
Abstract
Introduction
Ovarian cancer has a high mortality and delayed diagnosis. Inflammation is a risk factor for ovarian cancer, and the inflammatory response is involved in almost all stages of tumor development. Immunohistochemical staining in stroma and epithelium of a panel of cytokines in benign and malignant ovarian neoplasm was evaluated. In addition, immunostaining was related to prognostic factors in malignant tumors.
Method
The study group comprised 28 ovarian benign neoplasias and 28 ovarian malignant neoplasms. A panel of cytokines was evaluated by immunohistochemistry (Th1: IL-2 and IL-8; Th2: IL-5, IL-6, and IL-10; and TNFR1). Chi-square test with Yates’ correction was used, which was considered significant if less than 0.05.
Results
TNFR1, IL-5, and IL-10 had more frequent immunostaining 2/3 in benign neoplasms compared with malignant tumors. Malignant tumors had more frequent immunostaining 2/3 for IL-2 in relation to benign tumors. The immunostaining 0/1 of IL 8 was more frequent in the stroma of benign neoplasms compared with malignant neoplasms. Evaluation of the ovarian cancer stroma showed that histological grade 3 was significantly correlated with staining 2/3 for IL-2 (P = 0.004). Women whose disease-free survival was less than 2.5 years had TNFR1 stromal staining 2/3 (P = 0.03) more frequently.
Conclusion
IL-2 and TNFR1 stromal immunostaining are related prognostic factors in ovarian cancer and can be the target of new therapeutic strategies.
Introduction
Ovarian cancer is a heterogeneous disease with different histological types.1,2 It has a high mortality, due to the lack of sensitive and specific biomarkers and the paucity of specific symptoms in initial stages, leading to delayed diagnosis. Methods for screening and early diagnosis of ovarian cancer in asymptomatic women have been ineffective. 3
Ovarian cancer is the most lethal gynecological cancer, and the overall survival at five years is less than 40%, with 95% survival for patients with cancer confined to the ovaries, 79% in those whose disease infiltrated into tissues adjacent to the ovaries, and 28% in those with an advanced clinical stage. Most patients have advanced-stage disease at diagnosis.4–7 Prevention is limited by inadequate knowledge regarding its causes and the lack of sensitive and specific biomarkers and available techniques for screening and early diagnosis. 8
Inflammation is a risk factor for ovarian cancer, and the inflammatory response is involved in almost all stages of tumor development.9–11 Chronic inflammation is associated with the development and progression of tumors. Epithelial ovarian cancer appears to be associated with inflammation, and the growth, differentiation, and signaling of these tumors appear to be regulated by cytokines.12,13 Biomarker expression may reflect the subtype, tumor diagnosis, and prognosis. That is, there is variation in the rate of expression of biomarkers among ovarian carcinoma subtypes.2,14 The growth and progression of ovarian carcinoma may be due to local cytokine-induced immunosuppression, which may lead to a state of immune privilege in the site of the tumor, allowing tumor development as an escape mechanism. 14
The cytokine expression may vary according to ovarian carcinoma subtype, contributing to the diagnostic and prognostic factors.2,15 This study evaluated immunohistochemical staining in stroma and epithelium of a panel of cytokines in benign and malignant ovarian neoplasms. Furthermore, epithelial and stromal immunostaining were related to prognostic factors in malignant tumors.
Patients and Methods
Patients
The study group comprised 56 patients receiving treatment from May 2009 to December 2013 at the Pelvic Mass Clinic of the Obstetrics and Gynecology/Oncology Research Institute (IPON)/UFTM. All patients underwent surgical treatment according to preestablished criteria16,17 and were subsequently diagnosed with ovarian benign neoplasia or primary ovarian malignant tumor. The exclusion criteria were ovarian cyst torsion, recurrent disease, and neoadjuvant chemotherapy.
Data recorded were as follows: age, parity, race, smoking, history of hormone therapy, age at menarche and menopause, hormonal status, histological grade, International Federation of Gynecology and Obstetrics (FIGO) stage, 18 histological type, lymph node metastasis, response to chemotherapy (complete, partial), and disease-free interval. In evaluating the histological grade, borderline tumors were considered well differentiated (grade 1). For other tumors, a pathologist reviewed the grade, dividing them into grade 1 (well differentiated), grade 2 (moderately differentiated), and grade 3 (poorly differentiated).
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration. The Research Ethics Committee (UFTM) approved the study (protocol number 1408/2009). Patients gave their written, informed consent to participate in the research.
Immunohistochemistry
The samples obtained by surgical resection were processed in paraffin. Biopsies were reviewed by an experienced pathologist and the selected paraffin blocks were subjected to further cuts of 4 mm thickness, in silanized slides (ATPS – Silano, Sigma® A3648), using the technique of streptavidin-biotin-peroxidase.
The slides were maintained at 56 °C for a period of 24 hours and then were deparaffinized in three baths of xylene remaining about 5 minutes each and dried in three baths of absolute alcohol, and 80% alcohol, for about 10 seconds. Subsequently, the slides remained in a phosphate buffered saline (PBS) for five minutes. Shortly after, the excess buffer was removed and the cut edge was dried carefully. Next, the slides were placed in tubes containing citrate buffer 10 mM (pH 6.0) or tris-Ethylenediamine tetraacetic acid (EDTA), which was supplemented with distilled water until the limit for 30 minutes at 100 °C. Then, the tubes were removed and were placed on the bench for cooling.
The slides were rinsed with distilled water and wiped. Hydrogen peroxide was added to 3% of each section for 10 minutes for blocking endogenous peroxidase. After that, the slides were washed in PBS and incubated with the primary antibody in about 18 hours in a humid chamber with a temperature of 3 °C-4 °C. The antibody was diluted with bovine serum albumin (Sigma®) according to the indications present in their specifications. These preparations with bovine serum albumin (BSA 2%) and primary antibody can block the nonspecific binding, to reduce background staining.

Immunohistochemical staining. Histological section of mucinous cystadenoma, showing epithelium staining 0 and stromal staining 0 by immunohistochemistry of polyclonal anti-IL-5 (
After overnight incubation at 4 °C with specific primary antibody, the slides were placed at room temperature, about 15 minutes, washed in PBS, and dried. The biotinylated secondary antibody (Dako Cytomation LSAB and System-HRP) was added to each slide for 30 minutes at room temperature in a humid chamber. Then, the slides were washed in PBS and dried. The streptavidin peroxidase complex (Dako Cytomation LSAB and System-HRP) was added for 30 minutes.
The primary antibodies used were IL-2 antibody (H-133, rabbit polyclonal IgG; sc-7896; Lot # H0811; Santa Cruz Biotechnology, Inc.), IL 5 antibody (H-85, rabbit polyclonal IgG; sc-7887; Lot D0708; Santa Cruz Biotechnology, Inc.), NLC-L-IL-6 antibody (mouse monoclonal; Lot L155309; Leica Microsystems Nussloch), IL-8 RB (E-2) antibody; mouse monoclonal IgG; sc-7304; Lot F1510; Santa Cruz Biotechnology, Inc.), IL-10 antibody (polyclonal; Lot 11042807; cat No. 250713; Abbiotec), and p-TNFR1 (receptor 1 Tumor Necrosis Factor) (be 274) antibody (rabbit polyclonal IgG, Lot B0509; sc-130220; Santa Cruz Biotechnology, Inc.); positive controls were used.
After washing in PBS, the slides were developed by the addition of a chromogen solution, diaminobenzidine (DAB) (Dako Cytomation and Liquid DAB Substrate Chromogen System), for five minutes. Then, the slides were washed in running water and counterstained with Harris hematoxylin.
Finally, the slides were immersed in three baths of absolute alcohol for about 10 seconds each, to remove excess water, and then they were washed with xylene. The coverslips were added on slides with Entellan for further analysis.
Three observers (MPJ, AM-F, and RSN) evaluated the sections subjectively, and the intensity of staining was evaluated using the following designations: 0 (no signal – 0%–10% of the labeled sectional area), 1 (weak – 11%–25% of the labeled sectional area), 2 (medium – 26%–50% of the marked cutting area), and 3 (strong – 51%–100% of the labeled sectional area).
Statistical analysis
Interobserver agreement between staining intensity scores was calculated by kappa, and discordant evaluations were defined by the more experienced researcher. Chi-square test with Yates’ correction and Fisher was used (GraphPad InStat), which was considered significant if less than 0.05.
Results
Patients with ovarian neoplasms were divided into two study groups: benign group (28 patients) and malignant group (28 patients). Of those with malignant neoplasms, the mean age was 49.9 ± 14.1 years, the mean parity was 2.2 ± 1.7 births, the average age of menarche was 13.1 ± 1.7 years, and the average age of menopause was 49.7 ± 4.2 years. Regarding the use of contraception, 2 patients (7.1%) had used hormonal contraceptives, none used condoms, and 4 (14.3%) had undergone tubal ligation. One patient (2.5%) used hormone replacement therapy, and six patients (21.4%) were smokers. In relation to hormonal status, 10 (35.7%) were premenopausal, and 18 (64.3%) were postmenopausal. Six patients (21.4%) died.
Of those with benign neoplasms, the mean age was 47.6 ± 10.5 years, the mean parity was 2.8 ± 1.8 births, and the average age of menarche was 13.1 ± 1.6 years. Regarding the use of contraception, six patients (21.4%) had used hormonal contraceptives, none used condoms, and 13 (46.4%) had undergone tubal ligation. Two patients (7.1%) used hormone replacement therapy, and six patients (21.4%) were smokers. In relation to hormonal status, 17 (60.7%) were premenopausal, and 11 (39.3%) were postmenopausal.
In relation to FIGO stage, 13 patients (46.4%) were in stage I, 1 (3.6%) was in stage II, 12 (42.9%) were in stage III, and 2 (7.1%) were in stage IV. Histological types of malignant neoplasms included 1 (3.6%) papillary adenocarcinoma, 1 (3.6%) endometrioid adenocarcinoma, 1 (3.6%) clear cell carcinoma, 1 (3.6%) borderline serous cystadenocarcinoma, 2 (7.1%) adenocarcinomas, 2 (7.1%) mucinous cystoadenocarcinomas, 2 (7.1%) serous cystadenocarcinomas, 8 (28.6%) papillary serous adenocarcinomas, and 9 (32,1%) borderline mucinous cystadenocarcinomas. For benign ovarian neoplasms, the histological types were: 1 (3.6%) serous cystadenoma and Brenner tumor, 2 (7.1%) mucinous cystadenoma and Brenner tumor, 9 (32.1%) mucinous cystadenomas, and 16 (57.1%) serous cystadenomas.
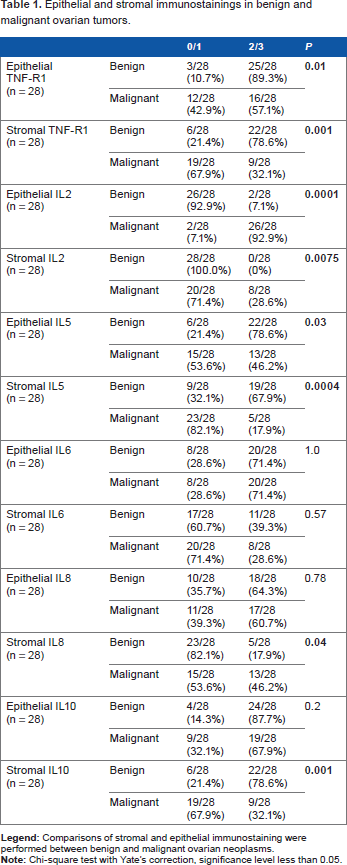
The epithelial and stromal stainings in benign and malignant ovarian tumors are presented in Table 1. Stromal and epithelial TNFR1 and IL-5, and stromal IL-10 had more frequent immunostaining 2/3 in benign neoplasms compared with malignant tumors. Malignant tumors had more frequent immunostaining 2/3 for epithelial and stromal IL-2 in relation to benign tumors. The immunostaining 0/1 of IL-8 was more frequent in the stroma of benign neoplasms compared with malignant neoplasms. No statistical difference was observed in relation to IL-6 cytokine.
Epithelial and stromal immunostainings in benign and malignant ovarian tumors.
Tables 2 and 3 show the relationship between cytokines studied and prognostic factors. In the ovarian cancer stroma evaluation, histological grade 3 was significantly correlated with staining 2/3 for IL-2 (P = 0.004).
Distribution of cytokines with stromal imunostaining 2/3, according to histological grade, staging, metastasis in lymph nodes, chemotherapy response and disease-free survival.

P = 0.004, compared to grade 1/2.
P = 0.03, compared to disease-free survival ≥30 months (Fisher or Chi-square test with Yate's correction).
Distribution of cytokines with epithelium imunostaining 2/3, according to histological grade, staging, metastasis in lymph nodes, chemotherapy response and disease-free survival.

Women whose disease-free survival was less than 2.5 years had TNFR1 stromal staining 2/3 (P = 0.03) more frequently.
Regarding the other cytokines, there was no statistical significance.
Discussion
This study evaluated potential cytokines that can be used as diagnostic and prognostic markers in ovarian cancer. The immune response profile, in which differentiation and proliferation occur in response to the production of certain cytokines, is capable of contributing to the induction of apoptosis and tumor regression control. 19
The ability to intervene and intensify the action of the immune system to produce a beneficial antitumor response remains an area of intense research. The development of cancer may indicate a failure in the immune response, such as a tumor escape mechanism. Tumor cells exhibit a variety of mechanisms that enable them to overcome immunodetection and destruction, making immune responses ineffective. 20
TNFR1 was expressed predominantly in the epithelium and stroma of benign neoplasms, showing strong staining, compared with malignant neoplasms (P = 0.01 for epithelium and P = 0.001 for stroma). By activating proteolytic enzymes such as caspases, TNF-α is capable of triggering a cascade of reactions, culminating in apoptosis of tumor cells.21,22
Most tissues with immunostaining of 2/3 for IL-2 were malignancies. IL-2 stimulates the proliferation and activation of natural killer cells, thus having antitumor activity. 23 Regarding IL-5, immunostaining of 2/3 was more frequent in benign neoplasms in both the epithelium and the stroma. To our knowledge, this is the first study that demonstrates a difference between benign and malignant neoplasms in immunostaining for IL-2 and IL-5, suggesting the important role of these cytokines as targets for future research evaluating new diagnostic markers in ovarian cancer.
Most weak IL-8 immunostaining of tissue stroma was found in benign neoplasms, with scores of 0/1. Regarding IL-10, the stroma of benign neoplasms more frequently demonstrated immunostaining of 2/3 than did that of malignant neoplasms. IL-10 alters the differentiation, maturation, and function of dendritic cells, increasing their spontaneous apoptosis and interfering with the induction of antitumor responses. 24 In normal ovarian cells, IL-10 probably maintains its original autocrine role by inhibiting the secretion of numerous other cytokines, such as IL-1, IL-6, TNF-α, and other growth factors essential for tumor progression and development.15,25,26
When the prognostic factors were evaluated, our study showed weak expression (0/1) of stromal IL-2 in patients with well and moderately differentiated malignancies and a stronger expression (2/3) in poorly differentiated neoplasms. IL-2 aids the growth and differentiation of T- and B-lymphocytes and stimulates growth and maturation of natural killer cells and dendritic cells.27,28 In ovarian cancer, there is no study showing a relationship between IL-2 and prognostic factors. Serum levels of sIL-2R < 522 U/mL, IL-4 < 159 pg/mL, and IL-8 > 339 pg/mL were related to stage I or II invasive colorectal cancer, in which there is no infiltration of the lymph nodes. 29
Women whose disease-free survival was less than 2.5 years had TNFR1 stromal staining 2/3 more frequently. This suggests that strong staining of TNFR1 in a malignant neoplasm may be a poor prognostic factor. The secretion of TNF-α is one of the immune escape mechanisms of the tumor, deviating the immune response toward a Th2 profile. 30 Studies suggest that TNF-α leads to chronic inflammation, angiogenesis, and other processes, which promote the initiation, growth, and spread of the tumor. 31 Many studies have associated inflammation with ovarian tumorigenesis, with TNF-α playing a key role in modulating invasion, angiogenesis, and metastasis.32–34
Antibodies that recognize tumor-associated antigens may help in the pathological diagnosis of cancer and help define the prognosis and detection of recurrent cancer. 20 In particular, it is important to understand whether multiple tumor sites within a given patient have different immunologic microenvironments. Increased heterogeneity in these pathways may reflect underlying differences in stroma biology and inflammatory response intrinsic to the various sites. 35 This could explain the heterogeneous response of cytokine expression profile.
Stromal cells have different gene expression profiles that contribute to the heterogeneity of the tumor. The understanding of their role in tumor development is necessary in the search for new therapies that interfere with carcinogenesis.36,37 The peritumoral stroma can control tumor growth and invasion. This compartment is related to the immune response. The interaction between neoplastic cells and the stroma is a very important factor for tumor growth. 38 Therefore, the stromal compartment has been the subject of studies related to the prognosis of several cancers.
The role of specific cytokines to the development, diagnosis, and prognosis of ovarian cancer is not well known. There are no published studies showing an immunohistochemical panel of cytokines in malignant and benign neoplasms and their correlation with prognostic factors. In the future, we plan to identify a panel of immunohistochemical markers that may help in the prognosis and treatment of ovarian cancer, as treatment currently is restricted to surgery and chemotherapy, with few options for targeted therapies. Our study can be the first step toward the discovery of an immunohistochemical panel in ovarian cancer to determine the likely prognosis and best treatment of the disease, which could be based on targeted therapies related to IL-2 and TNF-α. The peritumoral stroma seems to have a more important role than the epithelium in tumor progression. However, further studies with a larger number of patients are needed. Continued analysis of the relationship between cytokines and ovarian carcinoma might help us to design a novel immunotherapy.
Conclusion
IL-2 and TNFR1 stromal immunostainings are related prognostic factors in ovarian cancer and can be the target of new therapeutic strategies.
Author Contributions
Conceived and designed the experiments: MPJ, AM-F, TPS, EFCM, RSN. Analyzed the data: MPJ, AM-F, EFCM, RSN. Wrote the first draft of the manuscript: MPJ, AM-F, RSN. Contributed to the writing of the manuscript: MPJ, AM-F, EFCM, RSN. Agree with manuscript results and conclusions: MPJ, AM-F, TPS, EFCM, RSN. Jointly developed the structure and arguments for the paper: MPJ, AM-F, EFCM, RSN. Made critical revisions and approved final version: MPJ, AM-F, TPS, EFCM, RSN. All authors reviewed and approved of the final manuscript.
Footnotes
Acknowledgments
The authors wish to acknowledge the funding received from the CNPq (Conselho Nacional de Desenvolvimento Científico e Tecnológico), FUNEPU (Fundação de Ensino e Pesquisa de Uberaba), CAPES (Coordenação de Aperfeiçoamento de Pessoal de Nível Superior), and the FAPEMIG (Fundação de Amparo à Pesquisa do Estado de Minas Gerais).