
Abstract
In the United States, prostate cancer is the most frequent malignancy in men and ranks second in terms of mortality. Although recurrent or metastatic disease can be managed initially with androgen ablation, most patients eventually develop castration-resistant disease within a number of years, for which conventional treatments (eg, chemotherapy) provide only modest benefits. In the last few years, immunotherapy has emerged as an exciting therapeutic modality for advanced prostate cancer, and this field is evolving rapidly. Encouragingly, the US Food and Drug Administration (FDA) has recently approved two novel immunotherapy agents for patients with advanced cancer: the antigen presenting cell-based product sipuleucel-T and the anti-CTLA4 (cytotoxic T-lymphocyte antigen 4) antibody ipilimumab, based on improvements in overall survival in patients with castration-resistant prostate cancer and metastatic melanoma, respectively. Currently, a number of trials are investigating the role of various immunological approaches for the treatment of prostate cancer, many of them with early indications of success. As immunotherapy for prostate cancer enters its golden age, the challenge of the future will be to design rational combinations of immunotherapy agents with each other or with other standard prostate cancer treatments in an effort to improve patient outcomes further.
Why Use Immunotherapy in Prostate Cancer?
Knowing that all cancer cells express tumor-specific antigens produced by genetic alterations (and epigenetic dysregulation), it is rational to design therapies to induce targeted antitumor immune responses. Cancer immunotherapy approaches range from activating innate and adaptive immune effector mechanisms to neutralizing inhibitory and suppressive mechanisms. 1 Strategies to stimulate effector immune cells include treatment with cytokines, vaccination with tumor antigens or enhancement of antigen presentation. Strategies to neutralize immune suppressor mechanisms include chemotherapy (for example, low-dose cyclophosphamide), the use of antibodies in an attempt to deplete regulatory T cells, and the use of antibodies targeted against immune-checkpoint molecules (for example, anti-CTLA4 antibodies and anti-PD1 antibodies) (Tables 1 and 2) (Fig. 1).2,3
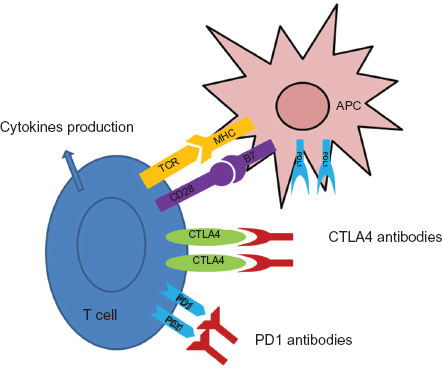
After an antigen presenting cell (APC) becomes activated, tumor antigens are presented to CD8 T cells via major histocompatibility complex (MHC) molecules that interact with the T cell receptor (TCR) on T cells (signal 1).
Selected completed and ongoing immunotherapy trials in prostate cancer.

Summary of key features of selected immunotherapies for advanced prostate cancer.

Antigen-Specific Immunotherapy
Using the antigen-specific immunotherapy approach, a specific tumor antigen is directly targeted either by incorporating the antigen into a vaccine or by loading that antigen onto antigen-presenting cells (APCs). Among the different potential antigens that could be used for prostate cancer, the most popular targets that have been used most commonly in clinical development include prostate-specific antigen (PSA), prostatic acid phosphatase (PAP), and the prostate-specific membrane antigen (PSMA).
Sipuleucel-T
In 2010, a 512-patient study led by Kantoff et al showed a statistically significant survival advantage using the APC-based immunotherapy sipuleucel-T, with men in the active treatment arm surviving 25.8 months while the placebo arm had a survival of 21.7 months (P = 0.03). 4 Trial participants included men with metastatic CRPC who had no or minimal disease-related symptoms, and most of which (85%) had not yet received cytotoxic chemotherapy. This study was significant, because it was the first time that a cancer “vaccine” demonstrated a survival benefit in any metastatic solid tumor. Based largely on the results of this trial (as well as two other smaller phase III trials), the FDA approved sipuleucel-T in 2010 for the treatment of asymptomatic metastatic, castration-resistant prostate cancer. Sipuleucel-T (Dendreon, Seattle, WA, USA) is a personalized; antigen presenting cell-based immunotherapy manufactured using patients’ own leukocytes and following the general principles of the dendritic cell vaccines. 5 To generate a dose of sipuleucel-T, patients undergo leukapheresis, and the resulting cells are transferred to one of several processing facilities where the enriched monocytes are cultured ex vivo for 36–44 hours with a fusion protein that links prostatic acid phosphatase (PAP) with granulocyte macrophage-colony stimulating factor (GM-CSF). PAP was selected based on evidence that immunization can drive T cell-mediated responses. In this process, GM-CSF's role is to activate and mature the dendritic cells that initiate an immune response, and potentially to direct the PAP protein into these cells. 6 After 2 days of culture, antigen-loaded APCs along with other immune cells (including T cells) contained in the culture become activated and are infused back into patients. Patients typically receive three rounds of leukapheresis and intravenous infusions of the immunotherapy product every 2 weeks as a complete course of therapy. It has been demonstrated that CD54 expression is substantially and consistently upregulated on activated APCs during culture with the PAP-GM CSF fusion protein, and that this upregulation can be quantified, supporting the use of CD54 upregulation as a surrogate for assessing human APC activation and as a potential measure of sipuleucel-T efficacy. 7 To this end, it has recently been showed that the cell number and the CD54 expression in men treated with sipuleucel-T may correlate with survival in metastatic castration-resistant prostate cancer, 8 although this finding requires validation.
Future studies should investigate whether sipuleucel-T has a role in patients with earlier-stage (non-metastatic) disease. Providing immunologic treatment during the earlier stages of the disease, when the immune response is more potent and tolerance has not developed, may have the potential to change the natural history of the disease. Based on the concept that immunotherapy will most likely prove maximally beneficial in the setting of a minimal disease burden, 9 studies have been initiated to test the efficacy and feasibility of administering sipuleucel-T in earlier stages of prostate cancer. The earliest stage at which immunotherapy could be used would be prior to primary prostatectomy. In this regard, sipuleucel-T was recently administered to approximately 40 men prior to surgery in a multisite phase II trial. 10 In that study, the primary endpoint involved immunological analysis of the prostatectomy specimens. Biopsy of the specimens showed increased frequency of T cells in prostate cancer tissue at the interface of the benign and malignant glands, suggesting that sipuleucel-T can modulate the presence of lymphocytes at the prostate tumor site. 11 In addition, after primary surgery or radiation therapy, approximately 30%–40% of men with prostate cancer present with a rising prostate-specific antigen (PSA) without evidence of overt metastatic disease. 12 This disease state, known as biochemical recurrence, would be another ideal setting for immunological intervention, as the cancer has clearly recurred but disease burden is at a minimum. A trial aiming to investigate the combination of androgen ablation and sipuleucel-T in this patient population is currently underway, 13 and will evaluate both immunological and clinical endpoints. Because the optimal sequence of androgen ablation and immunotherapy is not clear, this trial has two arms: one in which sipuleucel-T is given before androgen ablation and another in which it is given after androgen ablation has been initiated. 14
Poxvirus Vectors
One of the most popular approaches for cancer immunotherapy involves the use of viral vectors, since there has been extensive experience using such vaccines for the eradication of infectious illnesses such as small-pox. Another important factor is that we can incorporate large amounts of genetic material into viral vectors and it is easy to engineer them. 15 The way poxvirus vectors mediate their effect is by infecting epithelial cells. These epithelial cells subsequently die releasing cell material including multiple antigens which can be taken up by immature APCs. These APCs, after the uptake of antigens, are becoming activated and are able to present the tumor antigens to CD4+ and CD8+ T cells. The current version of the vaccine for prostate cancer known as TRICOM includes three co-stimulatory molecules (intercellular adhesion molecule 1 (ICAM1), lymphocyte function-associated antigen 3 (LFA3) and CD80.16,17 Because poxvirus-based vaccines tend to produce a strong antibody response which makes homologous prime-boost regiments insufficient, ProstVac-VF combines recombinant viral vectors (a vaccinia vector “prime” followed by an analogous flowlpox vector “boost”).18,19
In a recent phase II randomized trial by Kantoff et al in patients with metastatic castration-resistant prostate cancer using ProstVac-VF vs. placebo, patients receiving the immunotherapy had a better OS with 25 (30%) of 82 alive versus 7 (17%) of 40 controls alive at 3 years, and a superior median survival by 8.5 months (25.1 v 16.6 months for controls). 20 ProstVac-VF immunotherapy was well tolerated with no significant adverse effects. Currently, there are various ongoing trials using poxvirus-based vectors in men with prostate cancer. The first is a randomized phase II trial of docetaxel with or without ProstVac-VF in patients with metastatic castrate-resistant prostate cancer. 21 The primary endpoint of this trial is to evaluate the overall survival of patients treated with docetaxel and prednisone with or without vaccine therapy. Unfortunately, this trial was halted early prior to complete enrollment due to poor patient accrual. Another study 22 using ProstVac-VF is aiming to determine if treatment with the prostate cancer vaccine plus the antiandrogen flutamide is more effective than flutamide alone in delaying disease progression in patients with non-metastatic castration-resistant prostate cancer. Finally a 3-arm randomized, double-blind, phase III study in men with asymptomatic or minimally symptomatic metastatic castrate-resistant prostate cancer 23 is evaluating if the combination of ProstVac-VF and GM-CSF can prolong overall survival when compared against ProstVac-VF alone (without GM-CSF) or against placebo.
DNA vaccines
DNA-based vectors are much less immunogenic than viral vectors that are able to produce a powerful inflammatory response. One way to enhance the immunogenicity of the DNA-based vectors is to incorporate specific pro-inflammatory cytokines, such a Toll-like receptor (TLR) agonists which activate APCs. Another way to attract APCs is to coadminister with the vaccine GM-CSF. In a study conducted by McNeel et al, twenty-two patients were treated in a dose-escalation trial with 100 μg, 500 μg, or 1,500 μg of a plasmid DNA (pTVG-HP) encoding prostatic acid phosphatase (PAP) co-administered intradermally with 200 μg granulocyte-macrophage colony-stimulating factor (GM-CSF) as a vaccine adjuvant, given a total of six times at 14-day intervals. No significant adverse events were observed. Three of 22 patients developed PAP-specific IFNγ-secreting CD8+ T-cells while nine of 22 patients developed PAP-specific CD4+ and/or CD8+ T-cell proliferation. The PSA doubling time was observed to increase from a median 6.5 months pretreatment to 8.5 months on-treatment (P = 0.033), and 9.3 months after 1 year of treatment (P = 0.054). 24
In another phase II randomized study, 25 investigators are aiming to determine if treatment with a DNA-based pTVG-HP vaccine (given together with GM-CSF as an adjuvant) can generate long-lived immune responses in men with biochemically- recurrent castration-resistant prostate cancer. With this PAP-encoding DNA vaccine, immune responses vary between different patients, potentially suggesting the need for individualized vaccination schedules in different patients.
Polyvalent Immunotherapy and Non-Specific Immunotherapy
Cell-based immunotherapy
GVAX is a good example of a polyvalent approach to cell-based immunotherapy, in which the vaccine is composed of GM-CSF-transduced tumor cells. 26 In this vaccine approach, we use the whole cell instead of one singe antigen, trying to initiate a more generalized immune response against multiple potential tumor antigens. GM-CSF is able to attract APCs and T cells to the vaccine site initiating an immune response to the tumor antigens.27,28 GVAX for prostate cancer employs the androgen-sensitive prostate cancer cell line LNCaP along with the castration-resistant prostate cancer cell line PC3, which are genetically modified in order to secret GM-CSF.29,30 Two recent trials (VITAL-1 and VITAL-2) using the GVAX approach in men with metastatic CRPC reported negative results and were prematurely terminated. 31 Some of the potential reasons for the failure of GXAV to produce positive clinical results have been outlined in other reviews. 32
Immune checkpoint blockade
A variety of inhibitory pathways are known to be upregulated in the tumor microenvironment and are known to enhance cytotoxic T-cell response against tumor antigens. These include those mediated through CTLA-4, PD-1, B7-H3, or B7x. Among those, the two checkpoints receptors that have been most extensively studied are CTLA-4 and PD-1. Cytotoxic T lymphocyte antigen 4 (CTLA-4) is an essential negative regulator of T-cell responses, inhibiting recognition of self antigens by T cells and having the ability to down regulate the antitumor immune response. 33 The importance of CTLA4 in down regulating the immune response was shown in early mouse studies, in which CTLA4-knockout mice died at 4–6 weeks of age from lymphocyte infiltration of vital organs.34,35 CTLA4 blockade has been well studied previously in patients with advanced melanoma, in which ipilimumab is associated with an approximate 10% objective response rate, but also a significant rate (25%–35%) of clinically important immune-related toxicities, such as colitis, neutropenia, dermatitis, pneumonitis and a variety of endocrine disorders including hypothyroidism and hypophysitis.36,37
Ipilimumab has been evaluated in several Phase I and Phase II trials in patients with prostate cancer, and objective clinical responses as well as declines in PSA levels have been described. 38 Based on those data, a randomized phase III trial is currently comparing ipilimumab against placebo in men with castration-resistant metastatic disease who have not responded to prior chemotherapy, 39 while another randomized phase III trial is comparing the efficacy of ipilimumab versus placebo in asymptomatic or minimally symptomatic patients with metastatic chemotherapy-naïve castration-resistant prostate cancer. 40 Recently, two phase I trials were completed combining ipilimumab with ProstVac-VF and GVAX, respectively.42,43 A number of clinical responses were seen, although the toxicity of these combinations was perhaps augmented compared to that of ipilimumab given alone. Finally, in a phase 2 study 44 which has now been completed, ipilimumab was given alone or in combination with docetaxel, in an effort to show the synergistic effect of chemotherapy and immunotherapy. Results from this study have not been reported yet.
Programmed Death-1 (PD-1) 41 is another immunological check point that has recently attracted interest in trials. Interaction between PD-1 and its ligand has been shown to lead to inhibition of T-cell function.45,46 In animal studies, PD1 blockade potentiates an antitumor immune response,47–49 and initiate autoimmune phenomena which are milder than CTLA4-knockout mice, with less mortality.50,51 Perhaps most importantly, PD-L1 has been shown to be upregulated in many human tumors and increase expression was associated with a poor clinical outcome, especially in renal cell carcinoma. 52 In a recent study, it has been reported that the CD8+ T cells that infiltrate the prostate gland in men with prostate cancer appear to express PD1. 53 A Phase I clinical trial using anti-PD1 (MDX-1106; Bristol-Meyers Squibb) has been completed with promising clinical responses in patients with different types of cancer (especially kidney cancer, lung cancer, melanoma, and colon cancer). MDX-1106 was generally well tolerated, with few serious adverse events, including immune-related deaths due to pneumonitis. 54 These data demonstrate the importance of PD-1 in cancer immunotherapy, suggesting that this agent would be a rational approach for the treatment of prostate cancer, either used alone or in combination with other traditional prostate cancer therapies.
Combining Immunotherapy with other Agents
The most effective strategy for attacking cancer is the multi-pronged treatment approach. In prostate cancer, and especially in advanced stages, it would appear beneficial to combine the novel immunotherapy agents with the more traditional established prostate cancer treatments. 55 Some of these combination strategies are reviewed below.
Combination with radioactive agents
One such strategy is to combine immunotherapy with radioactive agents. There are several ongoing trials including studies using 177Lu-J 591 (which is a radiolabeled monoclonal antibody to PSMA) alone 78 or in combination with other agents such as docetaxel 56 or ketoconazole. 57 Another phase II study 58 is using the radiopharmaceutical drug 153Sm-EDTMP (Quadramet) with or without ProstVac-VF in men with castration-resistant metastatic prostate cancer.
The concept of using radiation in prostate cancer is also exciting because it has been shown that irradiation of cancer cells can promote antitumor activity 59 through the uptake of the damaged tumor cells by APCs 60 which subsequently present the tumor antigens to immune cells inducing a pro-inflammatory response. 61 This process is not unique in radiation-induced cell death but can also be observed in chemotherapy-induced apoptosis. Several studies have demonstrated the synergistic effect of radiation and immunotherapy.62,63 In a trial of men undergoing primary radiotherapy for prostate cancer, 13 of 17 patients in the radiotherapy and immunotherapy combination treatment group demonstrated significant increase in the number of PSA-specific T cells, whereas there was no increase in the number of PSA-specific T cells the group that received radiotherapy alone.64,65 Recently, a phase I study by Beer et al 66 was completed. In this study patients were treated with escalating doses of ipilimumab every 3 weeks for 4 doses in cohorts of 6 patients at dose levels of 3, 5, and 10 mg/kg. After the 10 mg/kg cohort was completed, a protocol amendment added single fraction of radiation prior to ipilimumab starting at the 3 mg/kg dose level. Six patients had a confirmed > 50% PSA decline, 1 of 7 patients with measurable disease had a partial response in nodal metastases and the prostate and achieved an undetectable PSA after treatment with 10 mg/kg of ipilimumab. Nineteen patients experienced 29 immune-related adverse events including diarrhea/colitis, rash, hepatitis, and endocrinopathy. 66 Finally, the ongoing, randomized Phase III trial of ipilimumab in men with docetaxel-refractory metastatic castration-resistant prostate cancer 39 includes a low dose of radiotherapy administered prior to ipilimumab in an effort to prime an initial antitumor immune response.
Combination with androgen ablation
Another rational approach would be the combination of androgen ablation with immunotherapy. It has been shown previously that in aged mice, androgen ablation has a direct effect on the thymus, leading to regeneration of the thymus and the appearance of naïve T cells in the peripheral blood, while in humans androgen ablation has also been shown to correlate with increased infiltration of the prostate gland with CD4+ T cells. A Phase I study which combined ProstVac-VF with androgen ablation showed minimal toxicity and increased immune responses against PSA. 67 Multiple studies are now testing sipuleucel-T in combination with conventional and novel hormonal therapies. An ongoing phase 2 study 13 is currently examining the sequencing of sipuleucel-T and androgen deprivation therapy in men with non-metastatic prostate cancer and a rising PSA after primary treatment. 14 This study has two arms, one with sipuleucel-T followed by ADT and another with ADT followed by sipuleucel-T. In a separate phase 2 study, 68 patients with metastatic castration-resistant prostate cancer are going to receive sipuleucel-T with either concurrent or sequential administration of abiraterone plus prednisone (6 weeks after the last infusion of sipuleucel-T). Finally, several studies are evaluating the role of immune checkpoint blockade using ipilimumab in combination with androgen ablation.69–71 All of the above results support the idea of combining immunotherapy and androgen ablation strategies in order to enhance therapeutic effects.
Combining immunotherapy agents with each other
Finally, with the evolution of immune checkpoint blockade strategies, various trials have started to combine immunotherapy agents with each other, with promising results emerging in prostate cancer patients. The first study combined GM-CSF to ipilimumab in an effort to stimulate an antitumor immune response. In the highest dose cohort of 3 mg/kg of ipilimumab, 3 of 24 patients experienced a > 50% decline in PSA, whereas one of these patients developed a near-complete radiological response in liver metastasis. 72 In another study, GVAX was combined with ipilimumab in a dose-escalation trial. Decreases in PSA levels, as well as radiographically detectable tumor responses, were noted. 73 The incidence of high-grade toxicity of ipilimumab, such as endocrine disorders including hypophysitis, may be a limiting factor in these studies. 74 Currently, there is one ongoing trial in patients with metastatic melanoma boldly testing the combination of ipilimumab and a PD1-targeted antibody. 75 Two other phase I trials combining ipilimumab with ProstVac-VF and GVAX, respectively, were just completed.42,43 In the first study by Madan et al, patients with prostate cancer were treated with ProstVac-VF plus ipilimumab. 42 The ipilimumab dosing ranged from 1 to 10 mg/kg per dose, and patients received ipilimumab until disease progression or unmanageable toxicity. Patients had a median progression-free survival of 3.9 months and a median overall survival was 34.4 months. The most frequent toxicities were neutropenia, diarrhea, rash, transaminitis, and endocrine-related events including hypophysitis, hypothyroidism and adrenal insufficiency. 42 In the second study by Van den Eertwegh et al, 43 28 patients were treated with ipilimumab plus GVAX, with 12 patients treated in a dose-escalation cohort of ipilimumab (0.3 mg/kg per dose, 1 mg/kg per dose, 3 mg/kg per dose and 5 mg/kg per dose) and 16 patients were treated in the expansion cohort of 3 mg/kg per dose. The median overall survival in that trial was 29.2 months with colitis, transaminitis, diarrhea, rash, and endocrine-related toxicities including hypophysitis and adrenal insufficiency as the most frequent toxicities. 43 In these trials, although the clinical activity of the combination strategies was promising, it would appear that certain adverse events were more prominent, highlighting the necessity to carefully evaluate the toxicity of these combination immunotherapy regimens before proceeding to larger trials. 76
Conclusion
The use of sipuleucel-T and ipilimumab in recent pivotal oncology trials (and their subsequent FDA approval) has opened new frontiers in the battle against cancer. However, clinical benefits remain modest and the quest for novel immunotherapeutic agents or combinations is as important as ever before. While encouraging data from early-phase clinical trials have resulted in the development of Phase III programs to evaluate ProstVac-VF and ipilimumab in men with metastatic CRPC, it is unlikely that any single immunotherapy drug used alone is going to have a major or sustained clinical benefit. To this end, the notion of combining individual immunotherapy agents either with each other (eg, vaccines with immune checkpoint blockades) or with other traditional treatment approaches (eg, androgen deprivation therapy, chemotherapy, and radiotherapy) is expected to maximize the potential benefit of these treatments. Finally, while the field of cancer immunotherapy is currently plagued by a lack of reliable indicators of treatment effect, it will be crucial moving forward to identify immunologic biomarkers that can predict clinical outcomes, allowing us to offer our patients a more personalized treatment approach. While these challenges may seem daunting, our early success with sipuleucel-T in men with advanced prostate cancer should remind us of the potential promise of immune-directed therapies and motivate us to continue on our path to transform lethal prostate cancer into a manageable chronic illness.
Author Contributions
Conceived and designed the experiments: SAB and ESA. Analysed the data: SAB and ESA. Wrote the first draft of the manuscript: SAB and ESA. Contributed to the writing of the manuscript: SAB and ESA. Agree with manuscript results and conclusions: SAB and ESA. Jointly developed the structure and arguments for the paper: SAB and ESA. Made critical revisions and approved final version: SAB and ESA. All authors reviewed and approved of the final manuscript.
Funding
Author(s) disclose no funding sources.
Competing Interests
Author(s) disclose no potential conflicts of interest.
Disclosures and Ethics
As a requirement of publication author(s) have provided to the publisher signed confirmation of compliance with legal and ethical obligations including but not limited to the following: authorship and contributorship, conflicts of interest, privacy and confidentiality and (where applicable) protection of human and animal research subjects. The authors have read and confirmed their agreement with the ICMJE authorship and conflict of interest criteria. The authors have also confirmed that this article is unique and not under consideration or published in any other publication, and that they have permission from rights holders to reproduce any copyrighted material. Any disclosures are made in this section. The external blind peer reviewers report no conflicts of interest. Provenance: the authors were invited to submit this paper.