
Abstract
Large randomized trials demonstrated a benefit of adjuvant chemotherapy after resection of the primary colon cancer. It improves overall survival and reduces the risk of death, by 5% in UICC (Union Internationale Contre le Cancer) stage II and approximately 15%–20% in stage III. Fluoropyrimidines have been the standard drugs for the treatment of colon cancer since large randomized controlled trials demonstrated their efficacy and safety in treating patients suffering from this disease. Capecitabine is an orally administered fluoropyrimidine, which is preferably activated in tumor tissue to the active moiety 5-fluorouracil (5FU) and is cytotoxic through inhibition of DNA synthesis. It has proven equivalent efficacy and tolerability despite a changed toxicity profile compared to 5FU with less myelosuppression but more hand-and-foot syndrome. Capecitabine is well tolerated in elderly patients. The oral route of administration avoids frequent clinical visits as well as insertion of central venous catheters. The impact of the particular drug features on daily clinical practice is discussed in this review.
Introduction
Besides lung (1.61 million) and breast cancer (1.38 million), colorectal cancer (1.23 million) was one of the most commonly diagnosed malignancies in 2008 worldwide. 1 In Europe, 436.000 new cases of colorectal cancer (CRC) were diagnosed in 2008 accounting for 13.6% of all diagnosed cancer. 2 Moreover, CRC was the second most common cause of cancer death with 12.2% (n = 212.000) after lung cancer (19.9%) in the same year. Median age at diagnosis is about 65 years. During the last two decades, mortality from CRC decreased, potentially related to improved detection (screening and early diagnosis) and advances in treatment of the disease.3,4 Recent analyses support the hypothesis of a preventive effect of CRC-related death by polypectomy performed during screening colonoscopy. 5
Primary treatment of localized colon cancer (about 75% of patients at diagnosis) is surgery. Whereas very early tumors (Tis or T1 N0 L0 G1 or G2) can be removed by local excision, standard approach for tumors > T1 is a wide local excision. Standardized pathologic assessment should include staging for depth of penetration (T), lymph node status (N), with a minimum of 12 nodes examined, resection margin status, grading (G), tumor type, tumor deposits, perineural growth, extramural invasion, and lymphovascular invasion. Beyond TNM, CRC is classified according to UICC (Union Internationale Contre le Cancer) stages and can be further stratified within lymph node negative stage II disease by the occurrence of clinicopathological risk factors (lymph nodes sampling < 12, poorly differentiated tumor, vascular or lymphatic or perineural invasion, pT4 stage, and clinical presentation with intestinal occlusion or perforation) in high-risk (at least one risk factor) or low risk stage II.
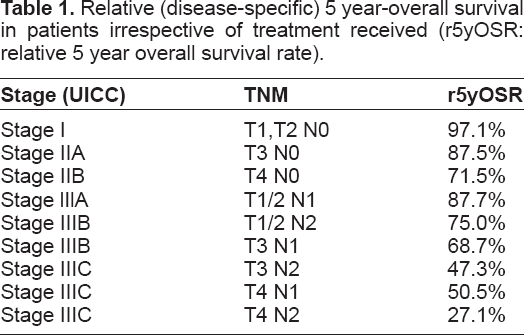
There is significant variability in survival depending on pathological staging (Table 1). Whereas in stage I the overall recurrence rate is about 3.0%–4.6% with a median time to recurrence of 33 months, stage-specific relative 5-year survival is only about 27% for stage IIIC (T4 N2).6,7 In regard of the poor outcome of stage III and partly stage II disease after curative resection adjuvant chemotherapy, which can eradicate occult tumor cells that might have remained after surgery, is commonly administered.
Relative (disease-specific) 5 year-overall survival in patients irrespective of treatment received (r5yOSR: relative 5 year overall survival rate).
The aim of this article is to review the available data on adjuvant treatment with capecitabine for localized colon cancer, in particular prognostic and predictive markers. Data from published trials, reports, and abstracts presented at selected oncology association meetings (eg, American Society of Clinical Oncology [ASCO]) were reviewed.
Development of Adjuvant Chemotherapy
The benefit of adjuvant treatment with fluoropyrimidine after surgery was already suggested more than 35 years ago in a study which demonstrated a significant benefit of adjuvant treatment with 5-fluorouracil (5FU) for stage II and III patients. 8 The first randomized data assessing the benefit of adjuvant systemic fluoropyrimidine based treatment in patients after resection of stage Dukes’ B2 or C colon carcinoma, was derived from the Intergroup (INT) 0035 trial. This trial established 12 months of 5FU and levamisol (lev) as standard of care at least for stage III disease. 9 In the following generation of trials, the role of lev was challenged and it was finally replaced by leucovorin (LV) in combination with 5FU.10–14 Moreover, treatment duration could be reduced to 6–8 months.10,13,15 Therefore, 5FU and LV administered either as bolus (eg, Roswell Park or Mayo Clinic regimen) or as bolus and continuous infusion (LV5FU2) emerged as standard adjuvant treatment for colon cancer.
Role of adjuvant chemotherapy in stage II colon cancer
The INT 0035 trial comparing 5FU and lev with observation alone demonstrated a non-significant increase in 5 year recurrence free survival rate (5yRFSR) (71% vs. 79% for 5-FU/LV, P = 0.10) and similar overall survival (OS) in stage II (Dukes’ B2) patients. 16 The inclusion of both stages (II and III) and thus usually limited number of stage II patients (eg, 318 of 1247 patients included in the INT 0035) is the reason for these non-significant trends in DFS in most of the trials. However, the trial with one of the largest stage II subgroup was the QUASAR (QUick And Simple And Reliable) trial with 2146 stage II patients out of 3239 patients with unclear indication for adjuvant chemotherapy, who were randomly assigned to 5-FU/LV +/–lev or observation. 17 After a median follow-up of 5.5 years, the relative risk of death from any cause with chemotherapy versus observation alone was 0.86 (99% confidence interval (CI): 0.66–1.12) for stage II colon cancer. Exploratory analyses in the QUASAR trial suggested an absolute benefit of 5.4% for high risk and 3.6% for low risk stage II patients (colon and rectum), taking into account the 5 year risk of death of 30% for high and 20% for low risk patients and the above mentioned 18% relative risk reduction.
In regards to the already mentioned low numbers of stage II patients included in trials, several pooled analysis were performed to overcome the statistical limitations of the single trial results.18,19,20
The largest pooled analysis of the Adjuvant Colon Cancer Endpoints (ACCENT) group including 20898 patients (33% stage II) from 18 randomized trials demonstrated a significant benefit of 5% in 8yOSR (66.8% vs. 72.2%, P = 0.026) for adjuvant treatment in stage II disease. 21 Recent population based analyses confirmed the benefit of adjuvant chemotherapy for stage II patients. 22
Furthermore, the addition of oxaliplatin was evaluated in the NSABP C-07 and Multicenter International Study of Oxaliplatin, Fluorouracil, Leucovorin in the Adjuvant Treatment of Colon Cancer (MOSAIC) trial in stage II patients. In the MOSAIC trial the stage II subgroup (40% of patients) had a 3yDFSR 87.0% vs. 84.3% (HR: 0.80; 95% CI: 0.56–1.15) favoring the group receiving FOLFOX, which did not translate into an OS benefit (6yOSR of 86.9% vs. 86.8%).23,24 However, the group of high-risk stage II patients showed a trend towards increased 5yDFSR (82.3% vs. 74.6%; HR: 0.72, 95% CI: 0.50–1.02) with FOLFOX, although again OS was not improved, possibly due to an excess of non-tumor-related deaths.24,25 Stage II subgroup analyses for DFS and OS of the NSABP-C07 trial showed CIs including 1, with a HR favoring 5-FU/LV for OS. 26
Role of adjuvant chemotherapy in stage III colon cancer
The results of the early trials which compared observation to adjuvant treatment in stage III patients (eg, INT 0035 with a reduced risk of recurrence by 41% (P < 0.0001) and increased OSR by 33% (P = 0.006)) as well as the following trials aiming at definition of regimen, mode of administration and treatment duration (eg, INT 0089, “Groupe Cooperateur Multidisciplinaire en Oncology” (GERCOR) C96.1, QUASAR) were mentioned above. In the ACCENT analyses an OS benefit, there was approximately a 10% improvement was demonstrated after 8 years for adjuvant 5FU based chemotherapy after surgery, compared to surgery alone, in stage III disease (8yOSR:53.0% vs. 42.7%, respectively, P < 0.0001). 21 Current standard treatment for stage III patients is adjuvant chemotherapy with a combination of FU and oxaliplatin (eg, FOLFOX or XELOX) based on the clear DFS benefit in all three oxaliplatin trials (MOSAIC, NSABP C-07 and NO 16968/XELOXA) and the significant OS benefit for FOLFOX and XELOX.23,24,27–29
Capecitabine
Capecitabine (Xeloda®; Hoffman-LaRoche, Nutley, NJ) was approved by the Food and Drug Administration (FDA) as an oral prodrug of 5FU in 2005 for use as single agent in the adjuvant setting of stage III CRC.
Mechanism of action, metabolism and pharmacokinetic profile
Capecitabine is an antimetabolite which, when converted to 5FU, causes cell death via RNA- and DNA-related mechanisms. 30 5FU is metabolized to FdUMP (5-fluoro-2′-deoxyuridine monophosphate) and FUTP (5-fluorouridine triphosphate). FdUMP and a folate co-factor bind to thymidylate synthase (TS) to form a covalently bound ternary complex. This binding inhibits the formation of thymidylate, which is essential for the synthesis of DNA and thus inhibits cell division. 31 FUTP inhibits protein synthesis by acting as a false nucleotide in RNA formation. 32 Due to the significant variation of bioavailability, 5FU cannot be given orally. Therefore the oral prodrug capecitabine, a fluoropyrimidine carbamate, was designed. It mimics serum concentration of continuous 5FU infusion. 33
Capecitabine activation follows a pathway with three enzymatic steps and two intermediary metabolites in both liver and tumor tissue (see Fig. 1). The final enzymatic step (conversion of 5′-deoxy-5-fluorouridine to 5FU) by thymidine phosphorylase (TP) seems to take place mainly in tumor tissue due to the higher TP expression. 34
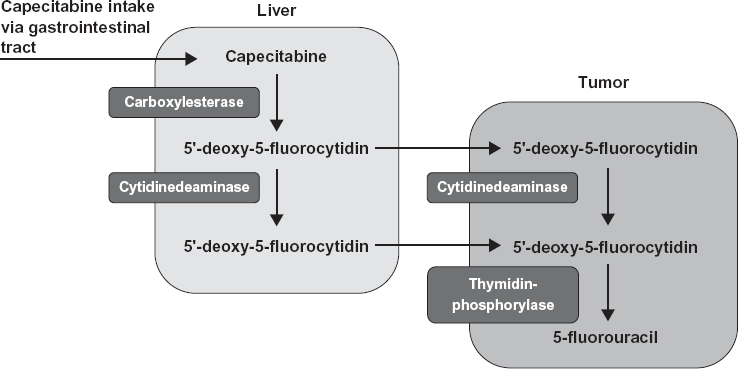
Pharmacodynamics of capecitabine.
Several studies assessed the pharmacokinetics of capecitabine. After oral administration (with water, twice daily within 30 minutes of the end of a meal) capecitabine is absorbed rapidly with blood levels reaching its peak after 1.5 hours. 35 Its bioavailability is nearly 100% and a linear increase is seen in both maximum plasma concentration (Cmax) and area under the curve (AUC) with dose titration. 36 The pharmacology of capecitabine is not significantly affected by gender, race, performance status, body surface area, albumin, or hepatic dysfunction. 30 The half-life of capecitabine is between 0.49 and 0.89 hours, while the half-life of the metabolite (5-FU) extends from 0.67 to 1.15 hours.36,37 The pharmacokinetics are largely dose-proportional. In regards to the mainly renal excretion (over 70% of metabolites), capecitabine is contra-indicated in patients with severe renal impairment (creatinine clearance below 30 mL/min) and should be given at doses reduced to 75% for patients with moderate renal impairment (creatinine clearance 30–50 mL/min) (according to SmPC).
Clinical Studies
Single agent capecitabine for adjuvant treatment of colon cancer
The role of adjuvant capecitabine was evaluated in the Xeloda in Adjuvant Colon Cancer Therapy (X-ACT) trial in comparison bolus 5-FU/LV (Mayo clinic regimen) in 1987 curatively resected stage III CRC patients. 38 In this well-balanced trial capecitabine was at least equivalent to bolus 5-FU/FA in terms of DFS (primary endpoint) (HR: 0.87, 95% CI: 0.75–1.00; P < 0.001) and OS (HR: 0.84, 95% CI: 0.69–1.01; P < 0.001) after a median follow-up of 3.8 years. The 5 year DFS rates were 60.8% and 56.7% for capecitabine and 5-FU/FA respectively. Pre-specified secondary analysis for superiority of capecitabine showed a trend towards superior DFS (P = 0.05) and OS (P = 0.07). The benefit was shown in all subgroups including patients aged > 70 years. Apart from hand-and-foot syndrome (HFS), a significant reduction of the onset of predefined key grade 3/4 adverse events like diarrhea, vomiting, nausea, stomatitis, alopecia, and neutropoenia (P < 0.001) in favor of adjuvant capecitabine was displayed. In a recent update, with a follow up of 6.9 years, results could be confirmed, and moreover the above mentioned superiority analysis became statistically significant for DFS and OS (P = 0.02). 39
Capecitabine based combination chemotherapy for adjuvant treatment of colon cancer
Capecitabine can be safely combined with oxaliplatin as proven in metastatic CRC. 40 In the NO 16968/XELOXA trial (n = 1886), the XELOX regimen was compared with standard 5-FU/LV regimens (Mayo Clinic or Roswell Park) as adjuvant treatment in stage III colon cancer. 28 The addition of oxaliplatin to capecitabine significantly improved DFS (HR: 0.80, 95% CI: 0.69–0.93; P = 0.0045) with a 3-yDFSR of 70.9% with XELOX compared to 66.5% with FU/LV, after median follow up of 57 months despite a decreased treatment duration and dose intensity for the combination treatment. The non-significant trend in OS at the initial report with a 5yOSR of 77.6% vs. 74.2% became significant after longer follow up (median 83 months) with a HR of 0.83 (95% CI: 0.70–0.99; P = 0.0367) and a 7yOSR of 73% vs. 67% for XELOX and FU/LV, respectively. 29
Separately published safety analysis of this study demonstrated less frequent grade ≥ 3 toxicity for neutropoenia (5.3% vs. 10.9%), febrile neutropoenia (0.2% vs. 3.8%), and severe stomatitis (0.6% vs. 79%), but higher rates of skin (3.6% vs. 0.2%) and neurosensory toxicity (8.1% vs. 0%) with the XELOX regimen. 41 Compared to the reported rates of other fluoropyrimidine and oxaliplatin regimens (FOLFOX), XELOX demonstrated similar toxicity, albeit rates of grade 3/4 neutropoenia (41.2% vs. 9%) seemed to be lower and higher for diarrhea (10.8% vs. 19%) with XELOX.23,41,42
Although not fully published yet, the AVANT trial with 3451 patients randomized to FOLFOX or FOLFOX plus bevacizumab or XELOX plus bevacizumab, demonstrated no significant benefit in DFS or OS after a median follow-up of 48 months for the addition of bevacizumab. 3-yDFSR was 76% (FOLFOX4), 74% (FOLFOX4 + bevacizumab) and 75% (XELOX + bevacizumab). 43 Efficacy results favored the chemotherapyalone control arm. Numerically more relapses and deaths occurred in both bevacizumab arms compared to control with FOLFOX. However, although the addition of bevacizumab to oxaliplatin-based chemotherapy was not successful in two large phase III trials, results of the QUASAR 2 trial comparing capecitabine vs. capecitabine and bevacizumab are still expected, scheduled for 2014.43,44
Capecitabine in elderly patients
In a pooled analysis of 7 trials (n = 3351 patients) with adjuvant 5FU with either LV or lev treatment, patients aged > 70 years had no increased incidence of grade 3/4 adverse events, except for occurrence of leucopoenia with 4% vs. 8% (P = 0.05) for treatment with 5-FU/LV and 17% vs. 31%, (P < 0.001) for 5FU/lev in patients ≤ 70 vs. >70 years, respectively. 45 Furthermore, no interaction of age and treatment efficacy was noted. Recent analyses of population-based data from the US confirmed the benefit of adjuvant chemotherapy in stage III patients ≥ 75 years of age. 46 Concerns about oral FU were raised by the still not fully published ACCENT analyses which include the X-ACT (capecitabine) and the NSABP-C06 (UFT/LV) trial demonstrating no beneficial impact of adjuvant oral fluoropyrimidines for colon cancer patients ≥ 70 years of age (DFS HR:1.13, 95% CI: 0.90 to 1.42, OS HR:1.17, 95% CI: 0.92 to 1.48). 47 However, the recent update of the X-ACT trial noted no significant interaction for treatment by age for DFS (P = 0.50) or OS (P = 0.78) and a decreased remaining benefit for capecitabine. 39
A tailored dose escalation strategy for adjuvant capecitabine in elderly patients with colon cancer starting with 2000 mg/m2 was recently published and might be a feasible approach. 48
Whether capecitabine confers a benefit over 5-FU/LV in combination with oxaliplatin in elderly patients is unclear. Whereas in the already mentioned ACCENT analyses showed no benefit for the addition of oxaliplatin to 5-FU/LV in elderly patients (OS HR 1.19, 95% CI: 0.90 to 1.57), this subgroup seemed to derive a non-significant benefit by the addition of oxaliplatin to capecitabine in the NO16968/XELOXA trial (OS HR 0.94, 95% CI: 0.66 to1.34).28,47,49 Pooled data from the more recent trials (NO16968/XELOXA, AVANT, NSABP-C08, X-ACT) demonstrated a significant benefit for DFS (P = 0.014) and OS (P = 0.045) for patients ≥ 70 years of age for the addition of oxaliplatin independent of the used fluoropyrimidine backbone. 50
Other oral fluoropyrimidines for adjuvant treatment of colon cancer
Other oral fluoropyrimidines (eg, oral uracil and tegafur (UFT) or tegafur, gimeracil and oteracil (S-1)) were evaluated in colon cancer, with the majority of trials performed in East Asia. The NSABP C-06 protocol with 1608 patients (stage II 47%) demonstrated non-inferiority of bolus 5-FU/LV and UFT/LV in terms of efficacy with similar DFS, OS, and tolerability with grade 3/4 adverse events of 37.8% vs. 38.2%, respectively. 51 However, UFT was never registered for adjuvant chemotherapy.
Currently, ongoing trials compare S-1 to UFT/LV in 1535 stage III patients and UFT/LV to observation in stage II patients.52,53
Toxicity
The safety profiles of capecitabine and 5FU significantly differ in the adjuvant setting. In the X-ACT trial, the most common grade 3 or 4 toxicities among the 995 capecitabine treated patients were hyperbilirubinemia (20%), HFS (17%), diarrhea (11%), abdominal pain (2%), nausea or vomiting (3%), fatigue/weakness (1%) and neutropoenia (2%). 38 Compared to the safety profile of 5FU (bolus), capecitabine was favorable with a significantly higher rate (all grade) of HFS and hyperbilirubinemia but less stomatitis, alopecia, neutropoenia, diarrhea, and nausea in the adjuvant and metastatic setting (see Table 3).38,54 In both treatment arms, patients with moderate renal impairment at baseline (estimated creatinine clearance 30–50 mL/min) experienced a higher incidence of grade 3 or 4 toxicities. Similar results for elderly patients were demonstrated in several studies. 30 However, grade 3 HFS (17% of patients) is defined as severe skin changes (eg, peeling, blisters, bleeding, edema, or hyperkeratosis) with pain limiting self care activity of daily living, according to common terminology criteria for adverse events (CTCAE) version 4, and might thus have a significant impact on quality of life.
Outcome of adjuvant capecitabine based chemotherapy in colon cancer.

Toxicity profile of capecitabine compared to 5-FU: summary of frequently reported treatment related adverse events (in%) all grades in metastatic CRC. 54

In conclusion, the safety profile of oral capecitabine is generally favorable, with a lower incidence and less severity of life-threatening bone-marrow toxicity and quality of life impacting adverse events like diarrhea, nausea, and stomatitis although the treatment is associated with frequent HFS.
Prognostic and Predictive Factors for Adjuvant Treatment with Capecitabine
High frequency microsatellite instability (MSI-H) or mismatch repair deficiency (dMMR)
MSI-H/dMMR patients have a proven better prognosis in stage II and III colon cancer compared to low frequency MSI (MSI-L) or microsatellite stable (MSS) patients. Pooled data analyses have suggested a detrimental effect for adjuvant treatment with 5FU in patients with stage II MSI-H/dMMR tumors, which could not be confirmed by recent analyses from randomized trials (PETACC 3, QUASAR).55–58 Potential explanation for the discordance of the data might be the insufficient analyses of the patients with respect to germline vs. sporadic MMR defects. 59 However, current guidelines recommend the usage of MSI/MMR status only for determination of prognosis. 60
Hand-and-foot syndrome
Based on results from breast cancer trials, a potentially predictive role of HFS for efficacy of capecitabine was suggested. 61 Recent analyses of the X-ACT trial suggested an association of HFS with outcome. Whereas in patients without HFS, 5yDFSR was 55.5% vs. 54.4% for capecitabine or 5-FU/LV, respectively, patients with grad 1–3 HFS had a 5yDFSR of 61.3% vs. 56.2%. These result indicate a potentially predictive effect of occurrence of HFS for DFS and OS in capecitabine treated patients, which could not be demonstrated with 5-FU/LV. 39 Similar results were shown in perioperative treatment of rectal cancer either as a single agent or in combination with radiotherapy. 62
Dihydropyrimidine dehydrogenase (DPD)
Several studies in the adjuvant or metastatic setting investigated the correlation between expression of enzymes and outcome of 5FU based treatment using different methods and techniques. Studies on DPD expression in primary tumors as determined by IHC (immunohistochemistry) and/or RT-PCR (reverse transcription polymerase chain reaction) with the use of FU in the adjuvant setting found a significant correlation between a low DPD expression and prolonged overall survival63,64 and disease-free survival,63,65 while others found only a trend 66 or no correlation at all. 67 In one large study on capecitabine with or without irinotecan in metastatic setting, a predictive value of DPD expression for OS and PFS was noted. 68 Recent analyses of 498 patients from the NO16968/XELOXA demonstrated significantly better DFS in patients treated with XELOX (HR 2.46, P = 0.0002) for low DPD expression, which was not observed with 5-FU/LV.29,69 Moreover, subgroup analysis indicated a larger benefit for XELOX compared to 5-FU/LV in patients with low DPD levels.
Thymidine phosphorylase (TP)
Conflicting results in correlation of TP expression and clinical outcome for treatment with fluoropyrimidine may be caused by the dual role of TP as an enzyme leading to DNA damage and comprising angiogenic properties.63,70 The precise mechanism through which it promotes neo-angiogenesis are still not fully elucidated. 71 However, a positive correlation between TP expression and microvessel density (MVD) has been reported which suggests that a high TP expression may predict a poor outcome.72,73 Interpretation of the prognostic or predictive value of TP expression is limited by the use of different techniques. Prediction of response to capecitabine-based chemotherapy by TP expression assessed by IHC was better than for TP gene expression by RT-PCR. 70 In the aforementioned recent NO16968/XELOXA analysis, low TP RNA levels were associated with better DFS in patients treated with XELOX (HR:1.73, P = 0.0229). 29
Besides TP and DPD, the ratio (TP/DPD) seems to be predictive for efficacy of adjuvant XELOX in colon or capecitabine based chemoradiation for rectal cancer.29,74
Thymidylate synthase (TS)
The prognostic and predictive role of TS expression was evaluated in several trials using different detection methods (IHC or mRNA) and materials (metastases or primary tumors). Thus, results are difficult to compare. In a meta-analysis of 20 studies in early and metastatic CRC patients with tumors expressing high levels of TS appeared to have a worse overall survival compared to patients with tumors expressing low levels. The retrospective analysis of the CAIRO trial with capecitabine-based chemotherapy did not demonstrate a prognostic value of TS. 68 However, the heterogeneity of the studies and a possible publication bias do not allow a straightforward conclusion.
Further Markers
Recent approaches on prediction of fluoropyrimidine treatment efficacy focus on epigenetic alterations (hypermethylation) or identification of germline polymorphism (single nucleotide polymorphisms (SNPs)).75,76
Predictive factors for toxicity
Clinical factors predictive for FU induced toxicity (eg, diarrhea) are female sex, Caucasian race, and presence of diabetes.77–79 Moreover, toxicity of oral or intravenous FU in the adjuvant setting differed greatly between regions with the highest risk for toxicity being in the US while the lowest is in Eastern Asia. This is potentially related to folate supplementation in the US. 80 Furthermore, the gender-and race-related differences might be influenced by the variable activity of DPD. 81 The leading polymorphism, which accounts for nearly 50% of nonfunctional alleles is the DPYD*2 A resulting in a decreased drug clearance and prolonged exposure with severe toxicities. Complete DPD deficiency is extremely rare, but a partial deficiency is present in 3%–5% of all cancer patients. DPD activity can be evaluated by peripheral blood mononuclear cell radioassay, DPD radioassay genotyping of DPYD gene by Denaturing High Performance Liquid Chromatography (DHPLC), or 2- 13 C uracil breath test (UraBT). The current genotyping strategies are not yet available for routine use. 82 Potentially the simple breath test (UraBT) could be used as a screening tool. 83 However, taking into account the multifactorial nature of fluoropyrimidine induced toxicity in daily practice genotyping for DPD will be initiated after occurrence of unusual toxicity.
Patient Preference
Available data on randomized comparisons of capecitabine and 5-FU/LV in terms of patients’ preference show conflicting results. A trial in 97 metastatic CRC patients comparing capecitabine with 5-FU/LV (bolus of modified de Gramont) in a cross over design demonstrated significantly higher treatment satisfaction mainly based on increased convenience, home-based administration and tablet formulation, despite decreased quality of life with capecitabine compared to the de Gramont regimen. 84 In a similar trial, out of 49 mostly adjuvant CRC patients receiving 6 weeks of capecitabine followed by 6 weeks of a bolus regimen (Nordic FL) or vice versa, the majority (61%) chooses 5FU for further treatment, based on the higher rate of side effects with capecitabine. 85
Place in Therapy
Administration of 5FU-based regimen either requires frequent visits (eg, weekly bolus regimen) or a central venous device (eg, de Gramont regimen). The latter especially may be associated with complications and side effects (eg, thrombosis, pulmonary embolism, infection). In terms of efficacy, capecitabine has proven equivalence to 5-FU/LV in gastrointestinal malignancies in different combinations with a particularly favorable trend as single agent for early colon cancer.86,87 Moreover, cost-effectiveness analyses demonstrated that capecitabine appears to produce greater health gains (mean quality adjusted life year benefit 0.98) at lower cost than 5-FU/LV for the management of CRC patients.88,89
Conclusion
Capecitabine as an oral fluoropyrimidine offers many advantages over adjuvant chemotherapy with bolus 5-FU/LV in the management of colon cancer. These benefits include non-usage of infusion, ports and pumps, favorable tolerability, and trend for superiority in DFS and OS. Owing to these benefits, capecitabine should be the preferred adjuvant treatment of early colon cancer, either as a single agent or in combination with oxaliplatin.
Author Contributions
Conceived and designed the experiments: not applicable. Analysed the data: JQ, DA, AS. Wrote the first draft of the manuscript: JQ, AS. Contributed to the writing of the manuscript: JQ, DA, AS. Agree with manuscript results and conclusions: JQ, DA, AS. Jointly developed the structure and arguments for the paper: JQ, DA, AS. Made critical revisions and approved final version: JQ, DA, AS.
Funding
Author(s) disclose no funding sources.
Competing Interests
A.S. has received honoraria from Roche and Merck Serono. D.A. has received honoraria from Roche and Merck Serono, and research support from Roche.
Disclosures and Ethics
As a requirement of publication author(s) have provided to the publisher signed confirmation of compliance with legal and ethical obligations including but not limited to the following: authorship and contributorship, conflicts of interest, privacy and confidentiality and (where applicable) protection of human and animal research subjects. The authors have read and confirmed their agreement with the ICMJE authorship and conflict of interest criteria. The authors have also confirmed that this article is unique and not under consideration or published in any other publication, and that they have permission from rights holders to reproduce any copyrighted material. Any disclosures are made in this section. The external blind peer reviewers report no conflicts of interest. Provenance: the authors were invited to submit this paper.