
Abstract
Background:
Blastic plasmacytoid dendritic cell neoplasm (BPDCN) is a rare and aggressive hematological cancer. Due to its low incidence, researchers struggle to gather sufficient prospective data to inform clinical treatment.
Objectives:
We sought to summarize the clinical characteristics and current treatment methods of BPDCN and provide more specific guidance on treatment options.
Design:
A systematic literature review using data from 74 Chinese BPDCN patients.
Date resources and methods:
We retrospectively analyzed the clinical manifestations, treatment response, survival outcomes, and prognostic factors of six BPDCN patients treated at the First Affiliated Hospital of Zhengzhou University and 68 patients described in 28 articles published in the China Knowledge Network database since 2019.
Results:
In Chinese patients, the disease occurred with a male-to-female ratio of 2.52 and a median age of onset of 50 years in adults and 10 years in pediatric patients. Immunohistochemical analysis revealed distinctive immune phenotypes of BPDCN cells, characterized by high expression levels of CD4, CD56, CD123, and HLA-DR, while showing minimal to no expression of myeloperoxidase (MPO), CD20, and CD79a. There was no significant difference in the initial complete remission (CR) rate, relapse rate, and the overall survival (OS) time of patients receiving acute myeloid leukemia-like, acute lymphocytic leukemia-like, or non-Hodgkin’s lymphoma-like chemotherapy regimens. Univariate analysis identified CD3 expression, male gender, and central nervous system infiltration as hazardous factors. In multivariate analysis, age proved to be an independent prognostic indicator, indicating better prognosis and longer OS time in younger patients. Notably, hematopoietic stem cell transplantation (HSCT) emerged as a significant factor in improving the survival outcomes for individuals diagnosed with BPDCN. However, further investigation is needed to explore the role of HSCT and the best timing for its implementation in pediatric BPDCN patients.
Conclusion:
Administering HSCT during the initial CR state following inductive chemotherapy might extend the OS and improve the prognosis of patients with BPDCN.
Plain language summary
Blastic plasmacytoid dendritic cell neoplasm (BPDCN) is a rare, aggressive neoplasm that derives from the precursors of plasmacytoid dendritic cell (pDC), accounting for 0.44% of hematological malignancy. Although CD123 targeted therapy has been implemented in the treatment of BPDCN, but a unique complication, capillary leak syndrome presents a therapeutic challenge, and retrospective analysis of conventional chemotherapy regimens is of irreplaceable importance for patients cannot tolerate CD123 targeted therapy. For the first time, we conduced retrospective analysis of large-scale clinical cases based on Chinese patients, and found that age and hematopoietic stem cell transplantation (HSCT) were two independent prognostic factors of BPDCN. In conclusion, younger patients had longer overall survival (OS) time and better prognosis. Combining HSCT in the initial complete remission state significantly prolonged the OS time and improved survival outcomes of BPDCN patients.
Keywords
Introduction
Blastic plasmacytoid dendritic cell neoplasm (BPDCN) is a rare and aggressive neoplasm originating from the precursors of plasmacytoid dendritic cells (pDC) and accounting for approximately 0.44% of hematological malignancy. 1 Immunohistochemical analysis reveals that BPDCN cells exhibit a distinctive immune phenotype characterized by the expression of specific pDC markers, including CD4, CD56, CD123, BDCA-2/CD303, and TCL1 while lacking myeloid, T, B, and NK cell markers.2,3 Despite its rarity, BPDCN is associated with marked invasiveness and a high rate of recurrence, leading to a median overall survival (OS) time of 10–12 months and a 5-year survival rate of only 0.6%. 4 Currently, there is no standardized treatment approach for BPDCN. Common treatment modalities include local radiotherapy, systemic chemotherapy, hematopoietic stem cell transplantation (HSCT), and targeted therapy. 5 While BPDCN initially responds well to chemotherapy, most patients inevitably experience disease relapse and progression within a short timeframe, resulting in a median OS time of approximately 1 year. 6 Recent studies suggest that BPDCN patients receiving a combination of chemotherapy and HSCT may have improved survival outcomes. 7
So far, there is still a paucity of literature on Chinese BPDCN patients, with only a limited number of cases reported. To address this gap, we conduct a retrospective study leveraging our institutional clinical cases and data from the China National Knowledge Infrastructure (CNKI) database. This study was designed to elucidate the clinical and biological features of this rare disease among Chinese patients and offer valuable insights for guiding clinical management strategies.
Methods
Search strategy and selection criteria
Under the guidance of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) reporting guideline and Cochrane handbook (Supplemental File 1), 8 this study collected a total of six BPDCN patients treated at the First Affiliated Hospital of Zhengzhou University and 68 complete cases reported in 28 articles published on CNKI since 1 January 2019 (Table 1). All patients received a clear pathological diagnosis following WHO recommendations. The study’s search strategy, available in Supplemental File 2, considered articles that included BPDCN cases for inclusion. In cases where articles contained overlapping data, those with the most recent and detailed information were chosen for further analysis (Figure 1). The literature search and assessment of citation eligibility were conducted independently by two investigators (CG and YL). Disagreements were resolved through consensus with a third investigator (MZ).
Baseline characteristics of the included studies.

The detailed case resources and references were available in Supplemental File 3.

Flow diagram of the search results.
Treatment definitions
The initial chemotherapeutic regimens were categorized into four groups. The first group was acute myeloid leukemia (AML)-like, which included DA (doxorubicin, cytarabine), IA (idarubicin, cytarabine), and other regimens based on cytarabine. The second group was acute lymphocytic leukemia (ALL)-like, comprising DVLP (doxorubicin, vincristine, asparaginase, prednisone), hyper CVAD (hyperfractionated cyclophosphamide, vincristine, doxorubicin, dexamethasone), and regimens associated with ALL treatments. The third group was non-Hodgkin’s lymphoma (NHL)-like, including CHOP (cyclophosphamide, vincristine, doxorubicin, prednisone), COP (cyclophosphamide, vincristine, prednisone), DDGP (dexamethasone, cisplatin, gemcitabine, pegaspargase), and regimens associated with NHL treatments. The fourth group was not otherwise specified (NOS) regimens, which consisted of all other drugs alone or in combination. Additionally, we identified patients who received autologous or allogeneic HSCT (auto-HSCT and allo-HSCT, respectively).
Statistical analyses
Quantitative variables were presented as mean + standard deviation or median (range), while categorical variables were expressed as number and percentage. Overall response rates and relapse rates among responders were delineated using number, percentage, and 95% confidence intervals. The Student t test or Mann–Whitney U test was employed for comparing quantitative variables, while the x2 test or Fisher’s exact test was utilized for comparing categorical variables as appropriate. Kaplan–Meier methodology was applied to construct OS curves, with censored patients defined as individuals lost to follow-up. Univariate and multivariate Cox regression analyses were conducted to identify potential prognostic factors. Statistical significance was set at p < 0.05.
Results
Clinical characteristics
A total of 74 patients were analyzed, including 15 underage and 59 adult patients. Among adult patients with BPDCN, the disease tended to affect elderly males more notably as evidenced by a median onset age of 50 years (ranging from 19 to 97 years). In contrast, children with BPDCN typically manifested the disease earlier, with a median onset age of 10 years (ranging from 9 months to 18 years). This discrepancy in age of onset between adult males and children with BPDCN resulted in a notable male-to-female ratio of 2.52, as illustrated in Table 2. Out of 38 patients with available blood routine results, only three (7.9%) showed normal examination findings. Anemia was present in 59.5% of patients at the time of diagnosis, while 36.8% had leukopenia and 57.9% had thrombocytopenia. Additionally, 28.9% of patients had hyperleukocytosis, with 81.8% of them having white blood cell counts exceeding 20 × 109/L, reaching as high as 147 × 109/L (Table 2). Furthermore, 60 patients (81.1%) manifested cutaneous lesions, while 53 out of 62 patients (85.5%) demonstrated bone marrow infiltration (12 patients did not undergo bone marrow aspiration). The median proportion of abnormal cells in bone marrow flow cytometry was found to be 54.98% (ranging from 0.09% to 92.21%). Lymph node invasion was observed in 41 patients. In addition, cerebrospinal fluid aspiration was conducted on 38 patients, revealing central nervous system infiltration in nine patients (23.7%; Table 2).
Clinical and biological characteristics of the study population.
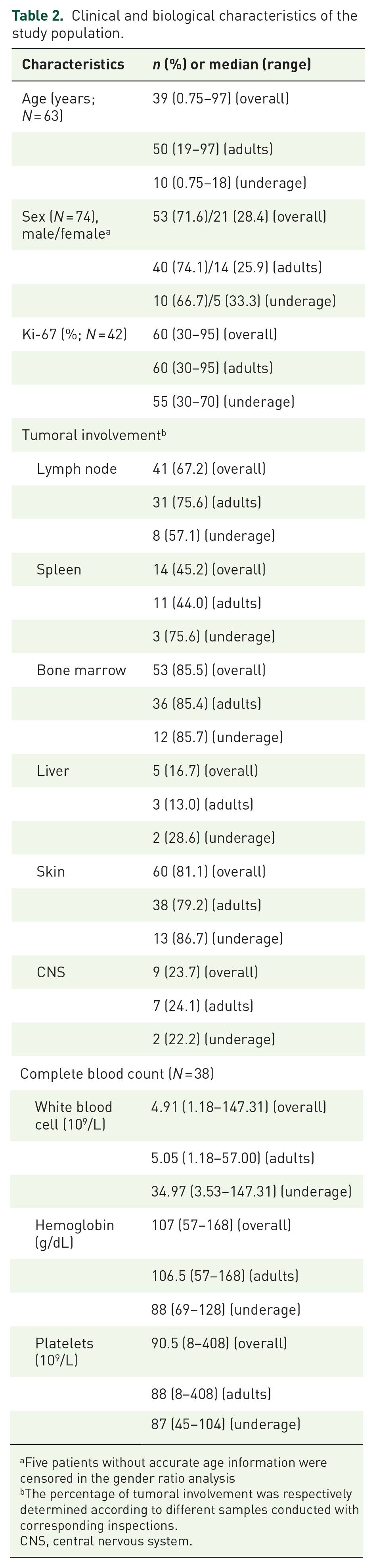
Five patients without accurate age information were censored in the gender ratio analysis
The percentage of tumoral involvement was respectively determined according to different samples conducted with corresponding inspections.
CNS, central nervous system.
Immunophenotype
The immune phenotypes of BPDCN cells, as shown in Table 3, were characterized by the high expression of CD4 (96.6%), CD56 (93.3%), CD123 (96.5%), and HLA-DR (100%) while exhibiting almost no expression of myeloperoxidase (MPO) (0%), CD20 (6.5%), and CD79a (3.8%). Furthermore, CD303 was expressed in 17 out of 20 patients (85.0%) and CD304 in 15 out of 16 patients (93.8%); in contrast, CD3 was expressed in only 6 out of 48 patients (12.5%), which was a crucial factor in the subsequent prognostic analysis. In 42 patients, the level of Ki-67 expression was available, with a median value of 60% (ranging from 30% to 95%), as outlined in Table 2.
Expression of classical hematopoietic markers in BPDCN patients.

BPDCN, blastic plasmacytoid dendritic cell neoplasm; MPO, myeloperoxidase; HLA-DR, human leukocyte antigen-DR; BCL-2, B-cell lymphoma-2; CD, cluster of differentiation; pDC, plasmacytoid dendritic cell; Tdt, intranuclear terminal deoxynucleotidyl transferase.
Treatment response
In the study, a total of 63 patients had evaluable complete data. Among them, five patients discontinued treatment and succumbed to disease progression, with a median survival duration of only 1.0 month. Initial complete remission (CR) was achieved in 44 patients (69.8%), although 10 patients (22.7%) experienced relapse. It is noteworthy that there was no significant discrepancy observed in the initial CR and relapse rate among patients who received AML-like, ALL-like, or NHL-like chemotherapy regimens as illustrated through the data presented in Tables 4a and 4b. There seemed to be no link between central nervous system infiltration and the disease’s relief or recurrence. Additionally, the study findings revealed that the initial response to inductive treatment was markedly superior among patients under 39 years of age compared to older patients, with percentages of 86.1% and 50.0%, respectively (p = 0.019; Tables 4a and 4b). Subsequent to the primary refractory or relapsing scenarios, a second line of treatment was administered to a cohort of 12 patients, resulting in 9 patients achieving a subsequent CR. Within this group, four patients were administered an AML-like regimen, three were subjected to regimens containing a Bcl-2 inhibitor, and two received high-dose methotrexate (HDMTX) treatment. Moreover, a total of 35 patients underwent HSCT, comprising 32 allogeneic HSCT and 3 autologous HSCT recipients. Notably, 25 individuals were transplanted while in the initial CR state (22 allo-HSCT and 3 auto-HSCT), whereas two patients underwent allo-HSCT transplantation during disease relapse subsequent to the initial CR. Among the eight patients who received allo-HSCT following rescue chemotherapy, seven were transplanted in the state of subsequent CR. Five patients experienced relapse post-HSCT: one auto-HSCT recipient (33.3%) relapsed after 20 months, and four allo-HSCT recipients (12.5%) relapsed as well. Despite some patients undergoing a second allo-HSCT transplantation post-CD123 targeted therapy or chimeric antigen receptor-T (CAR-T) cell therapy, four patients ultimately succumbed to BPDCN progression after relapse. Noteworthy was that out of the 35 patients who received HSCT, 6 individuals (17.1%) passed away due to severe graft-versus-host disease (GVHD), while the majority, 25 out of 35 patients (71.4%), remained alive in persistent CR following HSCT at the time of analysis.
Therapeutic evaluation analysis of age and chemotherapy regimens in BPDCN patients.
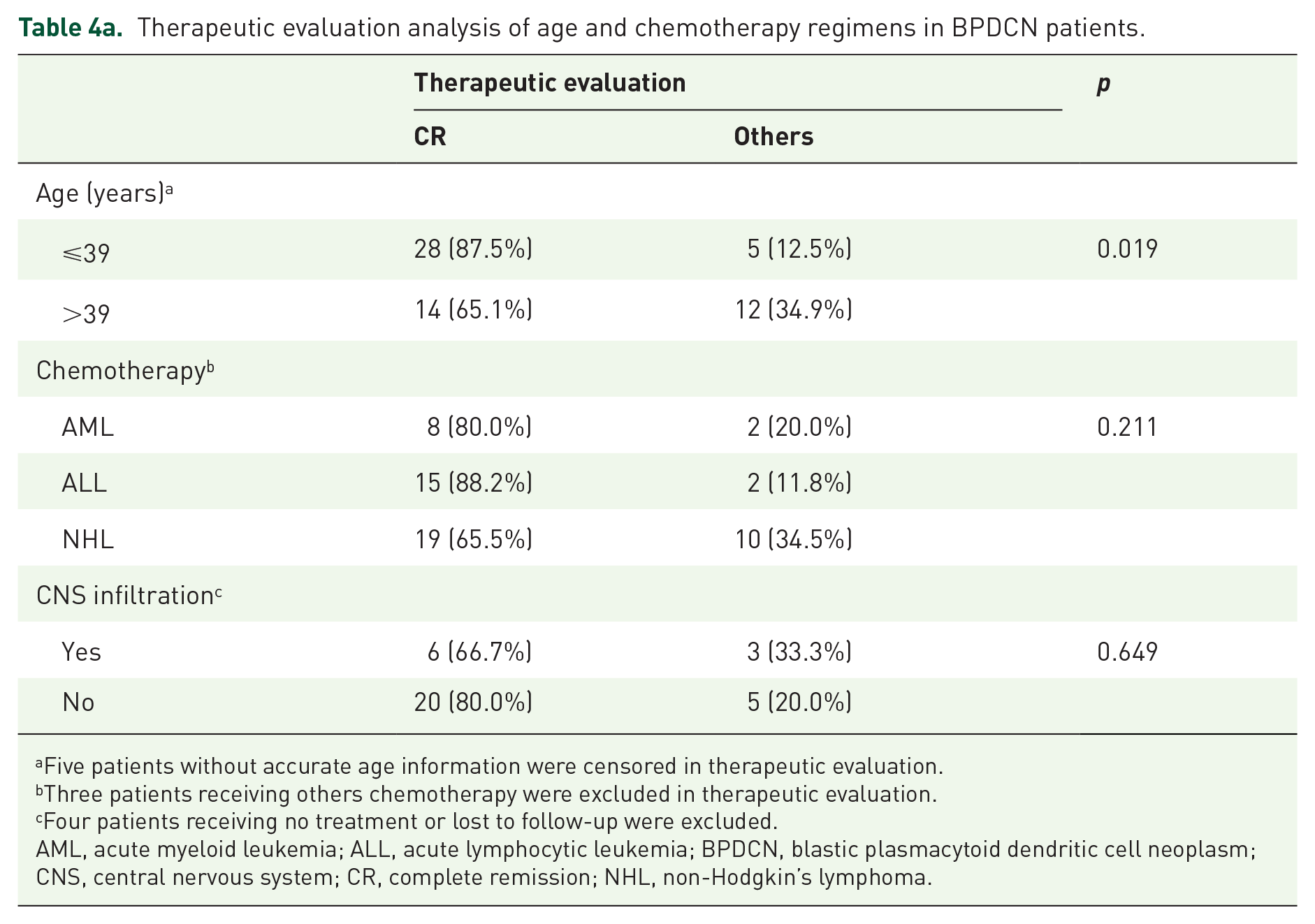
Five patients without accurate age information were censored in therapeutic evaluation.
Three patients receiving others chemotherapy were excluded in therapeutic evaluation.
Four patients receiving no treatment or lost to follow-up were excluded.
AML, acute myeloid leukemia; ALL, acute lymphocytic leukemia; BPDCN, blastic plasmacytoid dendritic cell neoplasm; CNS, central nervous system; CR, complete remission; NHL, non-Hodgkin’s lymphoma.
Recurrence analysis of age and chemotherapy regimens in BPDCN patients.

Five patients without accurate age information were censored in recurrence rate evaluation.
Three patients receiving others chemotherapy were excluded in recurrence rate evaluation.
Four patients receiving no treatment or lost to follow-up were excluded.
AML, acute myeloid leukemia; ALL, acute lymphocytic leukemia; BPDCN, blastic plasmacytoid dendritic cell neoplasm; CNS, central nervous system; CR, complete remission; NHL, non-Hodgkin’s lymphoma.
Survival analysis and prognostic factors
In the univariate analyses presented in Table 5, age, sex, CD3 expression, and treatment group (HSCT versus No HSCT) were identified as significant factors impacting OS. Additionally, CNS infiltration emerged as a potential hazard factor, supported by a p value of 0.034 in the log-rank test [Figure 2(b)] and a p value of 0.054 in the univariate analyses (Table 5). Notably, no significant differences in survival rates were observed among patients receiving AML-like, ALL-like, or NHL-like regimens. Moving to the multivariate analysis, the impact of age and treatment group (HSCT versus No HSCT) on OS was further confirmed (Table 6). Specifically, younger patients exhibited longer survival times and better prognoses as evidenced by a noticeably longer median OS for patients under 39 years when compared to older patients [Figure 2(d)]. Moreover, HSCT emerged as a protective prognostic factor with a sustained beneficial effect, independent of age, according to the multivariate analysis. Patients who received HSCT displayed improved median OS compared to those receiving only chemotherapy or those who opted out of treatment at the time of diagnosis with respective median OS durations of 13.0 and 1.0 months. Importantly, as of the last follow-up, 25 out of 35 patients (71.4%) who underwent HSCT after initial chemotherapy [both autologous (n = 3) and allogeneic (n = 32) transplant recipients] remained in persistent CR, precluding the calculation of a median OS for this group. Although a specific overall median OS could not be determined, the survival outcomes associated with transplantation notably improved the OS time when compared to all chemotherapy regimens, underscoring the effectiveness of transplantation [Figure 3(a)]. However, when only the population of underage individuals was considered, the implementation of HSCT after inductive chemotherapy did not improve patient outcomes [Figure 3(b)]. Further investigation is needed to explore the role of HSCT and the best timing for its implementation in pediatric BPDCN patients.
Univariate analysis of prognostic factors for OS in BPDCN patients.

The estimates of the parameters are given with their 95% CIs.
p Value <0.05 is considered statistically significant.
BPDCN, blastic plasmacytoid dendritic cell neoplasm; CI, confidence interval; CNS, central nervous system; HR, hazard ratio; HSCT, hematopoietic stem cell transplantation; OS, overall survival.

Comparison of survival according to different factors: OS curves according to CD3 expression (a), CNS infiltration (b), sex (c), and year (d).
Multivariate analysis of prognostic factors for OS in BPDCN patients.
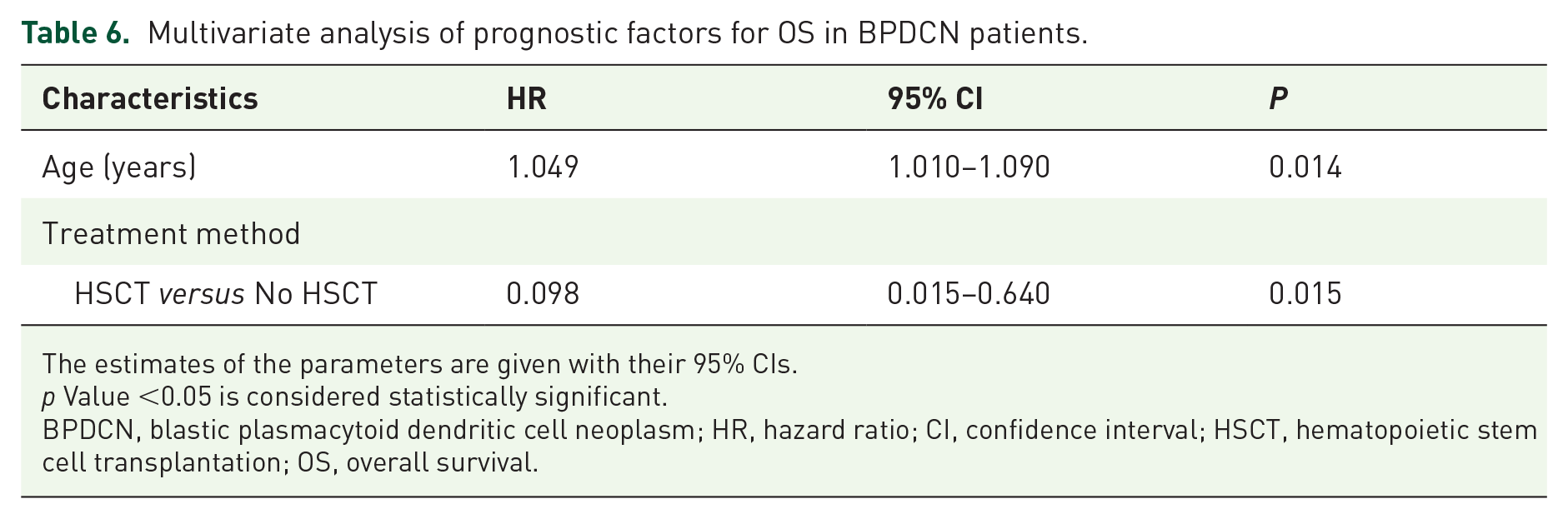
The estimates of the parameters are given with their 95% CIs.
p Value <0.05 is considered statistically significant.
BPDCN, blastic plasmacytoid dendritic cell neoplasm; HR, hazard ratio; CI, confidence interval; HSCT, hematopoietic stem cell transplantation; OS, overall survival.

Comparison of survival according to treatment (HSCT or Non-HSCT): OS curves according to treatment (HSCT or not) in all BPDCN patients (a) and OS curves according to treatment (HSCT or not) in underage BPDCN patients (b).
Discussion
Constrained by the rarity of BPDCN, researchers face challenges in acquiring adequate prospective data for analysis to inform clinical diagnosis and treatment. The existing literature predominantly consists of sporadic case reports, with only a limited number of retrospective analysis articles examining more than 15 cases. 9 Notably, there is a lack of large-scale retrospective analysis reports focusing on Chinese patient populations. This gap in the literature motivated our research team to undertake data collection and analysis for the purpose of this study.
BPDCN has heterogeneous clinical manifestations, commonly affecting older men but also presenting in children. Based on our data, the disease was associated with a distinct immunophenotype that includes universal expression of CD4, CD56, CD123, CD303, CD304, and HLA-DR, consistent with previous research findings. 10 Despite our pathological specimens showing negativity for CD56 in four patients, the diagnosis of BPDCN was supported by a combination of immunohistochemical standards and pathological morphological characteristics. This observation aligns with existing literature reports, 11 underscoring the importance of clinical physicians remaining vigilant to avoid misdiagnosis. Notably, CD3, a T-cell marker, is typically not expressed in BPDCN, 12 a fact corroborated by our finding of an 87.5% negative rate. In our univariate analyses, the expression of CD3 was linked to an adverse prognosis with a hazard ratio of 3.25 and a p value of 0.038, demonstrating its potential as a prognostic marker.
Most BPDCN patients typically present initially with cutaneous lesions, followed by symptoms and signs from involvement of the hematological system and CNS, including the bone marrow, peripheral blood, lymph nodes, and cerebrospinal fluid.13,14 In our study, it was found that 23.7% of BPDCN patients had confirmed CNS infiltration, which may be considered a potential hazard factor as per the univariate analyses, where the p value of CNS infiltration was determined to be 0.054. Reported rates of CNS involvement range from 20% to 60%15,16; the actual rate is unknown, as lumbar puncture at diagnosis has not historically been part of a standard of care workup. The potential role of CNS infiltration in prognosis highlights the importance of performing CSF cytology and imaging (when appropriate) at diagnosis, during treatment, and in instances of relapse. These actions are essential for accurately assessing the occurrence and progression of CNS disease in pediatric patients. 17 Although the CNS has been indicated in numerous studies as a possible sanctuary for tumor cells and a common site for recurrence, 18 there appeared to be no link between central nervous system infiltration and the disease’s relief or recurrence in our study. This might result from insufficient standardization in the examination and treatment of nervous system infiltration or limited numbers of cases. Efforts are ongoing to augment the dataset of CNS involvement cases in order to achieve more precise determination of outcomes. The necessity of prophylactic intrathecal injection remains uncertain. As seen in previous studies, the inconsistent application of preventive intrathecal injections across different healthcare facilities hindered the establishment of conclusive evidence in our research.
Previous studies indicate that at initial diagnosis, both minor and adult BPDCN patients exhibit similar clinical manifestations with the main differentiating factor being the presence of cutaneous lesions in some cases. 19 It was observed that younger patients showed significantly higher initial CR rates and better prognosis compared to older patients in our study. This improved outcome in younger patients could be attributed to their higher tolerance to intensive conventional chemotherapy regimens, facilitating the achievement of initial CR.20,21 Additionally, the incidence of transplantation related adverse events in underage patients undergoing HSCT is lower. 22
Several treatment regimens have been employed in clinical practice for BPDCN over the years without a consensus on the most effective approach. Some clinicians opt for the ALL-like regimen due to the expression of CD4 and CD56, 23 while others prefer NHL-like chemotherapy regimens such as CHOP.4,24 Given its classification as an AML subtype, 25 some physicians choose the AML-like regimen for BPDCN. Tagraxofusp, a novel CD123 targeted agent, has emerged as the first specific treatment approved for BPDCN. 26 However, its use is linked to a distinct toxicity known as capillary leak syndrome, prompting a ‘black box warning’ on the FDA label. 27 Therefore, for patients who cannot tolerate CD123 targeted therapy, a retrospective analysis of traditional chemotherapy regimens is invaluable. Our research findings revealed no significant disparities in the initial CR rate and relapse rate among patients treated with AML-like, ALL-like, or NHL-like chemotherapy regimens. While some studies highlight BPDCN’s responsiveness to various treatments, it is noted that the induction response rate with NHL-like regimens is comparatively lower.28,29 This might be explained by the fact that the therapeutic effect of CHOP or CHOP-like regimens is not satisfactory. 9 Nonetheless, the utility of NHL-like regimens cannot be discounted entirely, as evidenced by the continuous CR status observed in all patients receiving the DDGP regimen pre-HSCT in our investigation.
Scholars have proposed that chemotherapy cannot extend the OS time of BPDCN patients and that it merely offers temporary relief for the disease. 30 Despite the high initial CR rate, the frequent recurrence and progression of BPDCN have compromised past achievements in conventional chemotherapy. 31 Our study findings revealed that patients undergoing HSCT exhibited a significantly longer median OS compared to those receiving other treatments, with only a 14.3% disease recurrence rate post-HSCT. Nevertheless, when considering the population of underage individuals, the implementation of HSCT after inductive chemotherapy did not improve patient outcomes. Previous studies indicate that pediatric patients with BPDCN generally have better outcomes than adult patients with the same condition, and allogeneic HSCT after the initial CR should be limited to pediatric patients with BPDCN exhibiting high-risk features.21,32 However, the definition of high-risk features depends on clinical practitioners and remains unclear. This is the reason for the lingering uncertain regarding the role of HSCT and its optimal timing in pediatric patients with BPDCN. 17 Due to the limited number (three cases) of patients who received auto-HSCT, we were unable to determine if there existed a substantial discrepancy between allogeneic and autologous HSCT.
GVHD, a frequent and severe complication following HSCT, continues to significantly impact patient morbidity post-procedure, thereby restraining therapeutic advantages. 33 Our research indicated that 17.1% of patients who underwent HSCT succumbed to severe acute GVHD. Although risk factors for GVHD have been extensively outlined, the accurate prediction of GVHD development post-HSCT is still lacking in clinical practice. 34 Researchers have persistently endeavored to surmount this challenge, and their efforts have borne fruit in the form of innovative strategies for GVHD prevention and mitigation. Recent studies published in Blood this year have showcased that the implementation of an oIL-2/oIL-2Rβ system can enhance the effectiveness of Treg therapy, which plays a pivotal role in the prevention of acute GVHD. 35
Future research on BPDCN should concentrate on investigating molecular, histochemical, and genetic changes to improve disease diagnosis and treatment. This includes developing treatment strategies that incorporate conventional chemotherapy, HSCT, and targeted therapies tailored to patients of all ages.
Conclusion
Age and HSCT were independent prognostic factors for BPDCN patients. Younger patients had longer OS and better prognosis. Consolidating HSCT in the initial CR state significantly prolonged OS and improved outcomes for BPDCN patients.
Supplemental Material
sj-docx-1-tah-10.1177_20406207241251602 – Supplemental material for A systematic literature review of 74 Chinese blastic plasmacytoid dendritic cell neoplasm patients
Supplemental material, sj-docx-1-tah-10.1177_20406207241251602 for A systematic literature review of 74 Chinese blastic plasmacytoid dendritic cell neoplasm patients by Chen Gong, Ying Liu and Mingzhi Zhang in Therapeutic Advances in Hematology
Supplemental Material
sj-docx-2-tah-10.1177_20406207241251602 – Supplemental material for A systematic literature review of 74 Chinese blastic plasmacytoid dendritic cell neoplasm patients
Supplemental material, sj-docx-2-tah-10.1177_20406207241251602 for A systematic literature review of 74 Chinese blastic plasmacytoid dendritic cell neoplasm patients by Chen Gong, Ying Liu and Mingzhi Zhang in Therapeutic Advances in Hematology
Supplemental Material
sj-docx-3-tah-10.1177_20406207241251602 – Supplemental material for A systematic literature review of 74 Chinese blastic plasmacytoid dendritic cell neoplasm patients
Supplemental material, sj-docx-3-tah-10.1177_20406207241251602 for A systematic literature review of 74 Chinese blastic plasmacytoid dendritic cell neoplasm patients by Chen Gong, Ying Liu and Mingzhi Zhang in Therapeutic Advances in Hematology
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.