
Abstract
Objective
To determine the epidemiological and sonographic characteristics of patients with endometrial carcinoma of endometrioid and non-endometrioid subtype to analyse if any differences can be observed between the groups.
Study design
A case-control study was performed considering 122 patients with endometrial carcinoma where 96 (78.69%) had endometrioid carcinomas (controls) and 26 (21.31%) had non-endometrioid carcinomas (cases). Epidemiological, clinical, and sonographic variables (endometrial thickness and sonographic suspicion of myometrial invasion of the tumour) were analysed. Qualitative variables were studied with the Chi-square test and the Fisher's exact test and quantitative variables with the t test. A value of p < 0.05 was considered statistically significant.
Results
Tumours of the non-endometrioid type are observed in older patients (p = 0.003) and frequently show a higher sonographic tumoral invasion (p = 0.0036).
Conclusions
This study supports previous observations that non-endometrioid endometrial carcinomas present at older ages and provides new data that non-endometrioid carcinoma more frequently show sonographic images compatible with myometrial invasion.
Keywords
Introduction
Endometrial carcinoma is the most frequent neoplasia in the female genital tract in developed countries. In Spain, according to The International Agency of Research on Cancer, the endometrial cancer incidence rate adjusted by age to the world's population was 10.24 in 100000 women in 1998 (Eucan, 1998), which means an intermediate rate worldwide.
In 1983, Bokhman (Bokhman, 1983) described two different types of endometrial cancer: Type I, well-differentiated, that appears at early menopause and comprises 70%-80% of the cases; and Type II, typical of elderly stages, less associated to hormonal factors and with an unfavourable prognosis. Later, in 1994, The International Society of Pathologists and Gynaecologists proposed a new classification of endometrial carcinomas depending on their histological type: on the one hand, there are the endometrioid adenocarcinomas with their own variants (villoglandular pattern, secretory, ciliate cells with squamous differentiation and adenoacantoma) and, on the other hand, non-endometrioid carcinomas with their different subtypes (papillary serous, clear cells, mucinous and adenosquamous) (Scully et al. 1994). According to this classification, endometrioid carcinomas are Bokhman's type I (up to 80%) are tumours with a favourable prognosis, occurring in perimenopause, associated to a hyperestrogenic state, that frequently appears after or along with endometrial hyperplasia. In addition to this, Type I carcinomas are less serious, with a high histological differentiation rate and low myometrial invasion. On the contrary, non-endometrioid carcinomas (Bokhman's type II) are a rare histological group with an unfavourable prognosis, typical in elderly stages and not related to hormonal factors. Type II carcinomas are severe and with a low histological differentiation rate and they are characterized by early myometrial invasion.
In the same way, according to what has been published, the pathogenesis of the non-endometrioid types is different from that in endometrioid carcinomas. In the particular case of the papillary serous and clear cell endometrial carcinoma (UPSC), Bokhman states that it does not seem to be associated with risk factors typical of endometrial adenocarcinomas (intrinsic or induced state of non-compensated hyperestrogenism, diabetes, obesity, high blood pressure…) and, different from endometrioid carcinomas, develops over an atrophic endometrium without any previous hyperplasia. Therefore, it seems obvious that there are two different types inside endometrial carcinoma not only in regard to the anatomopathological aspect but also (and maybe overall) to the following:
Patient's characteristics
Pathogenesis
Each histological variant prognosis.
Probably each variant of the tumour should have its own diagnosis and treatment.
Our objective is to describe the characteristics of those patients who have endometrial carcinoma of the endometrioid type and those who have a non-endometrioid carcinoma to determine if there are any differences among them.
Material and Methods
A case-control study was conducted collecting data obtained from those patients diagnosed of endometrial carcinoma. To do so, the clinical records of all endometrial carcinomas diagnosed in Area 2 in Madrid between 1993 and 2005 were revised. In the case group, all endometrial carcinomas of non-endometrioid type (clear cells, papillary serous or adenosquamous) were included, whereas the control group included endometrioid carcinomas. 122 clinical histories of patients with endometrial carcinomas were included. 96 (78.7%) corresponded to endometrioid carcinomas, 12 (9.76%) clear cell carcinomas, 9 (7.34%) were papillary serous and 5 (4.1%) adenosquamous carcinomas. We grouped as cases all non-endometrioid carcinomas, 26 patients (21.3%) whereas the control group was constituted by the 96 endometrioid carcinomas.
According to our institutional protocol for endometrial cancer, an abdominal extrafascial hysterectomy with double adnexectomy followed by pelvic lymphadenectomy was performed. Aortic lymphadenectomy was performed when in selected cases (clear cell or papillary serous histologic subtypes, suspicious nodes, grossly positive adnexa, uterine serosa involvement). The anatomopathological report of the surgical specimens provided diagnosis, histological classification and subtype of endometrial carcinoma. The FIGO staging classification was followed for stadification.
Inside the group of the epidemiological variables and history of the disease, we included the following:
age in years
parity in number of children
the first presenting symptom as methrorrhagia (yes or no)
Menopausal patient's condition expressed as a binary system (yes or no)
Time after the last menstruation expressed in years
Menopause was confirmed in every woman older than 40 years with an amenorrhea period of at least 12 months and a FSH > 20.
Concerning to sonographic variables, the endometrial thickness in millimetres (mm) and sonographic suspicion of tumour myometrial invasion (yes or no) were studied. The sonographic examination in the period of time when the data were collected was performed with two identical monitors Toshiba Eccocee CX- model SSA-340- with a vaginal probe of 7.5 MHz. Likewise, members of the staff performed the ultrasound examination in a systematized way.
The first sonographic parameter considered was endometrial thickness. To determine it, longitudinal planes are taken in the uterus cavity looking for the thickest area by an endometrial scanning from horn to horn. All the endometrium must be included between callipers, which means including endometrial lines of the anterior and posterior sides of the uterus (double line technique).
Then, the suspected myometrial invasion was considered, subjectively assessed by each examiner, taking into account the regularity of the endometrial lining, absence or presence of subendometrial halo, as well as myometrial thickness when invasion occurred.
All these data were retrospectively obtained from the patients’ sonographic video records.
Continuous variables are expressed in terms of median and confidence interval of the mean at 95% (CI 95%) and qualitative variables as number of cases and percentage.
An statistical analysis with Statistical Package for the Social Science (SPSS 12 version) was performed analysing qualitative variables with the Chi-square test and the Fisher's exact test and the quantitative variables with the t test. A value of p < 0.05 was considered statistically significant.
Results
Inside the group of the epidemiological and clinical variables (Table 1), the mean age of patients with non-endometrioid carcinomas was significantly higher than the age in the group with endometrioid carcinomas: 70.63 years (CI 95% 67.1–74.1) compared to 64.8 years (CI 95% 62.3–67.3). No differences were observed between groups concerning parity, presence of bleeding as the initial symptom, menopausal state or time after last menstruation.
Epidemiological and clinical variables.

Data expressed for quantitative variables in terms of mean and confidence interval of the median at 95% (CI 95%) and qualitative variables as number of cases and percentage.
Concerning sonographic variables, significant differences were not found in endometrial thickness sonographically measured in both groups: 19.18 mm (CI 95% 13.8–17.9) for the control group (p = 0.095) (Fig. 1) (Table 2). 7 cases of endometrial carcinomas of less than 4 mm were observed (2 non-endometrioid and 5 endometrioid) (Table 3) in which diagnosis was achieved hysteroscopically because of persistent methrorrhagia.

Box plot of endometrial thickness sonographically measured depending on the anatomopathological carcinoma subtype.
Sonographic variables.

Data expressed for quantitative variables in terms of mean and confidence interval of the median at 95% (CI 95%) and qualitative as number of cases and percentage.
Sonographic variables. Distribution of frequencies of endometrial thickness in carcinomas.

Interestingly, a higher rate of sonographic suspicion of tumour's myometrial invasion was observed in non-endometrioid carcinomas. In this group, tumour invasion was suspected in 6 cases (23.1%) whereas in endometrioid carcinomas only 8 (3.3%) were suspected (p = 0.036) (Table 4).
Anatomopathological variables.
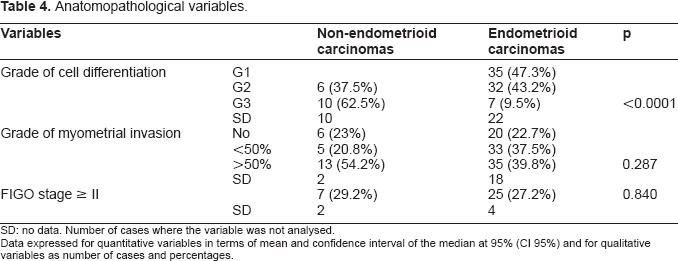
SD: no data. Number of cases where the variable was not analysed.
Data expressed for quantitative variables in terms of mean and confidence interval of the median at 95% (CI 95%) and for qualitative variables as number of cases and percentages.
Discussion
Our analysis on the frequency of the histological subtypes of endometrial carcinomas clearly shows more endometrioid adenocarcinomas, representing 78.7% out of all. In 1989, Fanning (Fanning et al. 1989) performed a retrospective study on the clinical and pathological characteristics of the different subtypes of endometrial carcinomas, revising 418 cases. Similar to our study, endometrioid carcinomas were the more prevalent (82% of the total, similar rate to ours). Considering the histologic subtypes of the non-endometrioid carcinomas, Fanning found 8% of papillary serous –7.34% in our study-, 5% of adenosquamous –4.09% in our study and 3% of clear cells –9.76% in ours-. The distribution of the different anatomopathological varieties is rather similar in both series, except in the clear cell carcinomas, more frequent in ours. Other authors (Fleischer et al. 2002) also report a higher rate of papillary serous than of clear cell carcinomas.
Age is the only of the epidemiological and clinical variables that differs in both groups where the mean age of women with non-endometrioid carcinomas is higher (p = 0.003) in our study. Cirisano (Cirisano et al. 2000) also observed a higher mean age in women with papillary serous and clear cell carcinomas compared with those with endometrioid carcinomas (p = 0.001). Likewise, regardless the type of carcinoma in their patients, they were mainly menopausal, as in our study. These data show that endometrial carcinoma of any histological subtype is a typical disease of the menopause, as a trend of the serious variants to set on later. Finally we did not find any difference between endometrioid and non-endometrioid carcinomas concerning parity, presence of uterine bleeding or menopausal status. Fanning (Fanning et al. 1989) observed a higher rate of nulliparous women in papillary serous carcinomas.
Most endometrial carcinoma diagnoses are made after transvaginal ultrasound in the context of postmenopausal bleeding. Endometrial thickness is the most objective parameter in the endometrial study of postmenopausal bleeding. Most authors agree to perform a histological study on patients with postmenopausal bleeding and endometrial thickness higher than 5 mm (Smith-Bindman et al. 1998; Huertas et al. 2001) although some other authors prefer reducing the cut-off point down to 4 mm to become more sensitive and to reduce the number of false negative (Karlsson et al. 1995; Gull B, 2003). Smith-Bindman (Smith-Bind-man et al. 2004) states that in a postmenopausal woman without vaginal bleeding, if the endometrium measures >11 mm a biopsy should be considered as the risk of cancer is 6.7%, whereas if the endometrium measures < 11 mm a biopsy is not needed as the risk of cancer is extremely low.
Karlsson observed that the mean endometrial thickness in endometrial carcinomas was 21 mm. The most significant fact was the absence of endometrial carcinoma in endometrium thinner than 5 mm. Contrarily, Wang (Wang et al. 2006) found 9 patients (17% in his 52 UPSC series) with endometrium thinner than 5 mm. In our study, we found 7 carcinomas with an endometrial thickness fewer or equal to 4 mm where 5 are in the group of endometrioid carcinomas and 2 in the group of non-endometrioid carcinomas. The difference was not statistically significant. In these cases, the pathologic report identified incipient cases despite the fact that there were misdiagnosed in the sonographic exploration.
The fact that non-endometrioid carcinomas are more serious in their prognosis, made us think that the ultrasound image could be different from the image of the endometrioid carcinomas. We did not find any differences in endometrial thickness between both groups, although the trend is towards a thicker endometrium in non-endometrioid carcinomas. On the other hand, a pattern of higher importance, as is the sonographic endometrial invasion, is present at a higher rate in the family of non-endometrioid carcinomas. Despite the subjectivity of the sonographic diagnosis in myometrial invasion, transvaginal ultrasound is a good tool in the preoperative assessment of myometrial tumoral affection in endometrial carcinomas. The use of colour Doppler and Doppler fluxometry techniques for the study of tumoral vessels would improve the diagnosis and evaluation of myometrial invasion (Fleischer et al. 2002; De Smet et al. 2006).
In conclusion, our study supports the observation that non-endometrioid carcinomas appear more frequently in older patients and more often show sonographic images compatible with myometrial invasion.