
Abstract
Purpose
We conducted a pilot trial to assess the tolerability, clinical benefit and antitumoral efficacy of modified (hydrolysed) citrus pectin (MCP) in 49 patients with various solid tumors in an advanced state of progression. MCP are hydrolysed from polysaccharide pectin fibers, derived from citrus fruits and acting as a ligand for Galectin-3. Preclinical investigations revealed an efficient inhibition of tumor development and metastasis in various tumor models.
Patients and Methods
The treatment consisted of the oral intake of 5 g MCP three times a day. One cycle of therapy was defined as 4 weeks of treatment. Objectives were clinical benefit (pain, functional performance, weight change), safety, tumor response (RESIST criteria) and quality of life (EORTC QLQ30).
Results
49 patients were enrolled, 29 patients were able to be evaluated for clinical benefit after 2 cycles of treatment. All patients tolerated the therapy well without any severe therapy-related adverse events. After 2 cycles of oral intake of MCP, 6/29 patients (20.7%) had an overall clinical benefit response associated with a stabilization or improvement of life quality. On an intent to treat basis 11/49 patients (22,5%) showed a stable disease (SD) after 2 cycles and 6/49 patients (12,3%) had a SD for a period longer than 24 weeks. One patient suffering from metastasized prostate carcinoma showed a 50% decrease in serum PSA level after 16 weeks of treatment associated with a significant increase of clinical benefit, quality of life and decrease in pain.
Conclusion
MCP seems to have positive impacts especially regarding clinical benefit and life quality for patients with far advanced solid tumors. The presented preliminary data encourage us to further investigate the role of MCP in cancer prevention and treatment.
Introduction
Plant fibers derived from fruits contain pectin, highly non-branched complex polysaccharides rich in galactosyl (sugar carbohydrate) residues suggested to have various health promoting properties [1–9]. Ordinary pectin isolated from citrus fruits has a molecular weight of 100.000–200.000 daltons and can be modified via pH, temperature and enzymatic degradation resulting in shorter, less complex molecules. These shorter carbohydrate chains, called modified citrus pectin (MCP), dissolve more readily in water and are better absorbed and utilized by the body than ordinary, long-chain pectin. In the United States of America MCP is registered as a food supplement.
Among other effects, it has been shown that shorter polysaccharide units provide MCP its ability to access and bind tightly to galactose-binding lectins (galectins), especially galectin-3, on the surface of certain types of cancer cells thereby interfering with cancer cell–-cancer cell interaction or cancer cell–-metastatic target site interactions [10–12]. MCP appears to either compete with galectin-3 receptors themselves, or more likely, bind to the galectin-3 receptor sites [11]. Galectin-3 interacts with oncogenic Ras and mediates cell transformation induced by this oncogene [13]. It is involved in the modulation of inflammation processes as well as cell adhesion and cell migration, thus affecting tumor metastasis [14–17]. Moreover, galectins promote angiogenic activity and function as mediators employed by tumor cells to evade the immune response [18]. In vitro, a monoclonal antibody against galectin-3 strongly inhibits experimental lung metastasis of B-16 melanoma and UV-2237 fibrosarcoma cells [19]. Furthermore, in several tumor models a direct correlation between galectin-3 levels and the stage of tumor progression has been shown [20]. Accordingly, in human studies involving colon, stomach, breast and thyroid cancers, the degree of galectin expression is directly correlated with the tumor stage [21–23]. Galectin-3 expression could also be found to correlate with the malignant potential of tumors in the central nervous system [24]. Therefore, galectin-3 may be an attractive target for anti-tumor therapies. MCP also contains Rhamnogalacturonan-II which was shown to be absorbed from the gut into the blood stream and can contribute to the immune enhancement and heavy metal chelation properties of MCP [25].
In vitro, the anti-adhesive properties of MCP were studied in a model utilizing human breast cancer cell lines MCF-7 and T-47D, human prostate adenocarcinoma cells PC-3, human melanoma cells A-375 and human laryngeal epidermoid carcinoma cells Hep-2 [26]. In order to investigate a possible tumor type selectivity growth inhibition in vitro the activity of MCP was evaluated in 19 human tumor xenografts using a clonogenic assay. MCP was effective at the dose of 1 g/l in half of the tumors tested, especially in colon, ovarian and prostate cancer models [10,27]. In vivo studies with MCP using several animal tumor models or human cancer cell lines showed antitumoral efficacies as well as inhibition of tumor metastasis and tumor associated angiogenesis [10–12,27]. Toler-ability studies in mice revealed no toxicity or side effects in terms of body weight loss, lethalness, health condition or behaviour of orally given MCP in a dose range of 3–9 g/kg/day. 9 g/kg/day was the maximum dose that could be administered to the mice within the limits of the formulation concentration [unpublished data].
In a first human study, Strum et al examined the effect of MCP (15 g/d) in seven patients with recurrent prostate cancer [28]. Remarkably, four of seven patients exhibited more than 30-percent lengthening of PSA doubling time implicating a decrease in the cancer growth rate.
The same oncology group then proceeded and conducted a phase II clinical trial evaluating the effects of MCP (Pecta-Sol®) on prostate cancer patients with biochemical relapse after local therapy [29]. 13 patients were evaluated for tolerability and 10 patients for response. PSA was checked monthly for six months prior to starting the trial and on a monthly basis for 12 months. Patients did not receive any other supplements or medical treatments for their prostate cancer for six months prior to the 12 months trial. Trial MCP dosage was 14,4 g/day, in three divided dosages. PSA doubling time (PSADT) increased significantly in 7/10 patients evaluated (70%, p value <0,05). One additional patient had a PSADT increase of over 70%, but was not statistically significant. PSADT increase did not correlate with Gleason score.
Based on preclinical and clinical findings, it appears that MCP might be an interesting option for cancer patients, which merits investigation. Thus, in a first step we decided to perform a pilot study with MCP in patients with advanced solid tumors, for whom no standard therapy is existent or no other promising therapies are available. However, we could not expect any efficient long lasting anti-tumor response for those patients. Therefore, in addition to the clinical response rate we focused on tolerability, life quality and clinical benefit response, which measures the symptomatic improvement based on level of pain, consumption of analgesics, ability to perform daily activities and weight change.
Patients, Materials and Methods
The trial was approved by the local Ethics Committee and carried out in accordance with the German Drug Law and the Declaration of Helsinki. The study began in September 2002 and was finished in December 2003.
Patients
Forty-nine patients with advanced solid tumors were enrolled, for whom no standard therapy was existent or no other promising therapies were available. All the patients included in the study had tumor progression without any change of therapy 2 weeks before study entry. Patients were also required to have a baseline Karnofsky performance status of at least 60% and estimated life expectancy of at least 3 months. In detail, the patients had to fulfil the following criteria: age > 18 years, adequate vital organ function (WBC ≥3.000/μl, platelets ≥100.000/μl, hemoglobin ≥ 10 g/dl, AST and ALT ≤2,5-fold and creatinine ≤ 1,5-fold of the upper limit of this institute's normal range, serum albumin ≤3,5 g/dl), stable pain (Memorial Pain Assessment Card <60 mm, pain intensity stable for at least one week, analgesic consumption unchanged for at least one week). Patients with pregnancy or breastfeeding or similar participation in another clinical trial within the last 4 weeks, cerebral metastasis and accompanying severe disease or disease which could influence the evaluation of the study were excluded. Moreover, patients who complain of reduced food intake due to difficulties in swallowing or prolonged nausea as well as patients who received chemotherapy or radiation in the last 2 weeks or who were operated within 4 weeks before starting the trial were excluded, also. All subjects provided written informed consent, and the protocol of the clinical study was approved by the institutional review board before patient enrolment.
MCP preparation
MCP was supplied as a lyophilized powder by the company “Take Care” CH-Zurich, Switzerland. It was prepared from carefully purified Citrus pectin by means of an enzymatic hydrolysis with food grade enzymes in aqueous solution to obtain the desired molecular weight and degree of esterification below 20%. To maintain a good solubility, the pectin is pH modified by partial neutralisation as Potassium/Sodium salt. The pectin solution is heat treated and dried to obtain MCP in powder form.
Treatment
The treatment consisted of the oral intake of 5 g MCP powder three times a day at 8 hour intervals. The MCP powder was dissolved by mixing it in a small amount of water, then diluting it with a juice of choice. One cycle of therapy was defined as 4 weeks of treatment. The dose was chosen on the basis of pre-clinical animal studies as well as on clinical experience [10,27–29]. Patients profiting clinically could continue the treatment at the same dose and application schedule.
Statistical analysis
This single-arm prospective, open labeled, bi-center pilot study evaluated the effects of an antitumoral therapy with MCP in 49 patients. Only the data of patients who received at least 2 cycles of MCP were analyzed. No statistical hypothesis testing was planned. The data analyses were of an explorative and descriptive nature only.
Trial objectives
The defined objectives were safety, clinical benefit, quality of life and clinical response rate. The trial was not destined to assess any survival benefit.
Safety
All 49 enrolled patients were included in the analysis of safety. Adverse events were evaluated according to the common toxicity criteria (CTC, Version2). Patients were evaluated every 4 weeks by history and physical examination, complete blood counts, chemistry profiles, and urine analysis.
Clinical benefit
Assessment of clinical benefit included the evaluation of the pain status, functional impairment and weight loss before and after 2 and 4 cycles of treatment with MCP [30].
Pain status
Pain status was assessed by a pain intensity score and an analgesic consumption score [31]. Patients participated in a pain stabilization lead-in period to establish base-line measures, then pain intensity was recorded daily (by the patient filling out both an MPAC (Memorial Pain Assessment Card) and an analgesic consumption diary. A positive score was rated as an improvement of ≥20% over baseline in pain intensity or analgesic consumption, a negative score reflects a worsening of pain or an increase of analgesic consumption ≥10% over baseline. Analgesic consumption is expressed in milligram morphine equivalent per day. If either of the two categories was negative, the overall pain classification was negative. If at least one of the two pain categories was positive, the overall pain classification was positive. If both categories were stable, the overall pain classification was stable.
Functional impairment
The functional impairment was assessed weekly by the Karnofsky performance status. A positive score was associated with an improvement of ≥ 10% over baseline, a negative score was associated with a worsening of ≥20% from baseline and a stable score was < 10% improvement and <20% worsening from baseline respectively.
Weight changes
Body weight changes were assessed every 4 weeks and considered a secondary measure.
For patients to achieve an
Quality of life
Psychological parameters assessed in the present study were quality of life (QoL), measured by means of the EORTC-QLQ-C30 questionnaire [32]. Patients had been asked to complete the questionnaire within 24 hours prior to the first medication, at the end of each cycle and/or in case of premature discontinuation. The EORTC-QLQ-C30 is a 30-item questionnaire including five functional scales, three symptom scales, a global health status and six single items. All of the scales and single item measures range from 0 to 100. A high scale score represents a higher response level. Thus a high score for the functional scale represents a high level of functioning, a high score of the global health status/QoL represents a high quality of life, but a high score for symptom scale/item indicates a reduced general condition. The principles for scoring these scales are the same in all cases:
Calculation of the average of the items that contribute to the scale (raw-score-RS).
Linear transformation to 0–100 in order to obtain the score S.
Functional scales: S = (1-[RS-1]/range) × 100
Symptom scales/items: S = ([RS-1]/range) × 100
Global health status/QoL: S = ([RS-1]/range) × 100
Tumor response
Patients were evaluated for response according to the Response Evaluation Criteria In Solid Tumors (RECIST) at baseline as well as for every other course (8 week intervals) by imaging [33].
Results
Patients characteristics
49 Caucasian patients aged between 36 and 82 years with various advanced solid tumors were enrolled in the trial (Table 1). 12 patients with colorectal cancer, 10 patients with prostate carcinoma, 5 patients with breast carcinoma, 4 patients with kidney cancer, 4 patients with pleural or lung cancer, 3 patients with cervix/uterine cancer, 2 patients with liver cancer, 2 patients with pharynx carcinoma and 2 patients with pancreatic cancers, 1 patient each with melanoma, stomach cancer, bile duct carcinoma and chondrosarcoma. 1 patient did not start the trial after recruitment. 89,6% of the patients had metastatic disease. Most were pre-treated with several chemotherapies. 56,3% of the patients had been suffering from cancer for more than 3 years. Altogether 146 cycles (584 weeks) of MCP were administered. The median of cycles was 2,5 [range 0,5–4,5]. 20 patients discontinued the study before the end of course 2 and therefore were not evaluated. The most common reasons were withdrawal of consent (1 patient), lost to follow-up (5 patients) and tumor progression (14 patients).
Patient's characteristics.

Karnofsky performance status.
Pain Intensity.
Safety
One patient with hepatocellular carcinoma had to interrupt the intake of MCP because of increasing pruritus. All other patients tolerated the therapy well without any severe (>grade 2) therapy-related adverse events (Table 2). The most common side effects were pruritus, dyspepsia and flatulence. There were no effects on vital signs or laboratory parameters.
MCP related toxicity.

The symptoms were registered according to the Common Toxicity Criteria (CTC Version 2.0).
(x) number of adverse events related to MCP.
Quality of life
26 of 49 patients were assessable for quality of life evaluation at the end of cycle 2 and 13 patients at the end of cycle 4 (Table 3). The analysis revealed an improvement in physical functioning, role functioning, social functioning, global health status, fatigue, pain, dyspnea, insomnia and appetite loss compared to the baseline. No change could be demonstrated for emotional functioning, cognitive functioning, nausea/vomiting, constipation and diarrhea. Merely, the financial difficulties score shows a slight worsening at the end of cycle 2 but stabilizes at the end of cycle 4.
Evaluation of quality of life–-median scores [range].
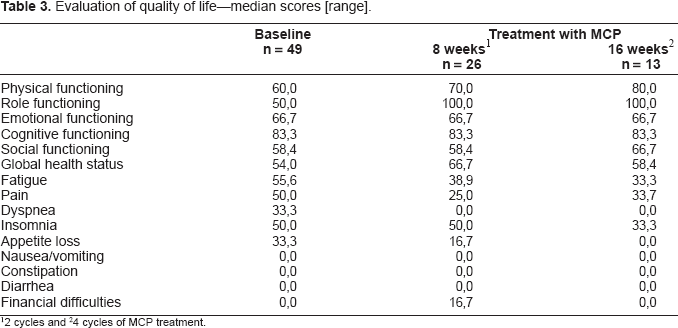
2 cycles
4 cycles of MCP treatment.
Clinical response
The clinical response was evaluated according to the RECIST criteria. Only patients who received at least two cycles of therapy with MCP were considered as assessable for tumor response. 26 of 49 patients could be evaluated. After 2 cycles (8 weeks) of oral intake of MCP 11 patients showed stable disease (SD) and 15 patients had progressive disease (PD). Yet, 10 patients showed SD after 4 cycles (16 weeks) and 6 patients had SD for a period longer than 6 cycles (≥24 weeks).
Remarkably, one patient suffering from advanced metastasized prostate carcinoma and classified as SD according to the RECIST criteria over a period of 9 months showed a 50% decrease in serum PSA level after 16 weeks of treatment associated with a significant increase of clinical benefit, quality of life and decline of pain. No patient exhibited a complete response.
Clinical benefit
17 of the 29 patients receiving MCP at least over a period of 2 cycles could be fully evaluated with regard to pain intensity, performance status and body weight change (Table 4).
Evaluation of the clinical benefit.

measures of pain and performance status.
patient is positive for at least one parameter (pain, performance status or weight) without being negative for any of the others over a period of at least 4 weeks.
Focusing on
Analysis of the
24 of 29 patients could be evaluated for
The evaluation of the
Discussion
Our pilot trial indicates that MCP is a food supplement with favorable properties for patients with far advanced cancer, for whom no other promising antitumoral therapies are available. Pecta-Sol® and Expecting® are two MCP brands in accordance with the specifications of the primary literature. As all patients studied were in a palliative situation, suffering from major syndromes like pain, cachexia, asthenia, malaise, psychological distress, nausea and vomiting, the main goal of our therapeutic intervention was not only to obtain an antitumoral efficacy, but also to improve the quality of life, to preserve physical functioning and well-being as well as to relieve symptoms.
Therefore, in this first step of investigation we focused on tolerability of MCP, life quality and clinical benefit response, which measures the symptomatic improvement based on the level of pain, consumption of analgesics, ability to perform daily activities and weight change. The design of our trial was inspired by previously published data describing the impact of gemcitabine versus 5-floururacil on clinical benefit response (23,8% versus 4,8%) leading to the approval of gemcitabine for the first-line treatment of patients with advanced pancreatic cancer [27]. In this context, it is remarkable, that in our study the treatment with MCP over a period of 8 weeks was associated with an overall clinical benefit response of 20,7% (6 patients out of 29) as well as an improvement of quality of life. However, the high drop out rate of 20 patients already 8 weeks after the start of treatment has to be considered, reflecting the poor clinical condition of most patients entering our trial and compliance issues in advanced disease.
In consideration of the preclinical investigations demonstrating the inhibition of tumor cell spreading rather than a direct antitumoral efficacy, it was not surprising that the treatment with MCP did not induce any objective antitumoral responses in patients suffering from therapy resistant uncontrolled cancer growth and tumor metastasis. However, in consideration of this background, it is remarkable that even 12 (10) out of 49 patients showed a stabilized disease over a period of at least 8 (16) weeks of oral MCP treatment. Moreover, 6 patients had a SD for a period longer than 24 weeks. Furthermore, the 50% decrease of the serum PSA level after 16 weeks of treatment associated with a significant increase of clinical benefit, quality of life and reduction in pain in one patient with far advanced hormone-refractory prostate cancer indicates antitumoral efficacy even in patients with far advanced solid tumors confirming preliminary results from Strum et al. [28] Guess et al. [29].
Despite these encouraging clinical data there are still many unanswered questions concerning, for example, the precise mechanism of action of MCP in patients as well as clearly defined pharmacokinetics to help us better define the optimal biologically active dose. Furthermore, these preliminary results should be confirmed in a more narrowly characterized patient population.
Nevertheless, this is the first Good Clinical Practice (GCP) conform study showing relevant measurable clinical effects of the orally administered natural product MCP in a cancer population of heavily pre-treated patients. This underscores the role of dietary components in cancer progression and metastasis as an emerging field of clinical importance.
Footnotes
Acknowledgments
We are most grateful to Felice Kasper and Barbara Sauer for their critical reading of the manuscript. The staff of the wards Erasmus and the lab of clinical diagnostics are greatly acknowledged. We also thank the corresponding authors of previous articles who provided additional information as required. This clinical trail was supported in part by grants from the Gottfried and Julia Bangerter-Rhyner-Stiftung, the Ehmann-Stiftung and the Stiftung Fürstlicher Kommerzienrat Guido Feger.
All authors were involved in the collection of data for this article and provided intellectual input throughout the project development, analysis, and write-up. The authors had no conflicts of interest.
This clinical trail was sponsored by MCP Forschungsfond, Landquartstraße 3, CH-9320 Arbon, Switzerland and Take Care AG, Würzgrabenstraße 6, CH-8048 Zürich, Switzerland