
Abstract
The treatment of chronic lymphocytic leukemia (CLL) has evolved over the past decade. Our better understanding of disease biology and risk stratification has allowed delivering more effective therapies. In fact, front-line chemoimmunotherapy has demonstrated improvement in overall survival when compared to chemotherapy in randomized studies. Yet, treatment of relapsed CLL remains challenging and few agents are effective in that setting. Ofatumumab (Ofa) is a humanized monoclonal antibody targeted against CD20 with demonstrable activity in rituximab-resistant CLL cell lines. This agent was recently approved for the treatment of relapsed/refractory CLL patients who have failed fludarabine and alemtuzumab. In this review, we provide a historical perspective on approaches to CLL as front-line and in the relapsed setting. We further summarize novel anti-CD20 antibodies with specific emphasis on ofa. We review studies that led to ofatumumab's approval including pre-clinical data, trials using ofa in combination therapies, and adverse events/toxicities reported with this agent.
Introduction
Chronic lymphocytic leukemia (CLL) is characterized by the progressive accumulation of phenotypically mature malignant lymphocytes likely a combination of predominant resistance to apoptosis and a component of continuing proliferation. 1 CLL cells usually co-express CD5, CD23, CD19, CD79b and CD20, but the level of expression of CD20, CD79b, and surface immunoglobulin is low compared to normal B lymphocytes. 1 The International Working Group for CLL (IWCLL) has clarified that the presence of 5000 monoclonal B lymphocytes/μl is required to diagnose CLL rather than 5000/μl lymphocytes; emphasizing the importance of demonstrating clonality to establish the diagnosis. 2 In addition, the IWCLL formally recognized monoclonal B lymphocytosis (MBL); an entity characterized by less than 5000 monoclonal lymphocytes/μl in the blood; with an annual risk of progression to CLL of 1%–2%. 2
Our understanding of CLL biology has evolved rapidly allowing us to divide CLL into unfavorable high-risk and favorable low-risk disease. 3 The novel prognostic indicators that allowed this division recognize the differences in disease behavior and prognosis within each clinical stage raising the question as to whether our current clinical staging system needs to be revised. Characteristically, patients with unfavorable CLL carry the unmutated IgVH, 4 have over 20% of malignant cells expressing the zeta-associated tyrosine kinase protein (ZAP-70), 5 with ≥30% of cells expressing CD38 by flow cytometry, 6 and have adverse genomic aberrations generally defined as 17p and 11q deletions. 7 These latter patients respond less well to our best therapies and responding patients have higher risk of relapsing more quickly and dying from the disease.8–10
While we have made substantial strides in finding aggressive combination chemotherapies and chemoimmunotherapy regimens (CIT) that have substantial activity in the front-line setting, 11 our ability to treat relapsed or refractory disease has been limited. Patients with relapsed disease are frail, demonstrate poor performance status, their disease is usually resistant to standard chemotherapy, their immune system precludes aggressive measures, and they frequently carry unfavorable prognostic features. 12 Despite higher response rates and prolonged disease-free intervals when CIT is implemented in front-line CLL, there is no agreed upon standard as to the most effective therapy in relapsed disease especially in older patients where allogeneic stem cell transplantation is not an option. Accordingly, the need for active agents in this adverse clinical setting is urgent. In this article, we briefly review the evolution of treatment paradigms in CLL, discuss the importance of targeted therapies and in particular focus on monoclonal antibodies specific for CD20 antigen (Fig. 1) as the targeting of this receptor has made a large difference in our overall responses including complete remission rates in CLL. We describe clinical trials that led to the novel anti-CD20 monoclonal antibody ofatumumab's approval in relapsed CLL, and suggest future directions. This review is timely in that newer therapies are now being designed specifically for patients with relapsed/refractory disease where choices of therapy are typically limited and responses are short-lived.

CD20 molecule and the binding sites of rituximab and ofatumumab.
Historical Perspective of Up-Front Therapy
Recent advances in combination chemotherapies and the identification of highly effective membrane receptor targeted monoclonal antibodies have allowed the introduction of effective regimens with high remission rates and better potential of eradicating disease to very low levels. The first major advance in modern treatment of CLL was the demonstration that purine analogues provided patients with better complete remission (CR) rates, improved progression-free survival (PFS), and recently better overall survival (OS) compared with alkylating agents.13,14 Fludarabine (F) was the purine analogue most commonly studied although other analogues (pentostatin and cladribine) have well documented and substantial activity in this disease.15,16 The paradigm that F inhibits the repair of alkylating-agent induced DNA interstrand crosslinks that enable leukemic cells to overcome the cytotoxic effects of alkylating agents provided the rationale to combine F with cyclophosphamide (C). 17 Three prospectively designed randomized studies have clearly shown the superiority of FC combination compared to F monotherapy making FC the most robust combination chemotherapy regimen in upfront CLL therapy.18–20 FC provided patients with high CR rates (24%) and prolonged PFS (30–48 months) although OS was not better than F monotherapy. With the knowledge that monoclonal antibodies have an impact on the leukemic burden in CLL, combining chemotherapy with CD20 directed agents was the next logical step. The first suggestion that chemoimmunotherapy (CIT) might improve the outcome in CLL was reported by Byrd et al when the combination of F with rituximab (R) demonstrated high response rates, CR, and PFS compared to F alone or to the sequential program of F followed by R.21,22 Subsequently, the regimen of FCR (fludarabine, cyclophosphamide, and rituximab) pioneered by Keating et al showed unprecedented overall response (OR) rates (95%, CR 72%) with some patients attaining molecular remissions that amounted to truly negligible levels of leukemia burden. 23 However, other CIT combinations showed similar OR, specifically the PCR (pentostatin, cyclophosphamide, and rituximab) and FCR-Lite (attenuated doses of FCR with maintenance rituximab).24,25 While the OR rates were similar between FCR and PCR, the CR rate favored FCR. However, it was suggested that PCR might be better tolerated in patients with advanced age, renal dysfunction, or elevated beta-2-microglobulin. 26 This latter aspect is not trivial as the mean age of CLL patients in this country is around 70 with higher prevalence of renal dysfunction in the older cohort.
Recently, the German CLL Study Group (GCLLSG) reported on a randomized phase III study comparing FCR to FC. With a median follow up of 38 months, the OR favored FCR (95% vs. 88%, P = 0.001) with better CR rates (44% vs. 22%, P < 0.001). 11 Importantly, PFS was superior in the FCR arm (52 vs. 33 months, P < 0.001) with more patients alive at 37 months in the FCR arm (84% vs. 79%, P = 0.01). Of interest, however, this GCLLSG trial has only had a CR level in the low 40% range likely reflecting the community-based cohort rather than referral populations seen with the earlier phase 2 studies. This study justified implementing FCR as the standard front-line approach in young, fit patients where there is typically little comorbidity. 27
Treatment of Relapsed and Refractory Disease
There is no universally agreed upon standard approach to patients with relapsed or refractory disease. While some benefit from second line therapy initially, others require aggressive measures and stem cell transplantation. 28 Furthermore, the fact that most relapsed/refractory patients carry resistant clones and demonstrate aggressive biologic features makes selecting the appropriate therapy a truly challenging endeavor. 29 To a certain extent this has been made easier by two antibodies specific for CD52 and CD20. The following discussion lists several treatment options for the relapsed/refractory CLL cohorts but does not necessarily imply our hierarchy of choices for this patient population.
Alemtuzumab is a humanized monoclonal antibody that targets CD52 with notable clinical activity in CLL. Keating et al reported an OR of 33% with 2% CR in 93 heavily pretreated CLL patients. 30 The median OS was 16 months for the entire population and 32 months for responders; an outcome that compares favorably with the reported median OS of 10 months in comparable albeit historical control patients. 31 The activity of R alone in relapsed/refractory CLL has been marginal and remissions were partial and of short duration making this antibody a less ideal monotherapy for this cohort. 32 Combining alemtuzumab with R has been explored in the relapsed/refractory33,34 setting with some activity that led to further development of this regimen in the upfront approaches.35,36 It is important, however, to note that we have learned that not all patients are appropriate for alemtuzumab treatment as it is less effective in patients with bulky nodal disease (>5 cm). 30 In fact, Tam et al reviewed the outcome of 99 patients who were F-refractory and ineligible or refractory to alemtuzumab. 37 The OR to first salvage therapy other than transplantation was 23%, with no CRs. Early death (within 8 weeks of commencing first salvage) occurred in 13% of patients, and 54% of patients experienced a major infection during therapy while OS was 9 months. These poor results highlight the urgent need for effective therapeutic agents in this clinical setting.
To improve upon those results and given the well documented activity of CIT in front-line, several studies investigated several CIT programs in relapsed disease. While phase II studies conducted in that setting were mainly single institution with diverse patient population demographics, all have suggested better outcomes for OR and CR when compared to single agent chemotherapies. FCR was studied in relapsed disease with patients achieving a CR levels from 15%–25%. 38 Subsequently, a phase III randomized study compared FCR to FC confirming superiority of the former in terms of OR (70% vs. 58% P = 0.003), CR (24% vs. 13%, P < 0.001), and PFS (31 vs. 21 months, P < 0.001). 39 OS, however, was not found to be different although long-term follow-up might yet prove otherwise.
Other CIT combinations have been explored in the relapsed setting. The combination of F with alemtuzumab has been reported with CR rates >30%. 40 In addition, the combination of FCR plus alemtuzumab has been proven safe, effective, and able to overcome high-risk disease. 41 However, when given as a consolidative approach in CR patients treated front-line with FR, alemtuzumab has been associated with serious adverse events and has recently been shown to increase infectious complications risks and death. 42 Table 1 summarizes the pivotal CIT protocols commonly used in relapsed/refractory disease.
Select chemotherapy or CIT in the treatment of relapsed/refractory CLL.
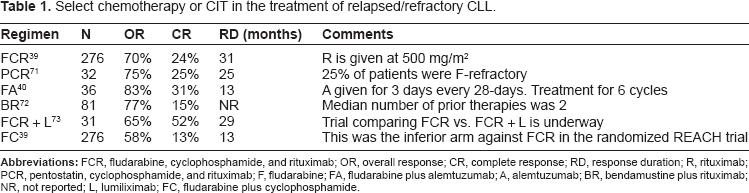
Abbreviations: FCR, fludarabine, cyclophosphamide, and rituximab; OR, overall response; CR, complete response; RD, response duration; R, rituximab; PCR, pentostatin, cyclophosphamide, and rituximab; F, fludarabine; FA, fludarabine plus alemtuzumab; A, alemtuzumab; BR, bendamustine plus rituximab; NR, not reported; L, lumiliximab; FC, fludarabine plus cyclophosphamide.
CD20
One approach to improve on our current therapeutics for relapsed/refractory disease is to optimize our targeted approach to CLL B cell membrane antigens/receptors. While the ideal receptor would be only on CLL B cells the CD20 receptor is at least restricted to B lymphocytes. CD20 is a transmembrane glycoprotein that is expressed on B-cells sparing the stem cells. 43 While the exact role of this antigen in B cell development and function is not clear, experimental data suggested that it has a role in B-cell activation, transmembrane calcium flux, and regulation of B-cell growth a proliferation. 44 The therapeutic appeal of CD20 as a target for therapy is that it is not internalized or downregulated after antibody binding. Antibody/antigen interaction also can theoretically allow for direct cell kill and cytotoxicity (ADCC). 45 Of interest the CD20 expression level in CLL B cells is lower than other malignant or normal B cells. The low level of CD20 expression in CLL likely explains the minimal activity of R as a single agent in this setting although such activity was enhanced when the drug was given more frequently (thrice/weekly) 46 or at much higher doses (>2000 mg/m2 for each infusion). 47 Given its known single agent activity, theoretical multiple killing functions and known efficacy in CIT, the strategy of developing and testing novel monoclonal antibodies that target the CD20 molecule has become an active strategy. See Figure 1 for more detail on the binding sites for both rituximab and the humanized antibody ofatumumab discussed below.
Rituximab
Rituximab is a chimeric anti-CD20 monoclonal antibody with remarkable activity in B-cell lymphoma. However, its activity in relapsed CLL is modest at standard doses; around 12% response. 48 This limited activity may be due to faint CD20 expression in CLL, and from CD20 acting as a decoy receptor or being present in soluble form in the plasma. However, the use of rituximab at higher doses or with greater frequency results in higher response rates as mentioned above.46,47 Most studies of rituximab in relapsed CLL show that the duration of response is only a few months.49,50 When rituximab is used alone as frontline therapy, higher response rates are seen with longer durations of response. However, most of these studies included heterogeneous patient populations including low-grade lymphoma, and most frontline trials included maintenance therapy; making the interpretation of clinical activity difficult.51,52 Rituximab is relatively safe in CLL, with infusion-related reactions being the most common adverse events seen albeit some of these reactions are robust. No increased in infectious complications have been reported although there are reports of reactivation of hepatitis B or JC virus.53,54 In addition, clinicians need to be vigilant to the “black box” warning regarding hepatitis B reactivation. Discussing all data pertaining to rituximab in CLL is beyond the scope of this review as our main focus in this review is the newer anti-CD20 antibodies.
Select Anti-CD20 Antibodies excluding Rituximab (Table 2)
Obinutuzumab
This is a humanized antibody that binds with high affinity and selectivity to the extracellular domain of the human CD20 antigen on B cells. 55 While rituximab recognizes type 1 epitope, obinutuzumab recognizes the type II epitope localized in the extracellular loop of CD20. In addition, the Fc-region of this antibody was glycoengineered to contain bisected, fucosylated carbohydrates allowing for increased affinity to the FcyRIII [a] allowing for better antibody-dependent cellular cytotoxicity (ADCC), direct cell kill, and apoptosis. 56 Salles et al conducted a phase I/II study with this antibody in 24 patients with CD20+ lymphoid malignancies confirming its' safety and activity. 57 Of those patients, 13 had relapsed/refractory CLL, of which 11 were evaluable. Seven patients exhibited a clinical response despite prior rituximab therapy. Subsequently, a phase I study was conducted in 13 refractory CLL patients (33% with high-risk cytogenetics). Here, even in a difficult high risk clinical cohort, the OR was 62% with transient neutropenia being the most common adverse event. 58
Veltuzumab
Veltuzumab is a unique and well crafted second-generation humanized anti-CD20 monoclonal antibody that contains 90%–95% human antibody sequences with identical antigen framework regions to epratuzumab (the humanized anti-CD22) and similar antigen-binding determinants to rituximab. 59 In vitro studies have demonstrated that veltuzumab has enhanced binding avidity and a stronger effect on complement-dependent cytotoxicity (CDC) compared with rituximab in selected cell lines. 60 Clinical trials of this agent are underway.
Current anti-CD20 monoclonal antibodies. 1

Ofatumumab
Ofatumumab (Ofa) is a human type 1 IgG antibody that binds a segment of CD20 that contains the small extra-cellular loop along with the N-terminal region of the second large extra-cellular loop. 61 Ofa exhibits a multiplicity of activity via CDC, ADCC, and has shown enhanced cell killing in rituximab-resistant cell lines. 62 It is hypothesized that enhanced CDC demonstrated with Ofa is related to its closer binding to the cell membrane.61,62 Using a mouse xenograft model, Bleeker et al evaluated the optimal dose of Ofa required to sustain in-vivo activity. 63 The authors demonstrated that B-cell repopulation occurred when serum Ofa levels dropped below 10 mcg/ml and accordingly sustaining these levels might enhance activity. Coiffier et al reported a phase I/II study in relapsed/refractory CLL with an OR of 50%, but the median response duration was only 3.7 months. 64 However, median duration to next treatment was 12 months. Subsequently, an international phase II study of 138 CLL patients with double refractory disease (that is refractory to fludarabine and alemtuzumab; n = 59) or those that were refractory to fludarabine with bulky (>5 cm) lymphadenopathy (here alemtuzumab was deemed a less viable option due to sizable lymphadenopathy [n = 79] was conducted. 65 The OR was 47%–58% with a median PFS of 5.7–5.9 months and median OS of 13.7–15.4 months. The drug was tolerated well, but a 25% incidence of infectious complications was reported. 65 These impressive clinical results in very high risk CLL led to its recent approval by the FDA for fludarabine-refractory disease and patients who have failed trials of alemtuzumab.
Österborg et al evaluated the relationship between baseline characteristics and pharmacokinetics (PK) data in patients enrolled onto this pivotal study. 66 Treated patients received 8 weekly infusions of Ofa followed by 4 monthly infusions (Dose 1, 300 mg; Doses 2–12, 2000 mg). Blood samples for PK analysis were collected at Dose 1, Dose 8, and Dose 12. The relationships between baseline patient characteristics, disease factors, and PK parameters were evaluated by multivariate regression analysis. Associations between PK and OR/PFS were also explored using univariate and multivariate logistic regression or Cox regression analyses. 66 This analysis showed that factors reflecting disease burden such as bone marrow involvement or elevated serum beta-2-microglobulin levels affect Ofa PK levels and that high serum concentrations after doses 8 and 12 were associated with improved outcome.
This latter study should provide guidelines for future studies with Ofa in the high risk and high disease burden CLL patient.
Ofa in Combination Therapies
The impressive clinical response data demonstrated with FCR and the clinical as well as theoretical advantage for Ofa over R based on the former CD20 directed agent's functional activity, paved the way to a multicenter phase II study combining FC with Ofa. Wierda et al conducted a randomized phase II study using two dose schedules of Ofa in combination with FC; the so-called O-FC regimen (30 patients received Ofa at 100 mg and 31 patients at 500 mg). 67 Treatment was repeated every 4 weeks for a total of 6 courses in chemotherapy-naïve CLL. OR rates were 77% (CR 32%) and 73% (CR 50%) for the low-dose and high-dose respectively. While these rates appear inferior to the historical phase II FCR remission rates, they are actually somewhat comparable to what has been reported by the GCLLSG in the FCR vs. FC randomized study. This is likely due to the fact that this study was a community based study reflecting the typical patient response to this CIT. Myelosuppression was the most common toxicity in this combination. Other important studies are underway including Ofa with pentostatin, Ofa/alemtuzumab regimen, Ofa and lenalidomide, and Ofa/bendamustine. 68
Toxicity and Adverse Events
Ofa has been well-tolerated with infusion-related adverse events being the most commonly reported. Most side effects occur on the day of infusion and are of grades 1 or 2. These are generally fevers, chills, shortness of breath, rash, and urticaria. Most infusion-related events occur with the first infusion and subside with further treatment doses.64,69
Coiffier et al observed grade 3 hepatitis in one patient although it remains questionable whether such event was Ofa-related. 64 Other severe adverse events included herpes zoster in one patient and fatal interstitial lung disease in another. Only 12% of patients experienced grade 3 or worse infectious complications although no significant drop in serum immunoglobulin levels was seen. Grade 3 or 4 hematologic toxicity was witnessed in 15% of patients with 6% having grade 3 or 4 neutropenia. 70
Conclusions
The activity of CIT in CLL in front-line and relapsed disease has clearly improved the overall outlook and outcome for patients with this disease. Refractory patients, however, have limited therapeutic options due to acquired drug resistance and the presence of high risk features. We believe that taking advantage of the membrane receptors more or less restricted to the leukemic B cell is an excellent target for continuing development to monoclonal antibodies like Ofa and future clinical trial evaluations in CLL. To this point, the hematology community is seeing that the novel CD20 directed antibody, Ofa, can be highly effective in high risk CLL patient populations with acceptable toxicity profile. This activity has been demonstrated as a single agent and will likely be enhanced when it is combined in correct dose and schedules with other targeted therapies or with aggressive chemotherapy combinations. The ever changing landscape of CLL therapeutics is eagerly awaiting further studies with unique monoclonal antibodies that target the CD20 membrane receptor.
Disclosure
This manuscript has been read and approved by all authors. This paper is unique and is not under consideration by any other publication and has not been published elsewhere. The authors and peer reviewers of this paper report no conflicts of interest. The authors confirm that they have permission to reproduce any copyrighted material.