
Abstract
Primary central nervous system lymphoma (PCNSL) constitutes a rare group of extranodal non-Hodgkin's lymphoma (NHL) primarily of B cell origin. It occurs in both immuno-competent and immune-compromised patients. High dose methotrexate (HD-MTX) based chemotherapy is the standard therapy. Chemotherapy with whole brain radiation therapy (WBRT) improves response rates and survival compared with WBRT alone. However, due to the increased risk for neurotoxicity with WBRT, recent studies have focused on using chemotherapy alone. Methotrexate based multi-agent chemotherapy without WBRT is associated with similar treatment rates and survival compared with regimens that include WBRT although controlled trials have not been performed. Because of the low incidence of this disease, it is difficult to conduct randomized controlled trials. In this article we have discussed about the past, present and emerging treatment options in patients with PCNSL.
Keywords
Primary central nervous system lymphoma (PCNSL) is an aggressive, rare extra-nodal non-Hodgkin's lymphoma (NHL) that involves the brain, spinal cord, meninges and eyes. It occurs in both immunocompetent and immunocompromised patients. Median age at diagnosis is between 60–65 years. It represents about 4% of all primary intracranial neoplasms. Contrast-enhanced cranial magnetic resonance imaging (MRI) is the best imaging modality for assessment. Surgical resection should be limited to patients with impending herniation and ventricular dilatation. The most common presenting symptoms include focal neurologic deficits, signs and symptoms of increased intracranial pressure, personality changes, seizures and ocular symptoms.
PCNSL is classified as stage IE by Ann Arbor classification. The important components of staging are to exclude concomitant systemic disease and ocular involvement. Testicular ultrasound is recommended in elderly patients to exclude testicular lymphoma. Cerebrospinal fluid analysis (CSF) should be done in all patients and should be sent for cell count, protein, glucose, cytology, flow cytometry and PCR. HIV testing is suggested in all patients. Bone marrow aspirate and biopsy is recommended in all patients. Currently there is no role for (fluorodeoxyglucose-positron emission tomography) scan in patients with PCNSL.
Most of the clinical trials use the International Extranodal Lymphoma Study Group (IELSG) prognostic scoring system which uses age, performance status, serum lactate dehydrogenase level, cerebrospinal fluid protein concentration, and the involvement of deep structures as the risk stratifying factors. 1 The prognostic scoring system developed by the Memorial Sloan Kettering Cancer Center uses age and performance status as risk stratifying factors and it has been validated in the RTOG PCNSL clinical trials. 2 To ensure similarity and increase the communication among the investigators conducting the clinical trials for newly diagnosed patients with PCNSL, an international group of experts representing hematologic oncology, medical oncology, neuro-oncology, neurology, radiation oncology, neurosurgery, and ophthalmology met to review current standards and devised a consensus opinion regarding minimum baseline evaluation and response assessment. 3
Pathogenesis
The most common histopathologic subtype is diffuse large B-cell lymphoma (DLBCL) seen in about 90% of patients. Rarely, PCNSL may present like Burkitt lymphoma, marginal zone lymphoma, lymphoblastic lymphoma, small lymphocytic lymphoma or Hodgkin Lymphoma. T cell lymphomas compose about 2% of PCNSL in western countries and about 8% in Japan. The exact pathogenesis of PCNSL is still unclear in immunocompetent patients. Epstein-Barr virus plays a role in the pathogenesis in immunocompromised patients. However, recent evidence suggests that Primary CNS DLBCL is derived from peripheral B cells activated by antigenic stimulation and enter the brain through connections between various extracellular matrix and adhesion molecules. 4 Thompsett et al have also demonstrated a high frequency of somatic hypermutation pattern suggesting the role of antigenic stimulation. 5 Sasayama et al measured the cerebrospinal fluid (CSF) levels of IL-10 and IL-6 in 66 patients with intracranial tumors and found the median CSF levels of IL-10 and IL-6 were 27 pg/mL and 5.4 pg/mL, respectively in patients with PCNSL. The levels were significantly higher in PCNSLs than in the other brain tumors. The sensitivity and specificity of 71.0% and 100% respectively was found with an IL-10 cut off level of 9.5 pg/mL. The CSF IL-10 level might be a useful diagnostic and prognostic biomarker in patients with PCNSLs. 6 Del (6) (q22) was found to be associated with decreased overall survival and is present in about 50% of patients. 7 Rubenstein et al has shown that high expression of STAT6 was associated with a shorter survival in patients treated with high-dose intravenous methotrexate and have also identified several IL-4 induced genes in patients with PCNSL. 8
BCL-6 is frequently expressed in PCNSL, but the data is conflicting on its prognostic value. Braaten et al have shown that BCL-6 expression was associated with favorable prognosis, 9 while Chang et al showed a trend towards poor prognosis. 10 Similarly, Song et al has shown that BCL-6 expression was associated with higher PFS and OS in patients having non-deep-site involvement in the brain. 11 It had no prognostic value in patients who had deep-site involvement.
Camilleri-Broet et al evaluated 83 cases of PCNSL and found that the majority had a phenotype indicative of the activated B-cell type. 12 This is in contrast to earlier studies that suggested a germinal center B-cell type derivation.13,14 In their study they have aslo reported that BCL-6 expression had no effect on the outcome of patients with PCNSL. Baraniskin et al have demonstrated that CSF micro RNA's could be a useful tool for the diagnosis of PCNSL. 15 Among the micro RNA's miR-21, miR-19 and miR-92a were found to be diagnostic. Kim et al failed to demonstrate the prognostic relevance of hypoxia associated protein in PCNSL. 16 Sung et al have recently published their study combining genomic profiling with gene expression profiling and identified novel tumor suppressor genes and pathways specific to PCNSL (JAK-STAT, NF-kB pathway, Notch signaling pathway) which might serve as potential therapeutic targets of PCNSL. 17
Pharmacokinetics
The blood brain barrier (BBB) is the limiting factor in delivering biologically active agents to the central nervous system (CNS). Certain physical properties like low molecular weight, lipophilicity and lack of ionization are important to reach the CNS. The concept of the blood-brain barrier (BBB) was first introduced by Paul Ehrlich more than 100 years ago. ABBB is present in 99% of the brain capillaries. There are multiple variables which determine the capability of drugs to cross the BBB, such as size, hydrophilia and ionization.
There are three major subgroups of drugs which differ according to their ability to cross the BBB and adequately treat PCNSL. First, there is a group of drugs with a very low ability to cross the BBB that can be administered at remarkably higher doses to obtain therapeutic concentrations in the tumor tissue and lymphoma-surrounding neural tissue. This is the case with methotrexate (MTX) and cytarabine. Second, there is a group of drugs with a very low capability to cross the BBB and which cannot be administered at high doses because of dose-limiting toxicity. This is the case with anthracyclines, vinca alkaloids and some alkylating agents, which represent the mainstay of treatment of systemic Non-Hodgkin lymphoma (NHL) but exhibit negligible activity in PCNSL. Third, there are some chemotherapeutic agents able to cross the BBB and reach therapeutic concentrations in the tumor bed. This is the case with thiotepa, ifosfamide, temozolomide and nitrosoureas which are frequently included in chemotherapy combinations for PCNSL.
The efficacy of MTX depends on the duration of infusion and drug concentration. The optimal administration schedule is still not clear. While standard dose MTX does not cross the BBB, doses at 1–3 g/m2 result in tumoricidal levels in the brain parenchyma and doses >3 g/m2 yield tumoricidal levels in the CSF. A significantly higher response rate and CSF levels have been obtained administering HD-MTX in a 3 hour infusion. 18 Methotrexate area under the curve AUCHD-MTX has been found to be the most most independent predictor of clinical outcome in the analysis done by Joerger et al on the patients enrolled in IELSG 20 trial. 19 This was also previously reported by Ferreri et al 2004. 20 Hence, personalized dosing of MTX should be used based on patients age, gender and creatinine clearance to improve the outcome. Various drug delivery mechanisms have been proposed to overcome the BBB. Intra-arterial delivery has the advantage of increased concentration of the drug in the CNS with less systemic exposure. Intrathecal or intraventricular delivery produces the most consistent CSF levels.
Treatment
Radiotherapy
For many years whole brain radiation therapy (WBRT) was the standard treatment for PCNSL patients resulting in a median survival of 10–18 months and a 5 year overall survival of 10 to 20% with very high relapse rates. 21 Partial brain irradiation was associated with reduced survival rates and high recurrence rates. 22 With the addition of multidrug regimens the role of WBRT seems to be decreasing. Using high dose WBRT with 40 Gy followed by boost to the tumor bed of 20 Gy showed no increase in overall survival as reported by the Radiation Therapy Oncology Group RTOG 83–15 trial. 23 WBRT alone as a treatment remains an option for elderly patients with multiple comorbidities or patients with poor performance status who cannot tolerate chemotherapy. To optimize the treatment outcome of patients with PCNSL studies were done using combined modality therapy.
Chemoradiation Therapy
HD-MTX based treatment showed good response in patients with systemic lymphoma who had CNS relapse. This led to the use of this drug in PCNSL patients. Since the incidence of this tumor is very low it was difficult to conduct adequately powered randomized phase III clinical trials. 24 Studies have shown that combined modality therapy (CMT) has produced response rates up to 80–90% and median overall survival up to 5 years (Table 1)25–35 but, this came with a major limitation of neurocognitive toxicity especially in patients older than 60 years of age. There is still a debate as to whether WBRT in combination with chemotherapy improves any survival.
Combined modality therapy in patients with newly diagnosed primary CNS lymphoma.
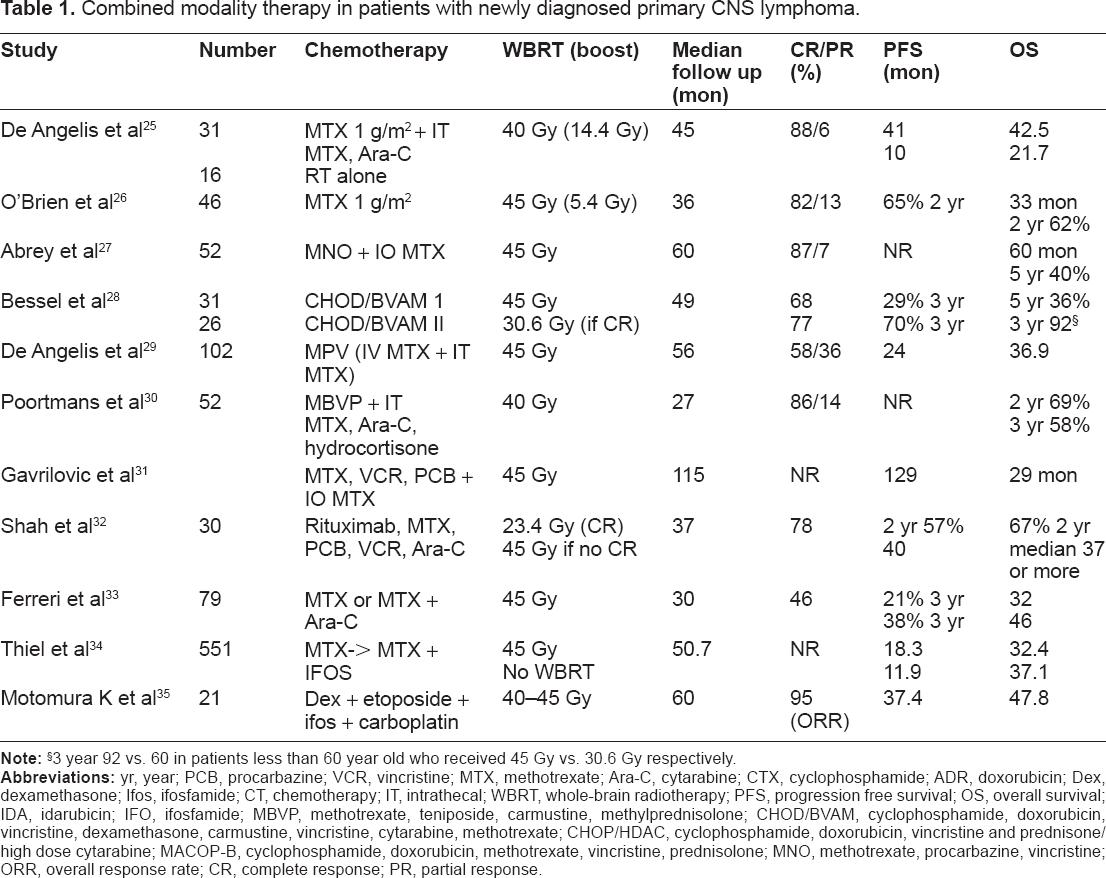
3 year 92 vs. 60 in patients less than 60 year old who received 45 Gy vs. 30.6 Gy respectively.
A randomized study comparing CHOP (cyclophosphamide, doxorubicin, vincristine and prednisone) to CHOP plus radiotherapy conducted by the Medical Research Council was stopped because of poor accrual and showed only minimal effectiveness. 36 It could be because of the poor penetration of CHOP through the BBB achieving sub-therapeutic levels in the CSF.
Deangelis et al reported an improved survival of 41 months for 31 patients treated with combined modality therapy consisting of pre-irradiation systemic MTX and intrathecal (IT) MTX with WBRT 40 Gy plus boost (14.4 Gy) followed by high dose Ara-C compared to a control group treated with RT alone (median survival 10 months). 25 This was not a randomized study and it did not reach statistical significance for overall survival (OS) because of the small number of patients. The exact dosing of RT and the role of boost remains undefined.
Shah et al has shown that reducing the dose of WBRT after achieving CR with induction chemotherapy had no impact on outcome, 32 which was contrary to data presented by Bessell et al who demonstrated that reduced dose of WBRT compromised survival in younger patients. 28
Ferreri et al has shown that WBRT dose reduction to 30 Gy in patients with CR after chemotherapy was associated with similar outcomes compared to those receiving higher radiation doses with reduced neurotoxicity. 37
A randomized phase 2 study IELSG 20, included 79 patients assigned to either MTX 3.5 g/m2 alone or combined with Ara-C followed by WBRT in both arms. 33 Patients assigned to the Ara-C arm had an improved response (CR 46% vs. 18%) and survival rates (3 year OS:46% vs. 32%) compared with HD-MTX alone. Most experts in the field think that MTX-Ara-C combination is the current standard approach for newly diagnosed PCNSL patients as it is supported by the highest level of evidence.
The combination of high doses of methotrexate (MTX) and cytarabine (Ara-C) is the standard chemotherapy for patients with primary CNS lymphoma (PCNSL). Ferreri et al conducted a pilot study to assess the efficacy of adding an alkylating agent (thiotepa) to the regimen of MTX + Ara-C (MAT). To minimize toxicity the dose of Ara-C was halved. 2-year OS of 24% ± 9% was noted. MAT and MTX-Ara-C combinations showed similar tolerability, whereas Ara-C dose reduction was associated with a remarkably lower efficacy, masking any potential benefit of thiotepa. 38 Thus the authors have concluded that treatment with full dose of Ara-C 2 g/m2 is important in patients with PCNSL.
A recently published randomized trial G-PCNSL-SG-1 has shown that there was no difference in overall survival when radiotherapy was omitted although progression free survival (PFS) was longer in patients who received WBRT (18.3 months vs. 11.9 months). 34 This study had major protocol violations and flaws however.
The dose of WBRT in patients with CR after radiotherapy remains undefined. It needs to be addressed in prospective trials. Combined modality treatment prolongs survival compared with WBRT alone and remains the mainstay of treatment. Comparing treatments can be difficult because of usage of different chemo regimens, different radiation doses and salvage therapies. To avoid the neurotoxicity, clinical trials have focused on intensifying chemotherapy by using poly-chemotherapy or giving high dose chemotherapy followed by autologous stem cell transplantation. (HDC/ASCT).
Chemotherapy Alone
To avoid the late neurologic complications arising from radiation therapy studies have focused on using chemotherapy alone in patients with PCNSL (Table 2).39–51
Chemotherapy alone in patients with newly diagnosed PCNSL.

TTF, time to treatment failure.
Single agent methotrexate has been tested in phase II studies. The study reported by Batchelor et al using HD-MTX at 8 gm/m2 showed an objective response rate of 74% with progression free survival of 12.8 months and median overall survival (OS) was not reached at 22.8 months. 45 An update on this study showed a median survival of 55 months. 52 Elderly patients also tolerated the regimen well although most of them required dose reductions due to impaired creatinine clearance. High dose methotrexate alone as initial treatment is still controversial.
Guha-Thakurta et al reported their results on induction chemotherapy MTX 8 g/m2 followed by maintenance therapy at 3.5 g/m2 at 3 month intervals. 41 Median PFS was 17 months and the median OS was 30 months with an objective response rate (ORR) of 100% with a 65% CR rate. The regimen was well tolerated with preservation of cognitive and memory skills. The baseline Karnofsky performance score (KPS) (median 40) was very low demonstrating a significant benefit of this approach in severly ill patients. Two subsequent studies failed to produce similar results however.42,45 Although MTX as a single agent has better side effect profile, to improve the outcome it may be necessary to add other agents.
A phase II study conducted by the EORTC group in elderly patients with PCNSL reported a median survival of 14.3 months and 1 year PFS of 40% when using a regimen that consisted of high-dose methotrexate, lomustine, procarbazine, methylprednisolone, IT chemotherapy with MTX and cytarabine. 43 Most patients preserved their cognitive function and KPS, with myelosuppression being the most frequent side effect. In this patient population, chemotherapy alone produced comparable results with WBRT and without any significant cognitive toxicity.
Pels et al conducted a pilot study using high dose MTX and cytarabine based therapy including dexamethasone, vinca alkaloids, ifosfamide, cyclophosphamide with intraventricular MTX, prednisolone and Ara-C. 44 The median overall survival was 50 months and median time to treatment failure was 21 months. For patients older than 60 years median survival was 34 months. Permanent cognitive dysfunction occurred in only 3% of patients. Response rates and duration were comparable to the results reported after combined chemo-radiotherapy.
A phase II study by Chamberlain et al reported their data on chemotherapy alone in patients with newly diagnosed PCNSL. 48 Their regimen included HD-MTX and rituximab with deferred WBRT. Median OS was 29 months with median PFS of 21 months. About 40% of patients were greater than 70 years old.
Temozolomide as upfront therapy tested in elderly patients is associated with a median survival of 21 months with 47% CR rate. 49 In this study 5 of 17 patients (29.4%) had prolonged responses for at least 12 months and overall survival of more than 24 months. Of these five patients three had a methylated O6-methylguanine-DNA methyltransferase (MGMT) promoter. Temozolomide alone remains an option in frail elderly patients who otherwise cannot receive HD-MTX based treatment.
A phase 2 study done by the CALGB (Cancer and Leukemia Group B) reported a 3 year PFS of 50% and OS of 67% using a combination of HD-MTX, temozolomide, and rituximab followed by consolidation with HD-Ara-C and HD etoposide without WBRT. 53
Intra-Arterial Chemotherapy with Blood Brain Barrier Disruption (BBBD)
The major challenge in PCNSL is to deliver therapeutic concentrations of drugs to the CNS. The safety and efficacy of intra-arterial chemotherapy in conjunction with blood-brain barrier disruption has been documented in few studies.39,54 The opening of tight junctions with osmotic disruption with mannitol allows increased levels of drugs up to 50 to 100 fold. Angelov et al reported their data on intra-arterial chemotherapy with BBB disruption suggesting a CR rate of 58% with 5 year progression free survival of 31%. 47 Tyson et al reported a retrospective study on patients with relapsed PCNSL treated with second line intra-arterial carboplatin-based chemotherapy plus BBBD. 55 The protocol was repeated every 4 weeks for up to 1 year. Overall response rate was 35% with a median survival of 6.8 months. Six patients were alive at 42.8, 50.4, 50.9, 54.7 and 91 months from first carboplatin/BBBD treatment. The potential advantages of this approach are achieving prolonged durable remissions without any neurocognitive sequelae associated with WBRT. The disadvantages include requiring general anesthesia with an increase incidence of stroke, thrombosis and seizures and this can be only done in major centers with expertise. IA chemotherapy with BBB disruption is being tested in multicenter trials.
Intrathecal Chemotherapy (IT)
Leptomeningeal involvement in PCNSL occurs in about 37% of patients. 25 The concentration of MTX between plasma and CSF is approximately 100:1 when given intravenously. 56 The serum half-life of MTX after a 24-hour infusion is 2 to 4 hours depending on the dose, while intraventricular administration produces a CSF half-life of up to 48 hours.57,58,59 The role of IT chemotherapy is not clear. CSF acts as a sanctuary for PCNSL tumor cells leading to increased risk of relapses. Large retrospective studies have not shown any benefit with the addition of IT chemotherapy in patients treated with high dose MTX.60,61 Pels et al reported their data on 65 patients with PCNSL who were treated with MTX-Ara-C based therapy combined with intraventricular MTX, Ara-C and steroids. Median PFS was 21 months, with 57% of young patients being alive at a median follow up of 100 months. 44 In a second trial conducted by the same author patients received the same chemotherapy without intra-ventricular drug delivery. 62 Although the response rates were similar, more than half of the patients relapsed within the first year leading to the premature termination of the trial. A phase 1 study conducted by Rubenstein et al has shown some activity of intraventricular rituximab. 63 Currently guidelines do not recommend intrathecal/intraventricular chemotherapy to be included in the treatment regimen, although many physicians recommend in patients with positive CSF cytology.
High Dose Chemotherapy with Autologous Stem Cell Transplantation (HDC/ASCT)
Current knowledge in PCNSL management results from a limited number of single-arm phase II trials, meta-analyses and large retrospective series. HDC/ASCT has been tested as salvage treatment in patients with recurrent or refractory PCNSL, and as consolidation after primary chemotherapy, replacing or preceding whole-brain irradiation (Tables 3 and 4).64–72 The rationale for the use of HDC/ASCT is to administer intensive doses of chemotherapy to overcome drug resistance and to achieve therapeutic concentrations in the lymphoma tissue and other sanctuaries, like cerebrospinal fluid (CSF), meninges and eyes. The results have been variable when used as first line therapy for newly diagnosed patients. 73 The results are not consistent among the trials because of usage of different induction regimens, consolidation treatment and the use of WBRT. Among induction regimens MTX based polychemotherapy was more effective. Among consolidation regimens BEAM (carmustine, etoposide, cytarabine, and melphalan) regimen was ineffective although it is a standard regimen for other aggressive lymphomas. Thiotepa based regimens were more effective. The discrepancies could be related to different CNS penetration of the drugs. Busulfan, carmustine and thiotepa exhibit good CNS penetration with CSF levels exceeding 50%–80% of serum levels, while drugs in the BEAM regimen have poor CNS penetration rates of 5%–22%. 74
High dose chemotherapy followed by autologous stem cell transplantation in patients with newly diagnosed PCNSL.
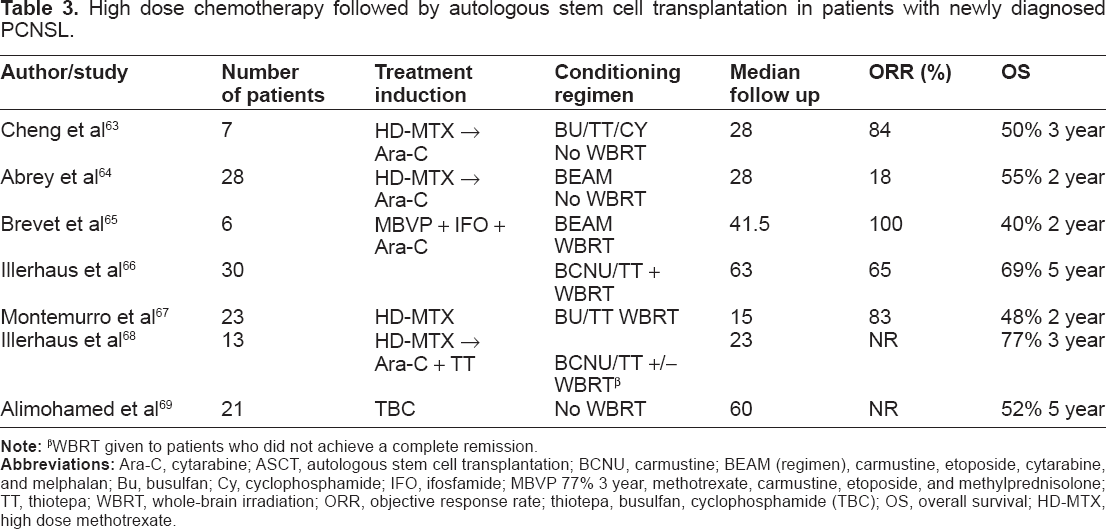
WBRT given to patients who did not achieve a complete remission.
High dose chemotherapy followed by autologous stem cell transplantation in patients with relapsed and refractory PCNSL.

Abrey et al treated 28 patients with an induction regimen consisting of MTX 3.5 g/m2 and Ara-C 3 g/m2 followed by conditioning which included BEAM therapy. 64 Only 57% achieved CR. Median time to progression after transplant was 9.3 months. Since the response rates were poor with this therapy subsequent trials have focused on intensifying therapy and using different conditioning regimen.
Cheng et al also reported their data using high dose MTX based regimen for induction followed by thiotepa, busulfan, and cyclophosphamide. 63 In patients with poor prognostic factors six of seven achieved CR.
Illerhaus et al reported their data using a regimen that included 3 cycles of HD-MTX 8 g/m2, Ara-C, and thiotepa. 66 Patients received carmustine and thiotepa before transplant. WBRT of 45 Gy was given to patients who had CR and 50 Gy to those who had a partial response. 15/30 patients had a CR with induction therapy and an additional six achieved CR after WBRT. The 5 year survival was 69% in this study. The same group reported their data in a small phase 2 study suggesting that HDC/ASCT could replace WBRT as a consolidation treatment by achieving a 3 year survival of 77% (2008) with no neurotoxicity. 68 Comparison is difficult since the two studies were done in different settings.
Soussain et al reported the results of a prospective multicenter trial of intensive chemotherapy followed by autologous hematopoietic stem-cell rescue in patients with PCNSL who failed HD-MTX-based treatment.70,71 The treatment consisted of 2 cycles of HD cytarabine and etoposide (CYVE) and the conditioning regimen was thiotepa, busulfan and cyclophosphamide. About 15 out of 20 patients with chemo-sensitive disease and 12 non-responders underwent HDC/ASCT.
The median PFS was 11.6 months and the median OS was 18.3 months in the overall population and 41.1 months and 58.6 months among patients who completed intensive chemotherapy followed by autologous hematopoietic stem-cell rescue, respectively. Intensive chemotherapy followed by autologous hematopoietic stem-cell rescue remains an effective treatment option in patients with recurrent or refractory PCNSL but remains an option as part of first line therapy. The two ongoing randomized trials (NCT01011920; NCT00863460) will establish the most effective way to consolidate therapy either with WBRT or HDC/ASCT.
Salvage Therapy
About 30%–60% of patients with PCNSL eventually relapse. Treatment options for these patients are limited and the prognosis is poor. The reported median survival of these patients is only 2 months if left untreated and with treatment the median survival goes up to 14 months (Table 5).54,62,75–86
Salvage treatment in patients with relapsed/refractory primary CNS lymphoma.

1 year survival.
When chemotherapy is used as first line treatment WBRT can be used as salvage treatment. Hottinger et al conducted a retrospective study to evaluate the safety and efficacy of salvage WBRT. 79 Median survival was 16 months with 1 year survival of 54%.
Similarly Nguyen et al reported their data on WBRT as salvage therapy for PCNSL. The median dose of WBRT was 36 Gy. 77 37% achieved a CR rate. Median survival was 10.9 months and median PFS was 9.7 months. Khimani et al have reported an overall survival of 11.7 months with a CR of 50% with salvage WBRT in patients with primary or secondary CNSL. 83 The median survival after salvage WBRT is comparable to the treatment with WBRT given as a first line treatment.
HD-MTX remains an option for patients with relapsed PCNSL who initially responded to HD-MTX. Plotkin et al performed a multicenter, retrospective study of high-dose methotrexate in patients with relapsed PCNSL. 75 Overall response rate was 91% to first salvage and 100% to second salvage. The reported median survival was 62 months. The most common toxicity observed was mainly hematologic.
Reni et al reported their phase II trial assessing temozolomide in recurrent PCNSL patients previously treated with HD-MTX chemotherapy and/or radiotherapy. 80 A response rate of 31% was observed with a median PFS of 2.8 months and median overall survival of 3.9 months.
Makino et al evaluated the methylation status of MGMT gene promoter region in patients with or relapsed refractory PCNSL. The primary treatment was HD-MTX (3.5 g/m2) with or without irradiation. Patients were treated with temozolomide 150–200 mg/m2, for 5 days every 28 days.
There were five complete remissions with five partial responses (PRs). Median overall survival was 6.7 months. MGMT promoter methylation was found in 4 (36.4%). Median overall survival was not significantly different between patients with methylated MGMT (11.1 months) and non-methylated MGMT (6.7 months). 85
Enting et al reported their retrospective data using a combination of Temozolomide plus Rituximab. 76 Rituximab (750 mg/m2) was given on days 1, 8, 15 and 22, and Temozolomide (100–200 mg/m2) on days 1–7 and 15–21. Median PFS for responding patients was 7.7 months with a median survival of 14 months. The toxicity was minimal. This combination might be an option in elderly patients.
Topotecan, is a topoisomerase I inhibitor which can cross the BBB and reach therapeutic concentrations in the CSF. Fischer et al reported the results of a prospective study on Topotecan in relapsed or refractory PCNSL. 78 The overall response rate was 33%, with 5 CRs and 4 PRs. The median PFS was 2 months (9.1 months in responders). The overall survival was 8.4 months with 1-year survival of 39%. Additional radiation therapy after topotecan treatment resulted in a longer survival time in the resistant patient group. Grade 3/4 leucopenia or thrombocytopenia occurred in 26% and 11% of the patients, respectively.
Similarly, Voloschin et al reported a Phase II study that included 15 refractory or relapsed PCNSL patients with a median age of 56 years. 82 The treatment consisted of intravenous topotecan for 5 consecutive days every 3 weeks. Three patients achieved CR with a median PFS of 2 months.
Eleven of the 15 patients had grade 3/4 neutropenia and 3 patients had grade 3 thrombocytopenia. Topotecan is active in relapsed and refractory PCNSL but hematologic toxicity remains a major concern especially in elderly patients.
Rituximab is a chimeric monoclonal antibody against the CD-20 antigen with a molecular weight of 145 kDa. Rituximab achieves a CSF concentration of only 0.1% of serum levels after intravenous infusion. A Phase 1study conducted by Rubenstein et al consisted of intrathecal rituximab thru Ommaya reservoir. 62 Median survival reported was about 5.2 months. Rituximab is being tested in combination with other chemotherapy. 90Y-ibritumomab tiuxetan is a murine anti-CD20 linked to the Yttrium-90 by the chelator tiuxetan. Iwamoto et al reported their data on 6 patients using 90Y-ibritumomab. 81 Median overall survival reported was only 1.6 months.
Tyson et al reported a retrospective study on patients with relapsed PCNSL treated with second line IA carboplatin-based chemotherapy plus BBBD. 54 Overall response rate was 35% with a median survival of 6.8 months. However, a CTC grade 3/4 hematological adverse event was seen in 41% of the patients. Ototoxicity was reported in 3% of the patients probably due to carboplatin.
Poly-chemotherapy was also tested in patients with relapsed or refractory PCNSL.
Arellano-Rodrigo et al reported a retrospective study of 16 patients with refractory and recurrent PCNSL. 74 The first line treatment used in all these patients was cyclophosphamide, doxorubicin, vincristine, dexamethasone/carmustine, vincristine, cytarabine and methotrexate (CHOD/BVAM) and radiotherapy, followed by VP16, ifosfamide and Ara-C (VIA) chemotherapy as a salvage treatment. Six patients (37%) achieved CR with a median PFS of 5 months and 1-year overall survival of 41%. The major toxicity was hematologic. VIA chemotherapy remains an option in patients with refractory/recurrent PCNSL.
A case report submitted by Renfrow et al has shown that there might be a role of Bendamustine in the treatment of relapsed PCNSL patients. The pharmacokinetics and efficacy needs to be further tested in larger trials. 86
Raizer et al have recently published their data on relapsed and refractory patients with PCNSL. Pemetrexed at 900 mg/m2 was given to 11 patients. Median PFS of 5.7 months and an OS of 10.1 months was observed. Mainly hematologic and infectious toxicity was noted. The optimal dosing and efficacy needs further investigation. 84
Conclusion
In the past few years considerable progress has been made in the treatment of PCNSL. It is difficult to conduct randomized prospective trials because of the low incidence of this disease. The ongoing randomized trials might provide some insight into the new treatment combinations, the most effective consolidation treatment with improved efficacy and less toxicity. To achieve this, international multicenter trials should be conducted. Every patient should be enrolled in a clinical trial if eligible. There are many unanswered questions at this time as to the best initial treatment in younger and older patients, in whom WBRT could be omitted without compromising survival, the role of intrathecal chemotherapy and the setting of HDC/ASCT. Recently published data suggests a role of certain pathways like JAK-STAT, NF-kB, NOTCH signaling which could serve as potential targets of therapy. HD-MTX based combination chemotherapy with or without WBRT remains the primary treatment of choice in patients with PCNSL at the present time.
Author Contributions
Conceived and designed the experiments: PP, PB. Analysed the data: N/A. Wrote the first draft of the manuscript: PP. Contributed to the writing of the manuscript: PP, PB. Agree with manuscript results and conclusions: PB. Jointly developed the structure and arguments for the paper: PP, PB. Made critical revisions and approved final version: PB. All authors reviewed and approved of the final manuscript.
Disclosures and Ethics
As a requirement of publication author(s) have provided to the publisher signed confirmation of compliance with legal and ethical obligations including but not limited to the following: authorship and contributorship, conflicts of interest, privacy and confidentiality and (where applicable) protection of human and animal research subjects. The authors have read and confirmed their agreement with the ICMJE authorship and conflict of interest criteria. The authors have also confirmed that this article is unique and not under consideration or published in any other publication, and that they have permission from rights holders to reproduce any copyrighted material. Any disclosures are made in this section. The external blind peer reviewers report no conflicts of interest. Provenance: the authors were invited to submit this paper.