
Abstract
Recent years have seen a dramatic change in the approach towards diagnosing and treating Multiple Myeloma. Newer and more target specific approach to treatment has prolonged the survival for patients with multiple myeloma. The proteasome inhibitors make an important class of anti-myeloma drugs that disrupts the proteolytic machinery of the tumor cells preferentially, enhancing their susceptibility to apoptosis. Bortezomib, in particular has shown significant clinical efficacy in myeloma treatment. It is the most commonly used proteasome inhibitor and has been tested to be effective in prolonging the overall survival in several trials. Its combinations with cyclophosphamide and dexamethasone are the treatment of choice for standard risk patients following the mSMART guidelines. The success with its lower dosage in elderly and its proven efficacious subcutaneous usage makes Bortezomib a useful agent for maximizing patient compliance and minimizing therapy related toxicity and costs. This review discusses several trials where Bortezomib has been used as a single/combination agent for front-line treatment of multiple myeloma.
Introduction
Multiple Myeloma (MM) accounts for 10% of all hematological malignancies, with an incidence of 5 cases per 100,000/year and a median age at onset of 65–70 years; there is a slight male predominance. It is diagnosed by the presence of monoclonal plasma cell proliferation with more than 10% plasma cells in the bone marrow, presence of monoclonal proteins in serum, and/or in urine with one or more of end organ effects such as hypercalcemia, renal failure, anemia, or bone destruction (CRAB).1,2 Treatment regimens have undergone immense changes resulting in significant improvements in treatment tolerability. Additionally, improvements in overall survival have been achieved with newer therapies such as proteasome inhibitors and immunomodulatory drugs.3,4 The survival advantages have been more evident for patients less than 65 years of age, of whom 68% and 53% go on living beyond 5 year and 10 years respectively. 5 Overall, decreasing trends in mortality for both newly diagnosed and relapsed myeloma patients suggest promising benefits due to the new drugs. 6 Here, we have reviewed current evidence supporting the use of bortezomib in front-line treatment for previously untreated or newly diagnosed MM.
Diagnosis and Treatment of Newly Diagnosed Patients
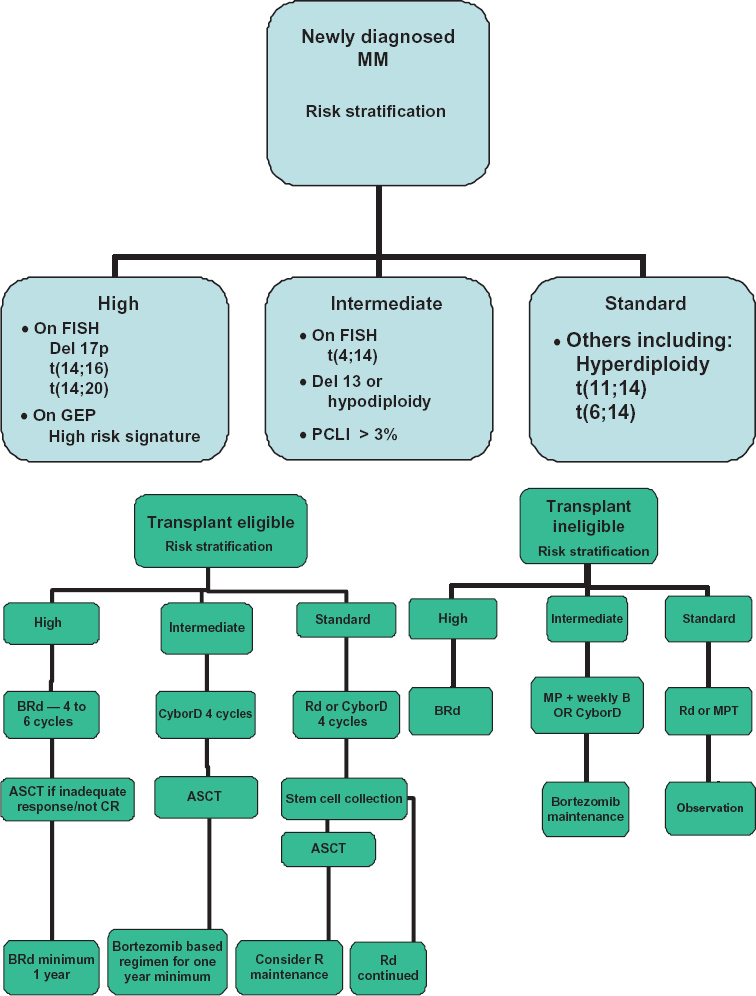
MM requiring therapy is diagnosed according to the International Myeloma Working Group criteria. The presence of serum and/or urine M spike (except in true non-secretory MM cases) along with ≥10% clonalplasma cells in the bone marrow and one or more of the CRAB features indicates MM. 7 Being part of a spectrum of closely associated plasma cell disorders, one must differentiate active myeloma disease from Smoldering Multiple Myeloma (SMM) or the more frequent and benign Monoclonal Gammopathy of Undetermined Significance (MGUS) syndrome, especially given the watch and wait approach for SMM and MGUS.8–11 Following the diagnosis, classification systems such as the Durie Salmon Staging system and the International staging system can be utilized for clinical staging and can be helpful in deciding on timing of initiation of therapy and determining prognosis.12,13 Once diagnosed, MM requires a multi-parametric risk stratification approach for determining the appropriate therapy. Additionally, the decision to pursue further consolidation or maintenance therapy following initial disease control requires scrutiny of disease severity and the response achieved after induction regimens.7,14
Given the significant heterogeneity in the outcomes as seen in this disease despite similar clinical stage classifications, it is now crucial to consider genetic risk factors for optimum therapeutic recommendation.15,18 Ideally, the risk stratification system should incorporate the known independent prognostic factors and allow us to determine prognosis, as well as allow us to select specific therapies for individual groups of patients. Over the years, we have developed such a system that has been since widely adopted (http://www.mSMART.org). The approach is detailed in Figure 1A and B.
(
Proteasome Inhibition as Therapy in Multiple Myeloma
The discovery of the Ubiquitin Proteasome system and its role in protein degradation affecting the cell division has been a major breakthrough in our understanding of the cellular systems degrading unwanted molecules.19,20 We now understand that for sequential degradation, proteins undergo a highly regulated and specific ATP driven tagging of their lysine moieties by a small protein molecule capable of forming chains called Ubiquitin; this involves the ubiquitin associated activating, conjugating, and the ligase enzymes.21,23 These ubiquinated molecules are recognized by large multienzyme ATP-dependent complexes called proteasome which are found in cytoplasm and the nucleus. 24 Proteasomes are comprised of complex inner (oc1 to oc7 subunits) and outer (β1 to β7 subunits) cylindrical structures with three compartments performing catalytic (20S) and regulatory (19S) processes. 25 The 20S subunit core eliminates the ubiquinated proteins via its Chymotrypsin-like (CT-L), Trypsin-like (T-L), and post-glutamyl peptide hydrolyzing (PGPH) proteases activity.25,26 Several important cellular regulatory proteins (eg, I-κB, Cyclins, p53, Bax) undergo ubiquinated degradation. Thus, proteasome inhibition deranges their metabolism, causing cellular dysfunction that culminates with apoptosis (Fig. 2).22,25,27,28 Given that cancer cells display increased susceptibility to proteasome inhibition due to faulty/decreased checkpoint mechanisms, development has begun on proteasome inhibitors for use in cancer treatment.29,30
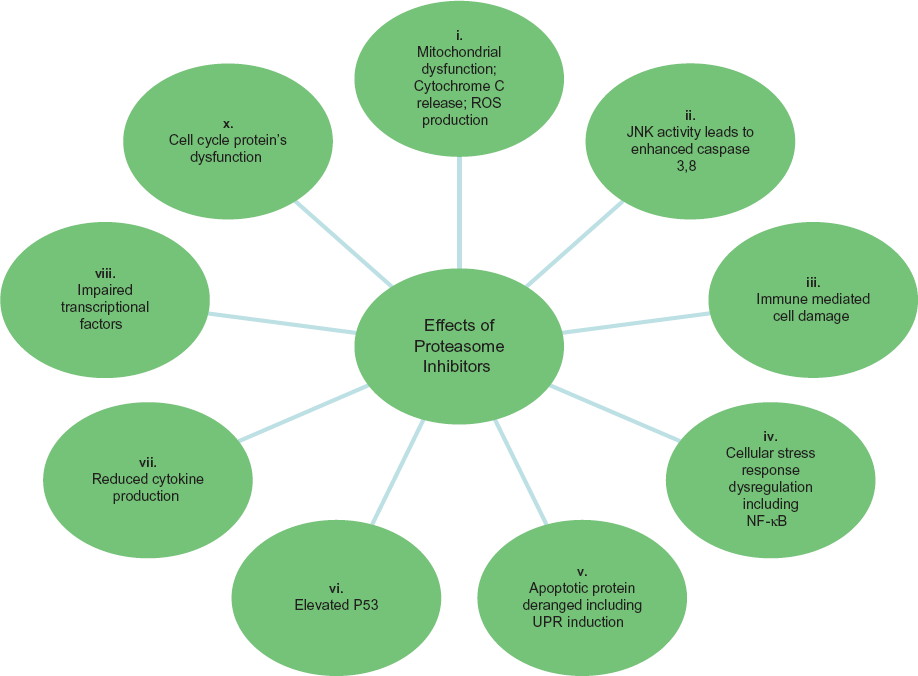
An overview of some major effects of proteasome inhibition.
Bortezomib (PS341, Velcade)
Unlike its non-specific and less potent predecessors, bortezomib's development was conceived as a potent and specific proteasome inhibitor suitable for clinicaluse.28,31–33 Its very specific 26S proteasome inhibitory function has been attributed to the reversible but strong covalent bond formed between its dipeptidyl boronic acid moiety and the threonine proteases of the 20S subunit.34–36 Following the promising activity seen in early phase clinicaltrials,37–40 a series of clinical trials followed, eventually leading to its FDA approval in 2003 for treating patients with relapsed MM.
Mechanism of Action
Bortezomib's mechanisms of action are plethoric and hence a detailed discussion is beyond the scope of this review. We will review the major mechanisms implicated in its efficacy against MM cells.
Bortezomib stabilizes Iκ-B, a small regulatory unit of NF-κB. NF-κB is a heterodimeric cytoplasmic transcription factor and promotes transcription of several anti-apoptotic growth factors, proteins, and cytokines, in response to cellular stress and after its nuclear translocation. 41 NF-κB is also constitutively upregulated in several MM cell lines. Stabilized Iκ-B binds NF-κB, hindering its nuclear translocation and thus preventing the transcription of the following: (1) anti-apoptotic proteins such as Bcl-2, A1, CIAP-2, and XIAP; (2) cell cycle regulators cyclin-D1 and c-Myc; (3) growth and anti-apoptotic factors such as IL-6 and VEGF, which is essential for myeloma cells and bone marrow stromal-cell signalling; and (4) adhesion molecules such as vascular adhesion molecule (VCAM-1) and intracellular adhesion molecule (ICAM-1) (Fig. 2).41,42 As NF-κB is highly expressed in myeloma cells,43,44 its inhibition by bortezomib promotes their apoptosis. Other mechanisms include: (a) stimulation of classical stress response proteins; (b) mitochondrial calcium transport and membrane potential disruption generating ROS. These mechanisms are also associated with bortezomib mediated apoptosis; (c) activation of JNK releasing mitochondrial second mitochondria-derived activator of caspases (Smac) and cytochrome-c causing caspase activation and (d) induction of intrinsic and extrinsic apoptotic pathways. These preceding mechanisms are the other significant NF-κB independent pathways causing apoptosis in bortezomib treated Myeloma cells (Fig. 2).
Pharmacology
Bortezomib is recommended intravenously or subcutaneously at a dose of 1.3 mg/m2 twice weekly for two weeks and with a treatment free week in a 21 day cycle.45,46 However, doses of 1.0 to 1.6 mg/m2 have been used in various trials, either in combination with dexamethasone or as part of multidrug combinations. 47 On intravenous administration, bortezomib is 80% plasma protein bound and shows rapid tissue redistribution, with a first dose elimination half-life varying between 9–15 hours and repeated dosage reducing its plasma clearance substantially. 48 While subcutaneous administration takes longer to reach peak serum concentration compared with intravenous route (30 minutes versus 5 minutes), the mean systemic exposure (56.8 nghr/mL versus 42.9 nghr/mL) and the 20S inhibitory activity (63.7% versus 69.7%) of bortezomib displays close similarity between subcutaneous and intravenous routes, suggesting similarities in their elimination half-lives.46,49
Potential bortezomib side effects. 101

In the body, bortezomib displays tissue selectivity with predominant accumulation in the gastrointestinal system, which contrasts its weak distribution in the subcutaneous fat and skin and complete inaccessibility of the centralnervous system, testis, and eye. 28 Hepatic CYP-450 isoenzymes metabolizes it via oxidative deboronation forming M1 and M2, two minor metabolites which undergo biliary clearance, making it a safer alternative for patients with the concurrent kidney disorders which can be rather commonly associated with Myeloma.28,50–52
Peripheral neuropathy is a major non-hematologic toxicity induced by bortezomib and can require mid therapy dose reductions or even discontinuation.53–55 Other significant toxicities include cytopenias, gastrointestinal distress, fatigue, cardiac side effects, infections, re-activation of shingles, and, rarely treatment-related mortality. 56 Once-weekly and reduced intensity regimens have been effective at maintaining therapeutic advantages, with reduced toxicity and treatment associated weekly patient visits.57,58 Recent trials using bortezomib's subcutaneous administration have reported a reduction in the neurotoxicity along with the possibility of self administration. Such changes can significantly alter patient's quality of life and hence need further investigation. 46
Clinical Results
Bortezomib ± Dexamethasone
Bortezomib was first used as a frontline single agent for treatment naive myeloma patients by Jagannath et al. 55 This open label Phase II study enrolled patients with newly diagnosed myeloma with no prior therapy or minimal exposure to steroids. Bortezomib was administered at a dose of 1.3 mg/m2 and the responses achieved were measured using EBMT criteria. Of 32 patients, 13 responded by the second cycle, resulting in 1 complete response (CR), 3 near complete responses (nCR), and 9 partial responses (PR). With the addition of dexamethasone in 22 patients, additional responses were observed in 15 of these patients. While bortezomib alone achieved a 40% response rate (RR), the RR further improved to 88% in combination with dexamethasone. An estimated 87% survival at 12 months was noted. Ten patients experienced grade 2 or 3 neuropathy while 8 patients reported painful neuropathy. Neuropathic pain disappeared within a median of 3 months of stopping bortezomib. Other noted side effects were myalgia, fatigue, and constipation of varying severity. In their extended follow-up, 59 the overall response among patients receiving the BD combination was 90%, with 42 in VGPR or better (19% in CR/nCR). The estimated survival at 4 years was 67%.60–62

Richardson et al 63 reported a time to progression (TTP) of 17.3 months post-bortezomib treatment in 64 patients, with 41% ≥ PR. In that study, bortezomib was administered up to 8 cycles or 2 more cycles post CR achievement while on the regimen. No significant correlation between adverse cytogenetics features and the responses achieved were noted. Median Overall Survival (OS) was not reached and a 30-month OS was estimated as 79%, with a trend towards better OS for patients receiving SCT of 82% compared with 78% OS for bortezomib-only treated patients.
PETHEMA phase II trial utilized alternating bortezomib and dexamethasone administered to 44 younger patients as induction regimens. The trial achieved a rapid M spike drop (>80%) within the first couple of treatment cycles. Post-induction, 65% patients had PR or better, showing 88% response rates after the ASCT with 33% immunofixation negative. Common side effects included neutropenia (72%), peripheral neuropathy (25%), thrombocytopenia (27%), and gastrointestinal distress, with other less frequent side effects including skin rash, fatigue, and hepatotoxicity. This trial highlighted the potential of using bortezomib and dexamethasone as potential induction regimens with quick responses, no stem cell collection issues, high post-ASCT response rates, and manageable toxicity. 64
These trials showed promising results from using bortezomib for newly diagnosed patients and increased the possible spectrum of future drug combinations.
Bortezomib Combinations
Bortezomib-Melphalan-Prednisone (VMP)
In their phase 1/2 trial with 60 elderly untreated MM patients, Mateos et al highlighted the benefits of using bortezomib in combination with melphalan and prednisone (VMP) when compared to the standard MP regimen. Seventy percent of patients showed an objective response within the first cycle. Overall response rate was 89% (32% CR) with VMP compared with 42% overall response rate for MP. In addition, the 16-month event free survival rate was significantly higher with VMP than MP (83% as compared to 51%, P < 0.001). 65 With a longer follow-up of 38 months, the results remained significant, showing improved survival for patients treated with VMP when compared to MP (85% compared to 38%, P < 0.0001). Adverse prognostic markers such as t(4;16), and t(14;16) had no impact on outcome, suggesting the beneficial effect of bortezomib for these high-risk patients. 66
The VISTA trial 56 was the first prospective, randomized open labelled phase III trial which tested the efficacy of VMP as front line treatment in previously untreated MM patients. Importantly, the median age of treated patients was 71 years, who would traditionally not classify for high dose therapy and SCT. Overall, 682 patients of whom 340 received VMP and 337 received MP. The median time to progression was 24 months in the Bortezomib arm as compared with 16.6 months in the MP arm.
CR rates were higher with VMP than MP (30% and 4% respectively, P < 0.001). More importantly, age and renal impairment did not affect the results for patients in the VMP arm as the CR rates achieved and the median time to progression (TTP) were identical. Patients with high risk cytogenetics subgroup [including t(4;14), t(14;16), and deletion 17p] had similar TTPs as compared to the subgroup with standard risk cytogenetics. A three year follow-up showed a 35% reduction in risk of mortality for VMP treated patients and an overall survival of 43.1 months in the MP arm and not reached for the patients on VMP arm. OS of patients below 75 years of age was better than the older subpopulation but no such significant trends were seen between groups based on creatinine clearance or cytogenetic abnormalities. More importantly, peripheral neuropathy resolved in the majority of patients within a median of 5.7 months. 67 This landmark trial displayed the potential usage of bortezomib in achieving reduced toxicities and greater therapeutic advantage amongst elderly patients and diverse subgroups of newly diagnosed patients with MM, prompting further trials of bortezomib in various combinations.
Mateos et al then compared VMP to VTP as first randomization 1:1 induction therapy, followed by VT versus VP maintenance in second randomization elderly untreated patients, using reduced intensity bortezomib in each arm. 57 Of 260 patients enrolled, 130 were treated in each arm and achieved comparable RR (≥PR) of 80% and 81% in VMP and VTP respectively. After VT or VP maintenance, complete remission rates of 44% and 39% respectively were noted; these were higher than the 30% response rate reported in the VISTA trial. Higher toxicities were noticed in the VMP arm, with 39% of patients experiencing thrombocytopenia compared with 12% in the VTP group. More serious adverse events were noted in the VTP (31%) arm when compared to VMP (15%) arm, which led to an increased discontinuation of therapy in the VTP arm. Patients from both arms were stratified based on cytogenetic abnormalities into high and standard risk groups and showed significant differences in the 3 year OS (55% vs. 77%—first randomization) and (60% vs. 85%—second randomization). Second randomization depicts patients who after successfully completing induction, and then went on to receive maintenance upto 3 years for high versus low risk respectively. The survival data didn't vary in either arm irrespective of the maintenance therapy used and emphasized the use of such regimens for elderly patients.
In 44 transplant eligible patients, Gasperatto et al 68 used a short induction of VMP with plans for ASCT after 2 to 6 cycles. High responses were achieved post-induction with 95% RR, including 18% ≥ CR, 27% VGPR, and 50% PR. More importantly they demonstrated rapid achievement of response to VMP as previously noted in the VISTA trial. Such short courses of therapy could reduce the side effects and potentially enhance adherence to the treatment regimen.
As a conditioning regimen, bortezomib combined with high dose melphalan has been tried effectively by the IFM group in their phase 2 trial, wherein 53 untreated patients were dosed with 1 mg/m2 of bortezomib on days –6, –3, –1, 1 and 4, along with melphalan 200 mg/m2 on day –2. 69 The results were promising, with 70% and 32% VGPR and CR rates respectively, much higher than the matched control (11% CR). No engraftment failure was reported and all patients completed the conditioning with no exacerbation of any pre-existing neuropathy. While 5 serious adverse events were noted, no deaths occurred. The trial showed promising use of bortezomib as a combination option with HDM prior to ASCT.
Bortezomib-Doxorubicin-Dexamethasone (BAD/PAD/BDD)
Several trials have assessed the outcomes among patients induced with bortezomib, doxorubicin and dexamethasone (BDD) followed by stem cell transplantation.47,70,71 One such trial compared combinations of 1.3 mg/m2 of bortezomib with doxorubicin and dexamethasone (PAD1) to 1.0 mg/m2 bortezomib with doxorubicin and dexamethasone (PAD2) in their phase I and II trials.47,70 Pre-transplant, PAD1/PAD2 induction had a 24%/11% CR, 33%/26% VGPR and high ORR's (95%/89%). After transplantation, VGPR increased in both PAD1 and PAD2 arms by 81% and 53% respectively. The 2 year OS was 95% and 73% for PAD1 and PAD2 respectively, favoring PAD1 over PAD2.
Jakubowiak et al 71 evaluated pegylated liposomaldoxorubicin (30 mg/m2) in combination with bortezomib (1.3 mg/m2) and dexamethasone (20 to 40 mg/day). This phase II, single arm, 40 patient trial had 6 three-week cycles of therapy. After 6 cycles, over 37.5% nCR and 57.5% nCR and VGPR were achieved. Thirty patients who underwent SCT further improved their responses to 76.6% ≥ VGPR from a previous level of 57.5%. Those who achieved ≥VGPR showed significantly better PFS at 1 year (100%) than those who didn't (82%). Additionally, the estimated PFS was significantly higher in VGPR patients than those who had PR or less (93% vs. 63%, P = 0.3). No differences were noted amongst patients when risk stratified according to chromosomal aberrations. With a manageable toxicity profile, the combination offers an induction option for patients going to SCT.
A phase II study specifically aimed at high risk patients (ISS stage II, III, and EMD) was conducted by Landau et al using BDD. 72 Depending on the response post 3 cycles of BDD, patients either got 2 cycles of thalidomide (T) and dexamethasone (D) (if ≥ PR) or 2 cycles of BTD (SD, PD). Of the 42 patients, 34 (81%) responded to treatment, with 26% in CR/nCR and 40% ≥ PR. The 19 patients who had a suboptimal response (<PR) post BDD therapy further received sequential BTD; 8 patients attained deeper response to the additional therapy. With a median TTP of 39 months and 2 year OS of 83%, the regimen showed promise not only for the high risk patients, but also for patients with renal failure, as a majority of patients with acute renal failure showed significant improvement. 71
Two cycles each of VAD and BTD consecutively followed by weekly (4 out of every six weeks, up to 4 cycles) bortezomib maintenance, was examined by Kim et al in a phase II trial of 71 patients. 73 They reported high response rates of 97% ≥ PR and 54% ≥VGPR pre-transplant, which further spiked over 98% ≥ PR, 82% ≥ VGPR, and 75% < CR/nCR after SCT. These responses were much higher than those achieved in other comparable trials.53,54 Although small, the poor cytogenetics patient subgroup responded well, showing no increased risk of mortality or adverse effects on stem cell collection. Median PFS was 29.4 months, while the median OS was not reached after 52.7 month follow-up.
The HOVON-65/GMMG-HD4 randomized phase III trial recently compared the efficacy of vincristine doxorubicin dexamethasone (VAD) versus bortezomib doxorubicin dexamethasone (PAD) as induction agents along with thalidomide (T) or bortezomib (B) maintenance therapy, respectively. Post induction, patients received high dose melphalan followed by autologous transplant. A total of 833 patients were randomized with 414 in the VAD arm and 413 in the PAD arm. Throughout the treatment protocol, the VAD arm in comparison to PAD showed significantly (P < 0.001) lower CR/nCR (9%/21% vs. 12%/26% three months after HDM-1 and 12%/26% vs. 12%/38% on protocol) and VGPR (60% vs. 40% post three months of HDM-1 and 75% vs. 61% on protocol) rates. PFS at 3 years was 48% versus 42% and OS at 66 months was 78% versus 71% on comparing PAD with VAD respectively. These results also favored bortezomib maintenance over thalidomide, as OS was higher in the PAD group. Among patients with renal insufficiency, bortezomib showed significant improvement in PFS (30 vs. 13 months, P = 0.004) and OS (54 vs. 21 months, P < 0.001) when compared to the VAD/T arm. Similar significant results were noted in high risk cytogenetics (–13/13q-and –17p) when compared to standard risk patients. This trial showed the unprecedented advantage of using bortezomib as both induction and maintenance, especially in patients with high risk features. 74
Bortezomib-Cyclophosphamide-Dexamethasone (Cybor-D)
CyborD was used as induction therapy for 33 newly diagnosed patients in a single arm phase II study at the Mayo Clinic, 75 demonstrating high response rates after four 28 days cycles of therapy. Among the 28 patients who completed 4 induction cycles, the ORR was 96% with 46% in CR + nCR and 71% ≥ VGPR. Additionally, all treated patients had ORR of 88% (≥ PR) with 61% ≥ VGPR. Rapidity of response to therapy was most evident within the first two therapeutic cycles. Cytopenias and hyperglycemia along with grade I PN (46%) were the commonly experienced toxicities. However, this regimen used high dose dexamethasone, which is currently no in common usage.
Kropff et al used a standard dosage of dexamethasone and bortezomib together with 900 mg/m2 of cyclophosphamide (maximum tolerated dose) as the induction regimen. After four cycles of induction, high response rates with ≥77% PR and 10% CR were achieved; 28 of 30 patients had an adequate stem cell harvest, of which the majority had adequate stem cell collection in one apheresis. Patients with –17p and t[4;14] showed inferior ORR compared to standard risk patients (62.5% vs. 86.5% ≥ PR respectively). 76 These results were similar to other comparable trials, for example, the 75% ORR with 41% VGPR or better in the VCD arm of the Evolution trial, and displayed rapid reduction of M spike, translating to faster responses.77–81 While BDD appears to show rapid response in patients, any assessment of its clinicalutility needs further, larger cohort-based studies.
Bortezomib Immunomodulatory Combinations
With Thalidomide
In one of the early trials, 38 newly diagnosed MM patients were treated with bortezomib, thalidomide, and dexamethasone (BTD). A rate of 87% RR was noted, together with 16% CR and improved responses in 25 patients (66%), who subsequently underwent transplantation and of which 3 with resistant disease achieved PR or CR and 7 with a previous PR upgraded to CR, resulting in an overall CR rate of 37%. With rapid median time to remission (0.4 months) and, more importantly, no mortality, this regimen showed potential for its addition to the treatment armamentarium for untreated MM patients.
Ghosh et al recently showed the benefits of using bortezomib with thalidomide in an upfront setting. This phase II trial of a steroid free regimen achieved high RR (≥PR = 81.5%) with 25.6% ≥ nCR and a 3 year OS of 74% (CI: 54%–89%) without SCT. Toxicity included a 22% Grade 3 PN, with resolution of symptoms on therapy discontinuation seen in 80%. Importantly, no thrombotic events or hyperglycemic complications were noted, a phenomenon which has previously been reported with thalidomide combinations. 82 Comparable results were noted with bortezomib, pegylated doxorubicin and thalidomide combination in another trial with 78% ORR, of which 35% achieved CR + nCR. Along with reduction in the severity of sensory neuropathy, the overall toxicity profile was manageable and no treatment associated deaths. 83 The promising results of such steroid-free regimens need further phase III verification for their clinical efficacy and relatively low toxicity.
The GIMEMA group conducted a Phase III study that evaluated the efficacy of VTD vs. TD as induction regimen, followed by tandem SCT and consolidation with the same regimens respectively. Significantly higher RR were noted in the VTD arm when compared to TD arm (30% vs. 11% CR respectively; P < 0.0001). The 3 year probabilities of relapse were 29% and 39% along with 68% and 56% PFS at 3 years, for VTD and TD arms, respectively. No significant differences were observed in OS. Patients with t(4;14) had an accelerated progression, relapse, or death in the TD arm with a 37% and 63% PFS at 3 years for the t(4;14) positive and negative patients, respectively. No such correlation could be drawn in the VTD arm. More Grade 1 and higher side effects were noted in the VTD arm, with constipation, neuropathy, and skin rash being the most common. Patients with high-risk prognostic features such as high lactate dehydrogenase levels (>190 U/L), age (>65 years of age), del3q, low bone marrow plasma cell count (<50%), t(4;14), +/–del17p, and high ISS stage had significantly improved outcome with VTD than TD arm. 54
The PETHEMA group 84 randomized 386 untreated patients to compare efficacy of BTD (130 patients), TD (127 patients), ands VBMCP/VBAD/B [vincristine, BCNU (bis-chloronitrosourea), melphalan, cyclophosphamide, prednisone/vincristine, BCNU, adriamycin, dexamethasone/bortezomib—129 patients] as induction regimens. Results showed the superiority of VTD over other treatment arms with significantly high CR (35%) on comparison with TD (14%) and VBMCP/VBAD/B (21%). In cytogenetically stratified high risk groups, high CR rates were seen with VTD when compared with TD (35% vs. 0%, P = 0.002) or with VBMCP/VBAD/B (35% vs. 22%, P = 0.02). In VBMCP/VBAD/B group the CR rate increased from 8% to 21% after completing 2 cycles of Bortezomib post 4 cycles of VBMCP/VBAD. While higher discontinuation within induction phase was noted with TD (n = 29) and VBMCP/VBAD (n = 15), only 9 discontinued in VTD due to progressive disease. A quarter of the 45% experiencing PN required dose reduction in VTD arm. This was much higher than the 8% and 15% in TD and VBMCP/VBAD/B arms, respectively, experiencing PN. PFS after a median of 33.1 months follow-up was also significantly higher in VTD than with VBMCP/VBAD/B or VT (56.2 vs. 35.3 vs. 28.2 months respectively) while no such differences were noted in OS. This trial's results support the use of VTD as an induction regimen in MM patients.
Mateos et al 57 took a less intense approach by using bortezomib once weekly instead of the usual twice weekly in combination with either MP or TP followed by maintenance with VP or VT. This randomized trial had 260 elderly patients, with patients receiving 6 cycles of induction and then up to 3 years of maintenance. The trial showed similar efficacies of both regimens in terms of CR, OS, and PFS. More importantly it showed improvement in the grade 3 or higher neurotoxicity seen with reduced dose of bortezomib (5% in VMP as compared to the 13% in the Vista trial). VTP was associated with higher cardiac adverse events and neurotoxicity while BMP had infection as a primary non-hematologicaltoxicity warranting antibiotic treatment prophylaxis in future such combination. Also of note was the fact that despite a larger subgroup analyzed in comparison to the VISTA trial, no significant prognostic benefit was achieved in the high risk cytogenetic group (t4;17 and del17p), although significant benefits were observed for patients with hyperdiploidy over non-hyperdiploidy with BTP (P = 0.02).
Moreau et alexamined the clinicalefficacy of using low dose bortezomib in combination with thalidomide and bortezomib, when compared to the normal dosage of the VD combination. By inducing significantly deeper responses (VGPR being 49% vs. 38%) a marked reduction in neuropathy (14% vs. 34%) among the 199 patients enrolled was noted. 85
More recently the multicentre study comparing VTD, VMP, and VD (each arm consisting 100 patients) showed deeper responses with the use of VTD when compared to VMP and VD. Of more value were the enhanced responses seen on bortezomib maintenance in all treatment arms and the absence of additional neuropathy. 86
BTD has also been shown to induce persisting molecular remissions when used as consolidation therapy after autologous SCT. The results emphasized major tumor shrinkage as shown by the use of RQ-PCR for minimal residual disease detection after the consolidation, with no relapse after a median of 42 months; these are certainly promising results. 87
With Lenalidomide/Revlimid
Lenalidomide (L) has shown favorable results when used as an induction agent in combination with bortezomib and dexamethasone by Richardson et al. 58 A total of 66 patients were administered eight 3 week cycles of BLD with a 100% > = PR rate in treated patients. With 39% ≥ nCR and 67% ≥ VGPR, and despite the ASCT, PFS in both the transplant and non-transplanted group was 75% (95% CI: 63%, 84%). The 18 month OS rate was 97% (95% CI: 88%, 99%), irrespective of the transplant status. Sensory neuropathy (80%), fatigue (64%), and neuropathic pain (32%) were major adverse effects reported and, more importantly, no treatment related mortality was noted. More studies are needed to assess clinical feasibility of such combinations.
Multi-drug combinations
The Evolution phase I and II trials analyzed responses to various combinations of bortezomib (V) with cyclophosphamide (C), thalidomide (R) and dexamethasone (D) in terms of response, adverse events, overall survival, and minimal residual disease and assessed such differences achieved amongst the treatment arms.81,88
The Phase I trial showed feasibility of combining different groups of drugs (VDCR) and achieving high RR of 96% with 40% CR/nCR and 68% ≥ VGPR. Peripheral neuropathy was the major adverse event which improved/resolved in 85% patients on treatment completion. Additionally, no thrombotic events were noted. Such promising results led to the phase II multicentre randomized trial of VDCR, VRD, VDC, and modified VCD (with additional cyclophosphamide dose), using eight 21 days cycles for each regimen. Overall, 122 patients were enrolled, with 88%, 85%, 75%, and 100% in ORR (33%, 32%, 13%, and 41% having ≥VGPR respectively) among the VDCR, VDR, VDC, and VDC-modified arms respectively, prior to ASCT. PFS at one year for VDCR, VDR, VDC and VDC-mod was 83%, 68%, 97%, and 100% in non-ASCT patients and 86%, 83%, 93%, and 100% including the ASCT subgroup in each arm respectively; OS was 100% at one year in all arms. While no added advantage was noted in adding alkylating agent to VRD as initially speculated, better responses with lesser toxicities were seen in the VCD-mod and VDR arms.
A retrospective analysis, done at the Mayo clinic compared RD, CRD, and VCD and reported no conclusive PFS or OS advantage with any of the regimens. 89 Higher responses were achieved with VCD but VCD had a higher incidence of neuropathy when compared to either RD or CRD.
The significance of maintenance was examined in the randomized phase III trial assessing VT maintenance used post-VMPT induction and its efficacy when compared to VMP induction without maintenance. 90 Among the 511 patients enrolled, a first cohort of 139 patients received twice weekly bortezomib for 9 six weekly cycles while the remaining patients received bortezomib once a week for 9 five week cycles of treatment, intending to reduce PN. This trial was beneficialto evaluate appropriate dosage for transplant in eligible patients who experience diminished toxicity with reduced frequency of bortezomib administration. A remarkably decreased incidence of PN with uncompromised drug efficacy was noted with the reduced schedule of bortezomib. More importantly, the cumulative treatment dose was similar in both arms despite changes in frequency of administration, suggesting more dose reduction with the twice weekly schedule. Reduced PN also translated to better treatment compliance in the modified arm. VMPT-VT was more efficacious than VMP arm with an enhanced 3 year PFS (56% vs. 41% respectively) and time to therapy (72% vs. 60% respectively). CR and VGPR were also significantly better with VMPT (prior to maintenance) than VMP (38% and 59% vs. 24% and 50% respectively). Sixteen treatment-related deaths occurred in total, while in general more side effects were evident in VMPT than in VMP (38% vs. 28% respectively). Additionally, there were more cardiac adverse effects for VMPT than VMP (10% vs. 5% respectively). Neuropathy was more common in people undergoing VT maintenance post induction but treatment discontinuation was similar and even less frequent in the once weekly bortezomib cohort, highlighting the importance of considering the frequency of bortezomib administration in the treatment regimen. The trial provided the rationale for considering VMPT in elderly, transplant ineligible patients given the better tolerability of bortezomib with once a week infusion than the usual twice weekly dosage (16% vs. 3%).
Another combination approach 91 examining sequential drug combinations has been tested using 3 cycles of VCD followed by another three of VTD as induction regimen with the goal of reducing toxicity related to prolonged drug exposure. Of the 42 evaluable patients ≥ 36% nCR, 19% sCR, and ≥57% VGPR were noted with an ORR of 95%. More importantly 82% patients completed all treatment cycles and no deaths related to treatment noted, highlighting the potential for larger trials in the future designed to test this regimen in larger randomized cohorts.
Varying degrees of bone involvement, from generalized osteopenia to lytic lesions and pathological-fractures, are a hallmark of the disease and affect a significant proportion of patients. Clinical trials have shown reduced frequency of skeletal events with bisphosphonate therapy and a recent randomized trial also demonstrated improved overall survival in the context of zoledronic acid therapy. Bortezomib treatment anabolically stimulates bone formation as indicated by the elevated levels of bone specific alkaline phosphatase and osteocalcin, results which are further complimented by radiologic evidence of improved bone structure in the same patients.92,93 Bortezomib is likely to add to the bone strengthening effect of the bisphosphonates directly by its effect on bone cells and indirectly through the disease control achieved with its use. 94
Conclusion
Bortezomib has come a long way since its development as one of the most effective drugs currently available for treating Multiple Myeloma. With improved efficacy of combination regimens we have seen increasing usage of its therapeutic spectrum ranging from frontline induction to maintenance therapy. Bortezomib has been integrated into the treatment of myeloma at every disease stage. In the context of newly diagnosed disease, bortezomib has been combined with other drugs as induction regimens in both transplant eligible and ineligible patients. The most common regimens in use include the VCD, VTD, VRD, and MPV regimens. Bortezomib has been used as part of the conditioning regimens in clinical trials and the results certainly encourage future larger trials to ascertain benefit. Bortezomib as part of consolidation post-transplant, or as a maintenance agent both in the transplant and non-transplant setting, continues to be examined with the goal of inducing deeper responses, which can potentially translate to longer PFS and possibly OS. However, maintenance requires an understanding of drug action and the possible side effect profile on long-term basis, 95 as elucidated by an increased risk of secondary malignancies reported with lenalidomide maintenance.96,97 Bortezomib has been shown to have a specific role in certain clinical situations. Based on several studies, it is clear that the drug should be part of any treatment regimen in the high-risk population and needs to be given for an extended period of time. The lack of renal excretion makes it an invaluable part of any regimen in patients presenting with renalin sufficiency. In the relapsed setting, bortezomib can be reused in combination with other myeloma drugs as well as with other experimental agents in clinical trials. Finally, the use of the subcutaneous administration and once weekly schedule has significantly decreased the neurological toxicity allowing for its extended use.
Author Contributions
Analysed the data: UP, SKK. Wrote the first draft of the manuscript: UP. Contributed to the writing of the manuscript: SKK. Agree with manuscript results and conclusions: UP, SKK. Jointly developed the structure and arguments for the paper: UP, SKK. Made critical revisions and approved final version: UP, SKK. All authors reviewed and approved of the final manuscript.
Funding
Author(s) disclose no funding sources.
Competing Interests
Author(s) disclose no potential conflicts of interest.
Disclosures and Ethics
As a requirement of publication author(s) have provided to the publisher signed confirmation of compliance with legal and ethical obligations including but not limited to the following: authorship and contributorship, conflicts of interest, privacy and confidentiality and (where applicable) protection of human and animal research subjects. The authors have read and confirmed their agreement with the ICMJE authorship and conflict of interest criteria. The authors have also confirmed that this article is unique and not under consideration or published in any other publication, and that they have permission from rights holders to reproduce any copyrighted material. Any disclosures are made in this section. The external blind peer reviewers report no conflicts of interest. Provenance: the authors were invited to submit this paper.