut-points are defined by calibration studies where counts/min from the accelerometer is compared with a criterion measure such as energy expenditure. Cut-points for MVPA vary between studies and this can lead to substantial under or over-estimation of the amount of MVPA accrued by subjects (Guinhouya et al. 2006). For example, NHANES and EYHS adopt relatively low thresholds for MVPA (906-2020 counts/min), whereas TAAG and ALSPAC use 3000-3600 counts/min. Reilly et al. have suggested that age-specific cut-points be used as it is unlikely that a single cut-point will be appropriate due to the changing relation between accelerometer counts and energy expenditure during growth (Reilly et al. 2006). In ALSPAC, we defined a population specific cut-point of 3600 counts/min for MVPA for use in our cohort (Mattocks et al. 2007).
Most studies use only one measurement occasion to assess usual physical activity. This does not take into account intra-individual variation over longer periods of time and may therefore not represent a ‘true’ level of physical activity. Physical activity shows seasonal patterning, with children being more active in the spring and summer than in the winter months (Mattocks et al. 2007). Intra-individual variation can be assessed by using the intraclass correlation coefficient (ICC), which is defined as the ratio of between individual variance to the sum of the between and within individual variance (Streiner and Norman, 1995). Using four measurements over a one-year period, ICCs for total activity of 0.53 and for MVPA of 0.39 have been reported (Mattocks et al. 2007). This indicates substantial intra-individual variation (an ICC of 1.0 would indicate no intra-individual variation). Serial measurements to assess variability in physical activity are beyond the scope of many studies. However, researchers should be aware that intra-individual variation in physical activity can result in regression dilution bias where the regression coefficient from an analysis that uses physical activity as the exposure may be underestimated (Knuiman et al. 1998). Where physical activity is the outcome, error in measurement of physical activity is unlikely to result in bias, but will increase imprecision (thus leading to wider confidence intervals).
Compliance and Design Issues
Compliance with the study protocol is important in order to maintain sample size. To achieve good compliance, it is important to maintain contact with subjects as frequently as possible (not always easy in large studies where throughput of accelerometers can be at an ‘industrial’ level). There are different ways to administer the accelerometer including face to face or by post. If possible, the initial contact should be face to face as this allows for a more detailed explanation of the protocol and also allows the subject to ask questions. Returning the accelerometer by post works well but returning it in person or collection by the researcher is probably better. Reminder cards or phone calls can both be used both to remind subjects to wear the accelerometer and to return it at the end of the measurement period. The widespread use of mobile phones and the internet in many countries may make maintaining contact easier as emails or text messages can be sent to subjects as a reminder.
Design of a study using accelerometers is, to an extent, dependent on the nature of the research in question. A full discussion of the issues such as the number of hours required to represent a valid day, the number of days required to represent usual activity, the appropriate epoch length and how to identify periods of non-wear are beyond the scope of this article but have been the subject of much discussion and there are some excellent reviews available in the literature. (Trost et al. 2005; Corder et al. 2008) It should be noted, however that such issues are, to an extent, dependent on the age of the subjects. For example, very young children spend fewer hours awake therefore 10 hours of monitoring normally used for older children and adolescents may not be appropriate for young children. The number of days required to represent usual activity may also be age dependent. Studies have generally estimated that children require more days of monitoring due to the variable nature of their activity when compared to adults. (Trost et al. 2005) When designing studies using accelerometers, it is important to achieve a balance between what is scientifically desirable and what is feasible in terms of subject compliance as too great a subject burden may decrease subjects’ willingness to participate.
Results from Studies Using Accelerometers
Levels of physical activity
Comparisons among studies of total physical activity (counts/min) show broadly similar levels by age and gender, although direct comparisons are difficult as age groups vary between studies. Table 1 shows comparisons between four large studies that use accelerometers to assess physical activity.
Child and adolescent physical activity levels assessed by accelerometry.
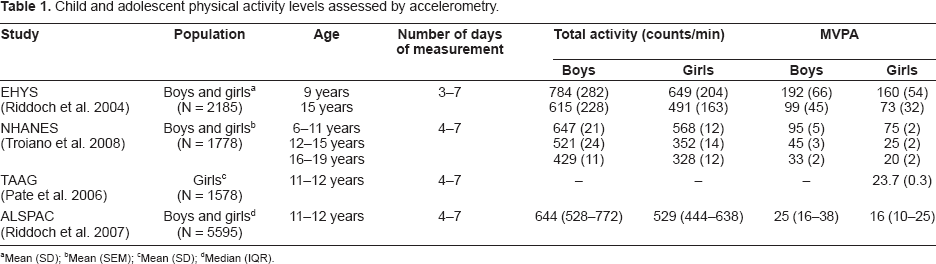
Mean (SD)
Mean (SEM)
Mean (SD)
Median (IQR).
Comparisons of minutes of MVPA between studies are difficult since the cut-points for the lower threshold of MVPA vary between studies within the range 906–3,600 counts/min. Table 1 compares mean daily minutes of MVPA between four studies. As previously mentioned, NHANES and EYHS adopt relatively low thresholds for MVPA (906-2020 counts/min), whereas TAAG and ALSPAC use higher thresholds (3000–3600 counts/min). Some of these differences are expected due to the age, gender and size of the children, although such large discrepancies may also be due to inconsistencies in the calibration studies that produce them. Calibration studies have been performed in different settings (laboratory or free-living), have used different activities (which have relied heavily on ambulatory activities which may underestimate the amount of moderate activity), and have used different criterion measures as the ‘gold standard’ with which to compare accelerometer output.
Physical activity, obesity and cardiovascular disease risk
In ALSPAC we are longitudinally assessing physical activity using the 7164 Actigraph accelerometer at ages 11, 13 and 15 years in approximately 5000 children (Ness, 2004). At the same time, body composition is being assessed using the Lunar Prodigy dual x-ray emission absorptiometry (DXA) scanner. The advantages of using precise methods of both physical activity measurement and measurement of body composition should enable the detection of small associations that may be important at the population level.
In a cross sectional analysis of 5,500 11–12-year-old ALSPAC children (Ness et al. 2007), total physical activity (counts/min) and minutes of MVPA were measured using the Actigraph. Fat mass and obesity (defined as the top decile of fat mass) were measured using DXA. There were strong negative associations between MVPA and fat mass that were unaltered after adjustment for total physical activity. There was also a strong, negative dose-response association between MVPA and obesity. Figures 1 and 2 show the odds ratio of obesity in each quintile of MVPA with the lowest quintile as the referent. The odds of being obese decreases in a linear fashion from the lowest to the highest quintile of minutes of MVPA. There was 97% less chance of being obese for a boy in the top quintile of MVPA when compared with a boy in the lowest quintile of MVPA and 64% less chance of being obese for a girl in the top quintile of MVPA when compared with a girl in the lowest quintile of MVPA. This gender difference is consistent with studies in the adult literature (Cooper et al. 2000).

Adjusted odds ratios for obesity by quintiles of objectively measured minutes of moderate and vigorous activity in 2,622 12-year-old boys from the Avon Longitudinal Study of Parents and Children (ALSPAC).

Adjusted odds ratios for obesity by quintiles of objectively measured minutes of moderate and vigorous activity in 2,878 12-year-old girls from the Avon Longitudinal Study of Parents and Children (ALSPAC).
Data from the EYHS have also shown the association between physical activity measured using the Actigraph and clustered cardiovascular disease risk, including body fat level assessed by skinfolds. Andersen et al. (Andersen et al. 2006) examined the cross-sectional associations between physical activity estimated by accelerometry and clustered cardiovascular risk in 1732 9 and 15 year old children in three European countries. Risk factors assessed were systolic blood pressure, triglycerides, total cholesterol/HDL ratio, insulin resistance, sum of four skinfolds, and aerobic fitness. Clustered risk was estimated using the mean of the Z scores of each individual risk factor. Odds ratios for having clustered risk for ascending quintiles of physical activity were 3.29 (95% CI 1.96–5.52), 3.13 (1.87–5.25), 2.51 (1.47–4.26), and 2.03 (1.18–3.50), respectively, compared with the most active quintile. The association between physical activity (counts/min) and the sum of four skinfolds (mm) adjusted for sex and age was −0.08 (p = 0.0001). A previous EYHS study examined the associations between obesity and physical activity in 1292 9–10 year olds. (Ekelund et al. 2004) Normal weight children accrued more minutes of MVPA per day than obese children (p = 0.022). Total physical activity was associated with the sum of five skinfolds (r = −0.12, P < 0.0001), as was minutes of MVPA (r = −0.15, P < 0.0001). However, minutes of MVPA explained less than 1% of the variation in body fatness (Ekelund et al. 2004). More recently, time spent sedentary, which may be independent of physical activity (Ekelund et al. 2006), has been associated with fasting insulin among 9–10 years olds in the EYHS (r = 0.21, p < 0.0001). (Sardinha et al. 2008)
Similar associations between physical activity and obesity have been found in adolescent girls. Stevens et al. (Stevens et al. 2007) reported from TAAG that girls aged 12 years (n = 1576) with an average MVPA of 12.8 minutes per day (the 15th percentile) were 2.3 times more likely to be overweight than girls with an average MVPA of 34.7 minutes per day (the 85th percentile). Girls aged 12 years in the 15th percentile for MVPA also had 2.6% more body fat, estimated by skin fold measurement, when compared with girls in the 85th percentile. Similarly, girls aged 14 (n = 3085) with an average MVPA of 11.8 minutes per day (the 15th percentile) were 2.0 times more likely to be overweight than girls with an average MVPA of 32.6 minutes per day (the 85th percentile). Girls aged 14 years in the 15th percentile for MVPA also had 1.6% more body fat, estimated by skin fold measurement, when compared with girls in the 85th percentile. (Stevens et al. 2007).
Use of the Actigraph accelerometer is widespread although other studies have been conducted using different models. The Tritrac R3D was used to examine the relationship between physical activity and body fat in 47 Australian children aged 5–10.5 years. Time spent in vigorous and hard physical activity was correlated with body fat (estimated using doubly-labelled water). Time spent in moderate physical activity was not associated with percentage of body fat. (Abbott and Davies, 2004) Comparison between data from different models of accelerometer is difficult due to the differences in output and interpretation of the output. The results from this study suggest similar associations to that of Ness et al. (Ness et al. 2007) i.e. it may be that higher intensity physical activity rather than total activity is more protective against obesity.
As a relatively recent development, accelerometers have yet to be used extensively in longitudinal studies. However, data from the Framingham Children's Study (Moore et al. 2003) has shown that children (N = 103) in the top tertile of physical activity assessed using the Caltrac (Muscle Dynamics, Torrance, CA) accelerometer had smaller gains in BMI and the sum of five skinfolds than those in the lower two tertiles between the ages of four and eleven years. At age eleven years, the sum of five skinfolds was 95.1 mm, 94.5 mm, and 74.1 mm for the low, middle, and high tertiles of activity, respectively (p for trend = 0.045). (Moore et al. 2003).
Conclusions
Accelerometers represent an important advance in measurement of physical activity that will greatly increase our understanding of the nature of the relationship between physical activity and obesity and cardiovascular disease risk factors that have their origins in childhood. Understanding this relationship is of great importance to public health as obesity continues to rise. Numerous groups have already started making important contributions to the literature by incorporating accelerometers into large, epidemiological studies. There are, however, some issues of data interpretation that need to be addressed in order to take full advantage of the capabilities of accelerometry. Despite these differences in data interpretation and differences in definitions of MVPA and varying measurement protocols, data are being published using accelerometers to measure physical activity that are highlighting important associations between childhood physical activity and obesity, as well as a range of other health outcomes. This should provide researchers and policy makers with more robust evidence from which to formulate effective interventions and public health campaigns to reduce chronic disease risk factors and obesity in children and adolescents through the modification of levels of physical activity.
Recommendations for Future Work
Much of the objectively measured physical activity research in large, longitudinal studies is still in its early stages and most analyses to date are cross sectional. As these studies progress, it will be possible to track changes in physical activity and obesity as children go through puberty. Such longitudinal data are vital if we are to address the question of the direction of the association between physical activity and obesity i.e. does low physical activity lead to obesity or does obesity lead to low physical activity, or a combination of the two? Extending these studies into adulthood will also provide data to allow the associations between physical activity in childhood and adult health to be examined—an area that has been under-researched (Sacker and Cable, 2006) yet has the potential to answer important questions on the long term effects of physical activity on a range of health outcomes.
Another question is to determine whether particular patterns of physical activity are beneficial to health. For example, children with the same physical activity level might accumulate their physical activity in very different combinations of intensity, duration, frequency and type. There is also developing interest in the concept of ‘sedentariness’. It is now increasingly accepted that sedentary behaviour is not simply a lack of physical activity but is an independent behaviour (TV/computer use, reading, homework, etc.), which constitutes a potential risk to health irrespective of physical activity level (Ekelund et al. 2006). Thus, it is possible for a child to have high levels of both physical activity and sedentariness. There are limited objective data on sedentary behaviour but accelerometers will allow for the accurate assessment of time spent sedentary. Some preliminary analyses in ALSPAC, however, found no independent association of time spent sedentary and risk of obesity (Blair et al. 2007).
The increased precision in physical activity measurement with accelerometry will also allow us to examine the levels of activity needed to maintain health in children and adolescents. Current guidelines are mostly the result of expert consensus (Department of Health, 2004) due to a historical lack of empirical evidence. It may be that different levels and intensities of activity are required to achieve and maintain different dimensions of health. Given the low levels of physical activity reported by some studies, it may be that the current guidelines need to be reviewed and refined. For example, the level or type of activity that is needed to maintain a healthy weight may be different from that required to maintain healthy bones. As more evidence from accelerometer studies becomes available, it should be possible to provide more precise guidelines relating to different aspects of health.
There is also the potential for using accelerometers in combination with other methods of measurement. The Actiheart combines an accelerometer and a heart rate monitor in one instrument and this may overcome some of the limitations of either method alone (Corder et al. 2007b). Combining accelerometers with global positioning system (GPS) data and geographic information system (GIS) data may also provide valuable information on the environmental factors that influence physical activity. GPS provides data relating to where the subject is and this can be integrated with the accelerometer data so that it is possible to ascertain where physical activity is undertaken in addition to assessing the levels and patterns of physical activity from accelerometer data (Rodriguez et al. 2005). Accelerometer data can also be combined with GIS data so that the possible effects of the environment where the activity is being undertaken can be examined (Scott et al. 2007; Trost et al. 2005).
Although there is considerable potential for accelerometers to improve our understanding the health benefits of physical activity, there are also several issues to be resolved. Where measures of physical activity are repeated, compliance may be a problem as children mature and are less willing to participate. For example, in ALSPAC those with valid accelerometer data numbered 5599 at age 11–12 years and 3800 at age 13–14 years (unpublished data). Such attrition can have a detrimental effect on sample size, as the sample will be limited to those with data on each measurement occasion. Strategies to improve compliance should be explored as this is an under-researched, yet important topic. Statistical techniques to impute missing data and so maintain sample size have also been used in some studies and these may be useful in studies where compliance is a problem (Catellier et al. 2005).
While understanding the relationships between physical activity and health outcomes is important, it is also important to understand what influences or determines physical activity. Identifying the determinants or factors that influence physical activity is an important area of research as this can inform intervention strategies designed to increase physical activity (Sallis et al. 1992). This could allow the identification and targeting of “at risk” groups where the determinant is not modifiable e.g. gender, or the modification of determinants that are amenable to change. An equally important, and poorly understood, area of research is to identify the factors that might determine change in physical activity, as physical activity declines through childhood and adolescence and into adulthood.
Confounding may be a problem in observational studies of physical activity and obesity. Many health behaviours are socially patterned although this appears to be minimal in the case of children's physical activity (Kelly et al. 2006; Riddoch et al. 2007) so confounding by socioeconomic status may not be a problem. However, in longitudinal studies, confounding by pubertal status (as a marker for biological maturity) may be a concern as pubertal status is associated with both physical activity (Riddoch et al. 2007) and obesity. Pubertal status is difficult to measure in large cohorts, in part due to the sensitivity surrounding sexual development in adolescents and Tanner staging by self-report may be inaccurate. Alternative means of estimating biological maturity using predicted adult height (Cumming et al. 2008) bypass the need to collect sensitive data although such predictions may not be accurate and add a further layer of the error in the estimate of biological maturity. Observers trained in Tanner stage assessment are probably a more accurate alternative although this again may present difficulties due to the sensitive nature of the assessment and the need to obtain consent.
Footnotes
Acknowledgements
We are extremely grateful to all the families who take part in ALSPAC and also to the midwives for their help in recruiting them, and the whole ALSPAC team, which includes interviewers, computer and laboratory technicians, clerical workers, research scientists, volunteers, managers, receptionists, and nurses. The United Kingdom Medical Research Council, the Wellcome Trust, and the University of Bristol provide core support for ALSPAC. The U.K. Department of Health, the Department of the Environment, the Department for Education and Employment, the National Institutes of Health, and a variety of medical research charities and commercial companies have supported individual projects. The physical activity research was funded by a grant from the U.S. National Heart, Lung, and Blood Institute (R01HL071248-01A1) while DXA measures were funded by a grant from the Wellcome Trust (GR068049MA).
The authors report no conflicts of interest.