
Abstract
Background:
Ocrelizumab is a humanized monoclonal antibody that targets the CD20 antigen found on B-cells. It is indicated in the treatment of both relapsing–remitting multiple sclerosis and primary progressive multiple sclerosis.
Objective:
The aim of this study is to report and describe the characteristics of alopecia areata following treatment with ocrelizumab for multiple sclerosis.
Results:
Five patients were reported, two female and three male. Four of the five patients had alopecia areata of the scalp, one of the five having alopecia to the beard area. All patients responded well to conventional treatment with topical and intralesional corticosteroids and topical minoxidil foam. Ocrelizumab can be associated with the development of alopecia areata. Initiation of proper treatment may lead to quick improvement or resolution of this potentially reversible adverse effect.
Introduction
Ocrelizumab is a humanized monoclonal antibody that targets the CD20 antigen found on B-cells. 1 It acts to deplete the human body’s B-cell stores by enhancing antibody-dependent cellular cytotoxicity and, to a lesser extent, complement-dependent cytotoxicity with a half-life of 26 days.1–4 It is indicated in the treatment of both relapsing–remitting multiple sclerosis (RRMS) and primary progressive multiple sclerosis (PPMS). Ocrelizumab is given as two 300 mg infusions separated by 14 days, with subsequent 600 mg doses every 6 months. Patients receive premedication with methylprednisolone (or equivalent) and an antihistamine. 5 Reported side effects of ocrelizumab include infusion-related reactions, depression, pain to the extremities, and peripheral edema. 6 Patients on ocrelizumab also have increased risk of infections and malignancy.1,6,7
Alopecia areata (AA) is an autoimmune disorder that causes non-scarring hair loss. AA is clinically characterized by well-demarcated round to oval patches of alopecia, most commonly on the scalp but can involve other areas such as the beard, eyebrows, or eyelashes. 8 Alopecia is a known side effect of immunomodulatory and chemotherapy agents used in multiple sclerosis (MS), such as teriflunomide and mitoxantrone.9,10 AA has also been reported as a side effect of other monoclonal antibody therapies for MS, including anti-CD52 agent, alemtuzumab, and anti-CD25 agent, daclizumab,11–13 but has not yet been documented as a side effect of ocrelizumab. There are also no reports of any anti-CD20 monoclonal antibody therapies inducing AA in the literature. On the contrary, there are several reports of anti-CD20 agent, rituximab, reducing risk of alopecia in lymphoma management as well as resolving cases of frontal fibrosing alopecia.14–16
Here, we report a case series in which five patients diagnosed with MS developed AA following initiation of ocrelizumab.
Case presentations
Five patients presented to the dermatology clinic with new-onset patches of AA within 4 months of starting treatment with ocrelizumab for MS. Summaries of each patient case can be found in Table 1. Each patient’s AA fully recovered following combined treatments of intralesional triamcinolone acetate injections (concentrations ranged from 3 to 8 mg/mL), topical betamethasone valerate 0.1% lotion, and 5% minoxidil foam, all of which are standard treatment of patchy AA (Figures 1 and 2).
Summary of patients who developed AA following ocrelizumab treatment for multiple sclerosis.

AA: alopecia areata; MS: multiple sclerosis; RRMS: relapsing–remitting multiple sclerosis; ILK: intralesional Kenalog (triamcinolone acetate) injections (concentrations ranged from 3 to 8 mg/mL); BMV: betamethasone valerate topical solution (0.1%, applied daily); Minoxidil (5% foam, applied nightly); PPMS: primary progressive MS.

Patches of alopecia areata of the beard of patient 1 before treatment.
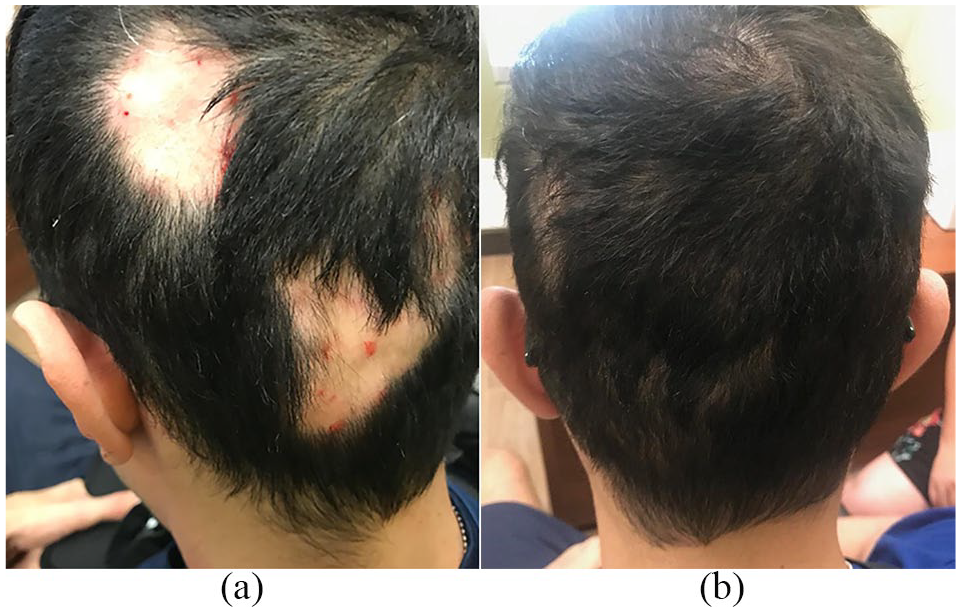
(a) Multiple patches of alopecia areata on the scalp of patient 3 immediately after first intralesional triamcinolone acetate injections. (b) Scalp of patient 3 eight weeks after one session of intralesional triamcinolone acetate injection and treatment with once daily betamethasone valerate 0.1% lotion and once daily minoxidil 5% foam application.
Discussion
Despite the extensive list of adverse effects of ocrelizumab in the treatment of MS, AA has not yet been reported as a side effect of the medication from the OPERA I/II and ORATORIO studies that assessed the efficacy and safety of ocrelizumab in RRMS and PPMS, respectively, 17 or on the Food and Drug Administration or Health Canada product monograph for ocrelizumab. 18 In fact, no autoimmune diseases have been reported as adverse effects of ocrelizumab.6,7,18,19 AA has been reported as a side effect of other disease-modifying treatments, including teriflunomide, mitoxantrone, alemtuzumab, and daclizumab,9–13 which are also used in the treatment of RRMS. However, to our knowledge, there have been no reports documenting the occurrence of AA following treatment with ocrelizumab in the management of MS or other diseases as of yet.
The prevalence of AA in the general global population is approximately 1.7% to 2.1%.8,20 It is possible that the diagnosis of AA in our patients presented was unrelated pathologically from ocrelizumab administration, as both AA and MS are autoimmune processes. However, the onset of AA within a few weeks to months of starting ocrelizumab treatment as well as the highly reported side effect of AA following other disease-modifying therapies in the treatment of MS makes it difficult to ignore the likelihood of ocrelizumab treatment being a causative factor in the development of AA in these cases.
In cases of AA development following alemtuzumab (an anti-CD52 treatment for both RRMS and chronic lymphocytic leukemia), secondary autoimmunity as a result of lymphocyte reconstitution has been a commonly proposed mechanism.11,12,21 Although the pathogenesis of this potential ocrelizumab side effect is currently unclear, it is possible that the pathology of AA development following ocrelizumab mirrors the secondary autoimmunity mechanism illustrated in research around alemtuzumab.
Although a confirmed causative relationship between ocrelizumab and AA in these cases cannot be proven, the cosmetic and psychosocial impact on patients cannot be overlooked.8,22 Therefore, both physician and patient awareness of this potential side effect are important. Since discontinuing ocrelizumab may not be feasible from an MS management standpoint, prompt diagnosis and initiation of treatment for AA may lead to quick improvement or resolution of this potentially reversible adverse effect, leading to improved patient quality of life and reduced morbidity.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
The patients included in this report provided consent for publication of the case report.