
Abstract
Sebaceoma is a benign tumor composed of incompletely differentiated sebaceous cells of varying degrees of maturity. Sebaceomas was never reported as a known premalignant lesion.
This is a report of a sixteen year old boy who presented with a malignant transformation of a recurrent sebaceoma which was excised twice by Moh's surgery. Excision was done with a free margin of 1 cm down to the parotid fascia. Reconstruction was performed on the same set by using cervicofascial flap extending down to the supraclavicular area. The patient had an uneventful postoperative period apart from distal marginal necrosis of the flap, which healed nicely with conservative measures and daily dressing and was sent to our cancer centre to start his adjuvant radiotherapy.
Previous literature stated that sebaceoma is a distinctive benign tumor. We have presented a case of an unusual malignant transformation of a preauricular recurrent sebaceoma. This indicates that sebaceoma does have a potential risk of malignant transformation. We believe that managing recurrent sebaceoma more aggressively with wide local excision and postoperative adjuvant radiotherapy would provide better prognosis.
Keywords
Introduction
Sebaceoma is a benign tumor composed of incompletely differentiated sebaceous cells of varying degrees of maturity. Sebaceoma was never reported as a known premalignant lesion. This is a report of a sixteen year old male patient who presented with a malignant transformation of a recurrent sebaceoma of the right preauricular area.
Case Report
A previously healthy sixteen year old male patient presented with a right preauricular lesion. This was excised by general surgery department and was reported as a sebaceous cyst. One year later he presented with a friable nodule measuring 1 cm x 0.75 cm in the scaphoid fossa of the right ear and incisional biopsy showed histological features of sebaceoma (Figs. 1, 2). Moh's surgery was performed twice. The preauricular area, superior and inferior crura, triangular fossa and the choncha of the right ear were found to be involved. The resulted defect was reconstructed with a full thickness skin graft.

Original leasion.

One year later the patient presented with a 0.5 cm x 0.75 cm soft purplish lesion. Incisional biopsy was consistent with sebaceous carcinoma (Figs. 3, 4). MRI study showed a 3.25 x 2.25 x 4.5 cm mass extending to the Masseter muscle and petrous bone medially, the cartilaginous part of the external auditory meatus posteriorly and the upper border of the right parotid gland inferiorly. One prominent ipsilateral lower cervical lymph node was felt, but fine needle examination showed no malignant metastasis (Fig. 5).

Recurrence of lesion after Moh's surgery.

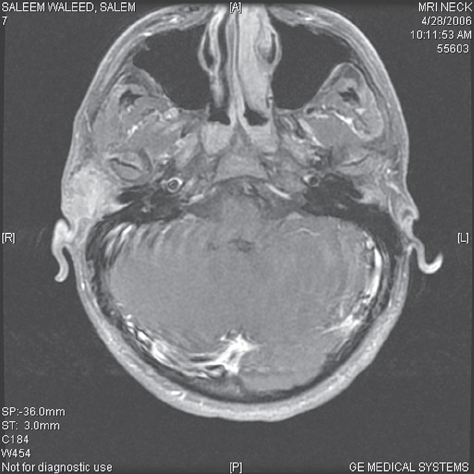
MRI study showed a 3.25 x 2.25 x 4.5 cm mass extending to the Masseter muscle and petrous bone medially, the cartilaginous part of the external auditory meatus posteriorly and the upper border of the right parotid gland inferiorly.
This was managed by wide local excision with postoperative radiotherapy. Excision was done with a free margin of 1 cm down to the parotid fascia. Local cervicofascial rotational flap area (Fig. 6) was used to reconstruct the resulted defect. Pathological analysis revealed T4 N0 M0 sebaceous carcinoma of the preauricular area with microscopic infiltration of the parotid fascia. All other margins were free. The cervical lymph node showed reactive changes and benign salivary gland inclusions without evidence of tumor metastasis. Further excision of the superficial part of the parotid was avoided to preserve the main trunk of the facial nerve and its branches.

(
The patient had uneventful postoperative period apart from distal marginal necrosis of the flap, which healed nicely with conservetive measures and daily dressing and was sent to our cancer centre to start his adjuvant radiotherapy. The patient was followed for 13 months with no evidence of recurrence.
Discussion
Sebaceoma is a new term proposed to designate a distinctive rare benign neoplasm of adnexal epithelium with differentiation toward sebaceous cells. 1 Most authors1–4 described this lesion as solitary or sometimes multiple nodules or plaques that have the appearance of a basal cell epithelioma and may show ulceration with a rolled, pearly border. Occasional tumours are more deeply located and appear cystic. The colour may be fleshy or of a waxy, yellowish hue, and the surface may be verrucose. Most lesions are located in the head and neck area. It usually grows slowly, but a sudden increase in growth rate can occur. The best treatment of sebaceoma is surgical excision.
The histologic spectrum extends from that seen in sebaceous adenoma to lesions that may be difficult to distinguish from sebaceous carcinoma. 4 Basal cell carcinoma with sebaceous differentiation is an uncommon event; most such cases also represent sebaceoma. 6
Sebaceous carcinoma is a rare, aggressive, malignant tumor that is derived from adnexal epithelium of sebaceous glands76 and complete surgical excision is required. 8 Reports of excellent results with Moh's surgery suggest that this maybe the treatment of choice. 9
In a clinicopathological study of five cases with sebaceous carcinoma arising in nevus sebaceous of Jadassohn, it has been shown that sebaceous carcinoma was always accompanied by other benign or malignant adnexal lesions such as sebaceoma, syrigocystadenoma papilliferum, syringocystadenocarcinoma papilliferum, trichoblastoma, trichlemmoma, desmoplastic tricholemmoma, or syrigoma. 10 The coexistance of sebaceous carcinoma, trichoblastoma, and sebaceoma was also reported in a nevus sebaceous. 11 In our case report Moh's surgery was performed in the histopathological diagnosis of sebaceoma, and a coexisting sebaceous carcinoma will be hard to miss. However, the possibility of the presence of sebaceoma and sebaceous carcinoma concurrently cannot be dismissed.
Conclusion
We have presented a case of an unusual malignant transformation of a preauricular recurrent sebaceoma. This indicates that sebaceoma could have a potential risk of malignant transformation. Managing recurrent sebaceoma more aggressively with wide local excision and postoperative adjuvant radiotherapy would possibly provide better prognosis.