
Abstract
A 34-year-old man presented to the hospital with right-sided headache. He was diagnosed with GBM. He underwent resection of the tumor with placement of carmustine impregnated wafers. Then he underwent adjuvant chemotherapy with temozolamide. Before the completion of chemotherapy he had a recurrence. He underwent re-resection with placement of carmustine impregnated wafers. Subsequently he had eighteen cycles of salvage biochemotherapy with bevacizumab and irinotecan. To date, routine MRI scans of the brain have not shown evidence of recurrence. He continues to be in remission three years after treatment with bevacizumab and irinotecan.
Introduction
Glioblastoma multiforme (GBM) is the most common primary brain tumor in adults. 1 There are about 12,000 to 14,000 cases of GBM diagnosed annually in the United States. 2 Despite aggressive multidisciplinary treatment approaches, the prognosis for GBM is poor, with a median survival of approximately 15 months and less than a 10% 5-year survival rate. 3 Furthermore, the prognosis for recurrent GBM is dismal, with a median survival of 4 to 6 months and less than a 5% survival rate at 5 years.4,5
Currently, the standard of care for the treatment of newly-diagnosed GBM is surgical resection, followed by concurrent radiation therapy with temozolomide, completed by adjuvant chemotherapy with temozolomide. 6 The addition of temozolomide to radiation therapy has improved survival, although benefit from the addition of temozolomide is primarily restricted to patients with a tumor with a methylated promoter of methyl-guanine methyl transferase (MGMT). 7 However, 45% to 55% of primary GBMs have an unmethylated MGMT promoter, and these patients have a worse prognosis.
Despite the survival benefit associated with surgery, adjuvant radiation therapy and chemotherapy, the majority of patients relapse following initial therapy. The optimal management for patients with recurrent or progressive GBM is unclear. In general, treatment for recurrent GBM may involve repeated resection, focal irradiation, and systemic or experimental therapies. Patients with recurrent GBM often undergo serial salvage therapies, but the decision about which treatments to pursue and in what sequence depends on specific factors related to each patient and tumor.
Since 1976, carmustine impregnated wafers (Gliadel®) is the last chemotherapy approved for use as an adjunct to surgery to prolong survival in patients with recurrent GBM for whom surgical resection is indicated. In May 2009, the FDA approved the use of bevacizumab for the treatment of progressive GBM despite treatment. Until bevacizumab, all other experimental therapies tested in recurrent or progressive GBM failed to meet the FDA guidelines for approval.
We report a case of a patient with recurrent GBM who continues to be in remission three years after re-resection followed by biochemotherapy with bevacizumab and irinotecan.
Case Presentation
The patient is a 34-year-old healthy man with no significant past medical history who presented to the hospital with severe right-sided headache and visual disturbances in October 2005. He had a magnetic resonance imaging scan (MRI) of the brain with gadolinium that revealed a large right temporoparietal hemorrhagic mass highly suggestive of a primary brain neoplasm (Fig. 1). CT scan of the chest, abdomen, and pelvis with IV contrast were negative for a primary tumor. The patient subsequently underwent a craniotomy and resection of the tumor with placement of carmustine impregnated wafers (Gliadel®). Post-surgically the patient recovered well and the pathology report revealed GBM. Shortly after recuperation from his surgery, the patient was treated with radiation therapy and concurrent temozolomide at 75 mg/m2 daily for the 6-week duration of his radiation therapy. He was also placed on dexamethasone simultaneously. The patient tol-erated the radiation with concurrent chemotherapy well. His neurological status was intact except for one episode of seizure for which he was given levetiracetam. After completion of radiation therapy, MRI of the brain demonstrated postoperative changes with surgical margin enhancement and diffuse T2 changes consistent with edema and/or non-enhancing neoplasm with no evidence midline shift or mass effect (Fig. 2). The patient was treated with two cycles of temozolomide at 300 mg/m2 daily for 5 days. After his second cycle of temozolomide, a MRI of the brain with gadolinium revealed diminishment in the postoperative cavity as well as enhancement along the margins consistent with response to therapy. He completed the adjuvant chemotherapy with three more cycles of temozolomide at 300 mg/m2 daily for 5 days. In August 2006, ten months after the diagnosis of GBM and before the completion of adjuvant chemotherapy, the patient returned to the office with complaints of blurred vision. MRI of the brain with gadolinium showed progressive disease with focus of enhancement seen inferomedially to the surgical cavity associated with edema extending to the right basal ganglia, right temporal lobe and right thalamus (Fig. 3). At that point the patient had a recurrence. He underwent re-resection with placement of carmustine impregnated wafers (Gliadel®). MRI with gadolinium demonstrated postsurgical changes within the right temporal lobe with no significant mass effect or midline shift (Fig. 4). The pathology report revealed GBM. Post-operatively he was started on salvage biochemotherapy. Beginning October 2006, he underwent treatment with four cycles of irinotecan and bevacizumab. He tolerated the chemotherapy well except for an acneiform rash involving the face and the upper chest for which he was treated with topical clindamycin. Repeat MRI of the brain with gadolinium showed diffuse, marked increase in T2 hyperintensity without enhancement diffusely involving the right parietal and frontal parenchyma. There was also mild enlargement of the ventricular system, diffuse effacement of the right hemispheric sulci and mass effect indicating progression since the prior study. He was continued on two more cycles of irinotecan and bevacizumab. After six cycles of bevacizumab and irinotecan, PET/CT scan (positron emission scan/computed tomography) of the head that showed a large photopenic area consistent with post treatment defect. He was continued on ten more cycles of irinotecan and bevacizumab. A repeat PET scan was done and showed no evidence of metabolically active tumor. He was continued on two more cycles of irinotecan and bevacizumab. In August 2007, after completing eighteen cycles of bevacizumab and irinotecan over a period of ten months, it was decided to terminate the chemotherapy since the patient's neurological status was stable and repeat MRI and PET/CT scans showed no evidence of recurrence or metabolically active tumor (Fig. 5).
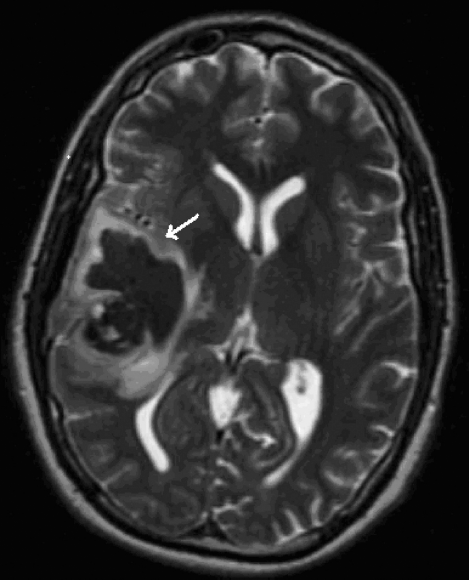
MRI of brain with gadolinium showing a large right temporoparietal hemorrhagic mass (arrow).

MRI of brain with gadolinium showing postoperative changes with surgical margin enhancement, edema and/or non-enhancing neoplasm (arrow).

MRI of brain with gadolinium showing new heterogeneously enhancing lesion adjacent to the surgical bed within the right temporal lobe consistent with recurrent neoplasm (arrow).

MRI of brain with gadolinium showing postsurgical changes within the right temporal lobe with no significant mass effect or midline shift (arrow).

MRI of brain with gadolinium showing overall decrease in midline shift and edema with no evidence of recurrence (arrow).
The patient has been on levetiracetam and his neurological status has been stable until now. He has been followed up at the office every 6 months and serial MRIs of the brain have shown no recurrence of the tumor. To date, it has been 3 years after the patient's last dose of biochemotherapy with irinotecan and bevacizumab for recurrent glioblastoma multiforme. Thus he is considered to be in remission.
Discussion
Glioblastoma multiforme (GBM) is a rapidly progressive brain tumor that is best managed with a combined modality approach incorporating maximal surgical resection, adjuvant postoperative radiation therapy with concurrent temozolomide, and adjuvant temozolomide. The prognosis of patients diagnosed with this deadly brain tumor is grim even if a multidisciplinary aggressive treatment approach is utilized. Temporary remission is only achieved in majority of the patients. Despite the use of a combined modality approach, most patients eventually relapse after initial therapy.
The optimal management for patients with recurrent or progressive GBM is unclear, and there are no randomized trials that directly compare active intervention versus supportive care. The value of re-intervention at the time of relapse was suggested in a retrospective review of 168 patients with recurrent GBM who were treated at a single center. Patients undergoing re-intervention were more likely to have a higher progression free survival (PFS) at 12 months (21 versus 8 percent), and to be alive at both one year (71 versus 15 percent) and two years (32 versus 5 percent). 8 One of the most important prognostic factors for benefit from re-intervention for recurrent GBM is the pre-treatment performance status.9–12 Other factors that contribute to the benefit from second-line therapy include the volume of residual disease, the histologic grade (both at initial therapy and at recurrence), the relapse-free interval, and recurrence pattern (local versus diffuse). As per the NCCN clinical practical guidelines in oncology, management of locally recurrent GBM includes re-resection and impregnation of carmustine polymers followed by systemic chemotherapy/re-radiation or re-resection followed by systemic chemotherapy/re-radiation. Management of locally recurrent GBM that is not amenable to resection includes systemic chemotherapy, radiation, brachitherapy or supportive care if poor performance status.
The surgical management of recurrent GBM is controversial. The indications for a debulking reoperation in a patient with recurrent disease are not firmly established. Recent studies have suggested that re-operation provides a 3–5 month median survival, without significant increase in morbidity and mortality. 13 Several studies have concluded that prolongation of survival time after re-operation was statistically significant in the Karnofsky performance subgroup (60 or greater).7,8 Other favorable prognostic variables include young age (<=50), a longer interval since the original surgery, and the extent of the second surgical resection. Re-resection improves symptoms, maintains quality of life, delays symptom progression, reduces corticosteroid doses and also improves response to chemotherapy and/or radiotherapy. Thus, surgical re-resection in recurrent GBM should be considered in selected patients.
Carmustine impregnated wafers (Gliadel®) may prolong survival in locally recurrent GBM after re-resection. In a phase III trial in which, patients were randomly assigned to have either carmustine or placebo impregnated wafers into the tumor site during surgery for locally recurrent disease, it was found that the carmustine wafer group had a significantly longer median survival (31 versus 23 weeks with placebo).2,14 Although it was found that carmustine impregnated wafers play a vital role in recurrent GBM, many patients are not candidates for a repeat gliadel wafer placement.
Irinotecan is a topoisomerase-1 inhibitor with excellent penetration into the central nervous system. 14 It has a different mechanism of action than alkylating agents such as temozolomide, carmustine, and lomustine and has demonstrated modest activity in recurrent GBM with response rates of 0% to 17%.15–18 The 6-month progression-free survival is less than 20% when irinotecan is used as a single agent for recurrent GBM.18,19 Thus, there is the need for combination chemotherapy in recurrent GBM.
The pathognomic features of GBM are the presence of necrosis and vascular proliferation. In May 2009, the US Food and Drug Administration approved bevacizumab as a single agent for patients with GBM with progressive disease despite treatment with other therapies. It is a monoclonal antibody to vascular endothelial growth factor, which is strongly expressed in GBM tumor cells. Although this overexpression is associated with a poor prognosis, it also provides a target that can be blocked by bevacizumab. Bevacizumab was approved for use in selected patients with GBM based on the results of two single-arm trials, AVF3708g and NCI 06-C-0064E.
The most recent trial, known as AVF3708g (BRAIN) evaluated 167 patients with GBM who had progressed on radiation and temozolomide. This was a phase II, multicenter, open-label, non-comparative trial. The patients were randomly assigned to receive bevacizumab 10 mg/kg alone or in combination with irinotecan 340 mg/m2 or 125 mg/m2 (with or without concomitant enzyme-inducing antiepileptic drugs) every 2 weeks. The primary endpoints were 6-month PFS and objective response rate. The secondary endpoints were safety and overall survival. The results revealed that the estimated 6-month PFS rates were 42.6% for the bevacizumab group and 50.3% for the bevacizumab plus irinotecan group. The median overall survival times (OST) were 9.2 months for the bevacizumab group and 8.7 months for the bevacizumab plus irinotecan group. The overall conclusion of the study was that bevacizumab alone or in combination with irinotecan was fairly well tolerated and highly efficacious in recurrent GBM. 19
The second trial known as the NCI 06-C-0064E was based on a single-arm, single-site study of 56 patients who had disease progression after receiving temozolomide and radiation therapy. These patients received bevacizumab (10 mg/kg IV) every 2 weeks until disease progression or unacceptable toxicity was noted. The objective response rate was 19.6% and the median response duration was 3.9 months. 19
There was also another retrospective study that was conducted at Henry Ford Hermelin Brain Tumor Center from 11/15/2005 to 04/01/2008 on 51 patients with recurrent high-grade gliomas treated with bevacizumab plus irinotecan. It was done to determine the efficacy, safety and patterns of responses, and occurrences in patients with recurrent high-grade gliomas treated with bevacizumab plus irinotecan. The results showed that the median progression free survival (PFS) time was 7.6 months, the 6-month PFS rate was 63.7%, the overall survival rate (OS) at 6 months was 78.0% and the 12-month OS rate was 42.6% for recurrent GBM. 20
Conclusion
GBM is a very aggressive malignancy that has a dismal prognosis despite combined modality treatment approaches with surgery, radiotherapy and chemotherapy. The recurrence is inevitable; its management is often unclear and case dependent.
We can conclude that the survival rate was improved in patients treated with irinotecan and bevacizumab compared with historical controls. It is unclear if irinotecan is the optimal chemotherapy, although studies have demonstrated that patients with recurrent high grade gliomas treated with the combination of bevacizumab and irinotecan demonstrate improved clinical outcome when compared to historical data. There is marked clinical benefit with the inclusion of bevacizumab in treatment regimens for recurrent GBM, as demonstrated by several trials. The anti-VEGF effect of bevacizumab is likely responsible for the clinical improvements.
We can conclude that this patient remains in remission 3 years after the initiation of salvage biochemotherapy consisting of bevacizumab and irinotecan. We can confidently report that his response and overall survival time exceeds by far of what is reported in the literature. It is also important to mention that the recurrence occurred after ten months of the diagnosis of GBM before the completion of adjuvant chemotherapy. As mentioned above, studies have revealed that the maximum median overall survival for patients with recurrent GBM is 9 months. The age of this patient and the high Karnofsky performance status are good prognostic features and certainly contribute to the continued remission. It is possible that re-resection would also have played a pivotal role in addition to bevacizumab in maintaining the extended remission.
Currently there are no randomized clinical trials that directly compare active intervention versus supportive care in the overall survival of recurrent GBM. Future research may be directed towards investigating the overall survival in patients opting for comfort care in recurrent GBM.
Disclosure
This manuscript has been read and approved by all authors. This paper is unique and is not under consideration by any other publication and has not been published elsewhere. The authors and peer reviewers of this paper report no conflicts of interest. The authors confirm that they have permission to reproduce any copyrighted material.